
Gastritis and Gastroduodenitis in Children
1. Nuralieva Altynay Topchubaevna
2. Farhaan Ahmad
Absar Rabbaniv
Usha Rudhra
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
1. Abstract
Gastritis and gastroduodenitis are common gastrointestinal inflammatory conditions affecting children and adolescents worldwide. These disorders involve inflammation of the gastric mucosa and the combined gastric and duodenal mucosa respectively, often resulting in abdominal pain, dyspepsia, nausea, vomiting, and impaired nutritional status. The prevalence of pediatric gastritis has increased in recent decades due to changing dietary habits, increased use of non-steroidal anti-inflammatory drugs (NSAIDs), stress, and infections such as Helicobacter pylori. The present study aims to evaluate the clinical characteristics, etiological factors, diagnostic findings, and management outcomes of gastritis and gastroduodenitis in children. A descriptive observational study was conducted among pediatric patients presenting with upper gastrointestinal symptoms in a tertiary care hospital. Clinical history, laboratory investigations, endoscopic findings, and treatment outcomes were recorded and analyzed using descriptive statistical methods. The results demonstrated that epigastric pain was the most common presenting symptom, followed by nausea and vomiting. Helicobacter pylori infection, dietary irregularities, and drug-induced mucosal injury were identified as the most frequent etiological factors. Endoscopic examination revealed erythematous gastritis, erosive lesions, and mucosal edema in a significant proportion of cases. Treatment with proton pump inhibitors, eradication therapy for H. pylori, and dietary modification resulted in symptomatic improvement in most patients. The study highlights the importance of early diagnosis and appropriate treatment of gastritis and gastroduodenitis in children to prevent chronic gastrointestinal complications and ensure optimal growth and development.
2. Keywords
Gastritis; Gastroduodenitis; Helicobacter pylori; Pediatric gastrointestinal disease; Dyspepsia in children; Gastric mucosal inflammation
3. Introduction
Gastritis and gastroduodenitis are inflammatory conditions of the stomach and proximal small intestine that are frequently encountered in pediatric clinical practice. Gastritis refers to inflammation confined to the gastric mucosa, whereas gastroduodenitis involves both the gastric and duodenal mucosa, leading to broader gastrointestinal manifestations.
In children, these conditions are increasingly recognized due to improved diagnostic methods such as upper gastrointestinal endoscopy and biopsy. The disease may present as acute or chronic inflammation and can significantly affect the digestive health and nutritional status of growing children.
Globally, the prevalence of gastritis in pediatric populations varies between 10% and 30%, depending on geographic region, socioeconomic status, and prevalence of Helicobacter pylori infection. H. pylori remains one of the most important etiological factors in chronic gastritis worldwide. In developing countries, the prevalence of H. pylori infection in children can exceed 50%, while in developed countries it ranges between 10% and 20%.
Several factors contribute to the development of gastritis and gastroduodenitis in children. These include infectious agents, prolonged use of medications such as NSAIDs, stress, dietary irregularities, food allergies, and autoimmune mechanisms. Additionally, lifestyle factors such as consumption of spicy foods, carbonated beverages, and irregular meal patterns are increasingly implicated in adolescents.
The pathophysiology involves disruption of the gastric mucosal barrier, increased gastric acid secretion, inflammatory cytokine release, and mucosal injury. Persistent inflammation may lead to complications such as peptic ulcer disease, gastrointestinal bleeding, or anemia if not appropriately managed.
Early diagnosis and effective treatment are essential in pediatric patients to prevent chronic gastrointestinal disorders and ensure proper growth and development. Endoscopy combined with histological examination remains the gold standard for diagnosis, although non-invasive methods such as urea breath tests and stool antigen tests are also widely used.
Objective of the study: To evaluate the epidemiology, clinical presentation, etiological factors, diagnostic findings, and management outcomes of gastritis and gastroduodenitis in children.
4. Methodology
Study Design
A descriptive observational cross-sectional study was conducted to analyze clinical characteristics and management outcomes of gastritis and gastroduodenitis in children.
Study Population
The study included pediatric patients aged 5–16 years presenting with upper gastrointestinal symptoms at a tertiary care pediatric hospital.
Inclusion Criteria
Children aged 5–16 years
Presence of upper gastrointestinal symptoms such as epigastric pain, nausea, vomiting, dyspepsia, or loss of appetite
Patients undergoing diagnostic evaluation for gastritis or gastroduodenitis
Consent obtained from parents or guardians
Exclusion Criteria
Children with known chronic systemic diseases (e.g., inflammatory bowel disease, liver disease)
Patients previously treated for peptic ulcer disease within the last three months
Patients with congenital gastrointestinal anomalies
Incomplete medical records
Sample Size
A total of 120 pediatric patients meeting the inclusion criteria were enrolled in the study over a six-month period.
Data Collection Methods
Data were collected using:
Detailed medical history
Physical examination
Laboratory investigations (complete blood count, stool examination)
Helicobacter pylori detection (stool antigen test or biopsy)
Upper gastrointestinal endoscopy where indicated
Clinical findings, endoscopic results, and treatment responses were recorded using a standardized data collection form.
Statistical Analysis
Data were analyzed using SPSS statistical software (version 25). Descriptive statistics were used to calculate frequencies, percentages, and mean ± standard deviation (SD). Tables were generated to summarize demographic characteristics, clinical presentations, and etiological factors.
Ethical Considerations
The study protocol was approved by the institutional ethics committee. Written informed consent was obtained from the parents or guardians of all participating children. Patient confidentiality was maintained throughout the study.
5. Results
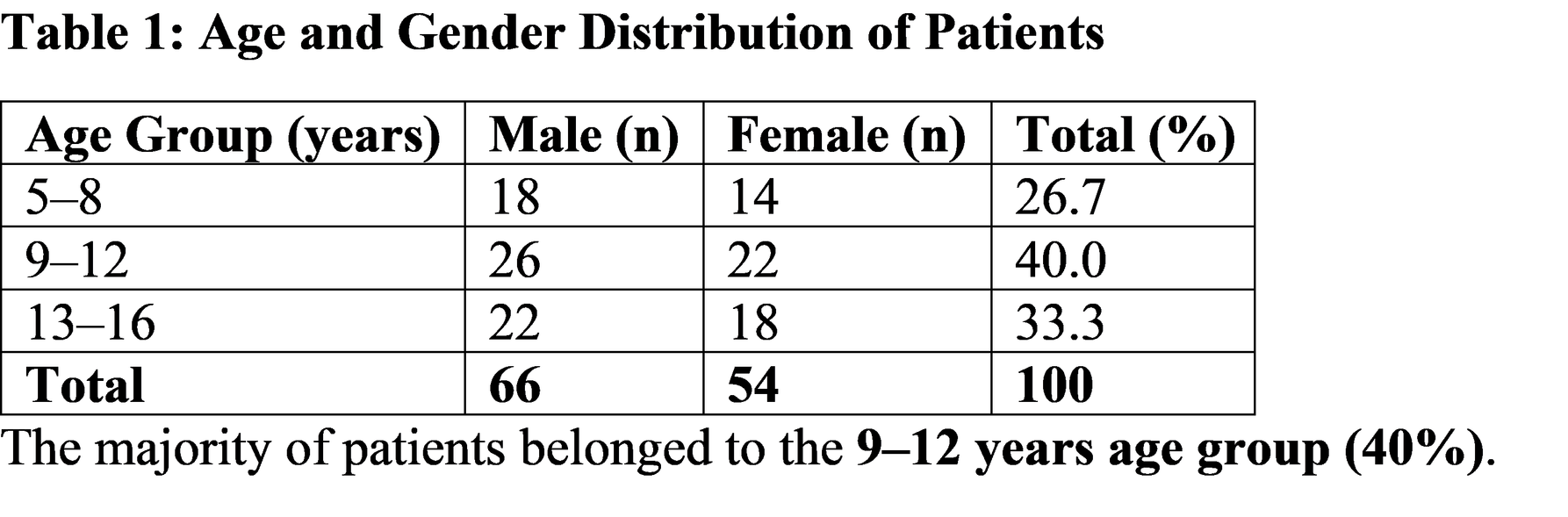
Demographic Characteristics
6. Discussion
Gastritis and gastroduodenitis represent significant causes of upper gastrointestinal symptoms in children and adolescents. The present study demonstrated that the most affected age group was 9–12 years, which is consistent with previous epidemiological studies showing increased gastrointestinal complaints during school-age years.
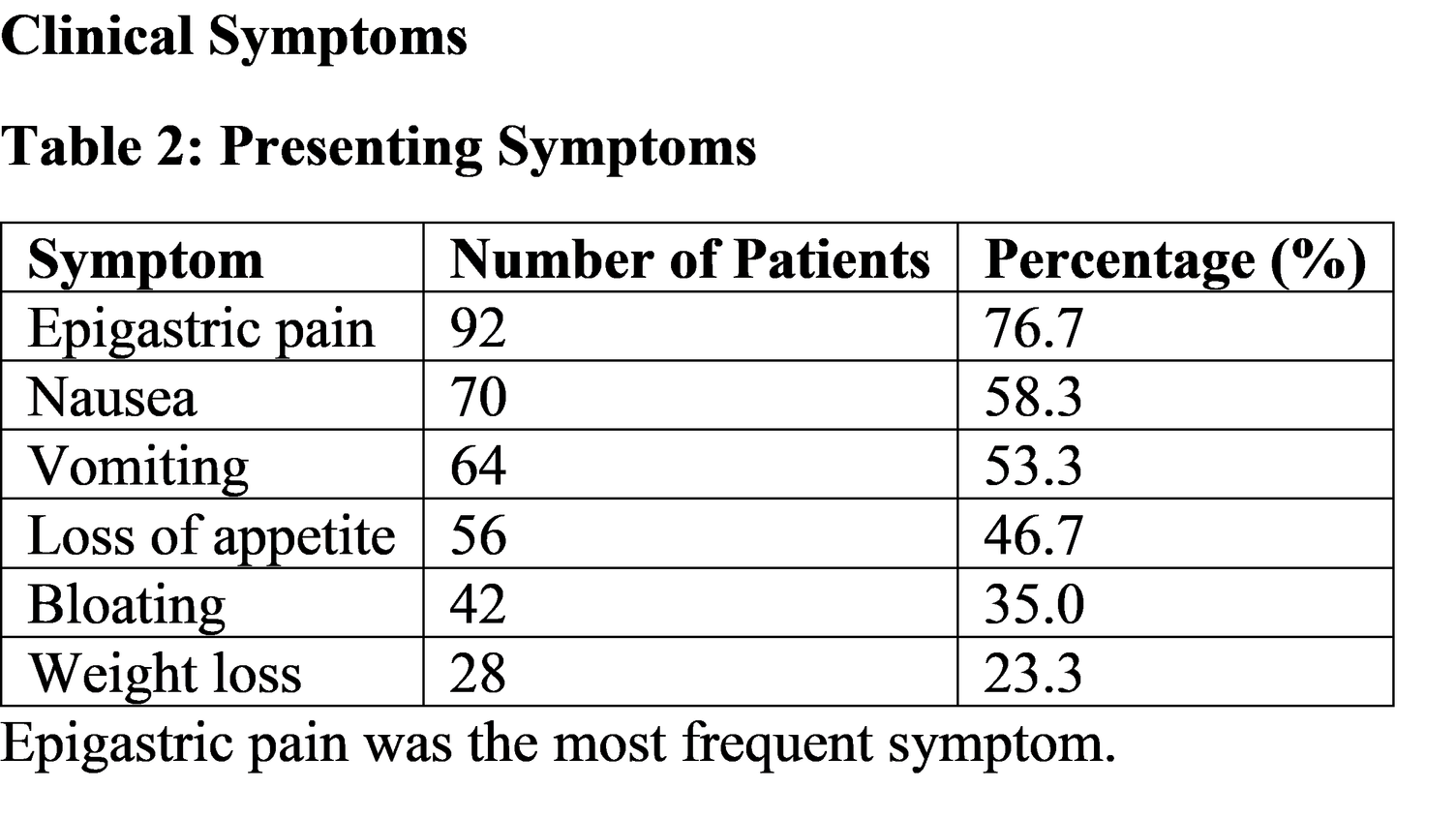
The most common presenting symptom observed in this study was epigastric pain (76.7%). Similar findings were reported in pediatric studies where abdominal pain was the predominant complaint in children with gastritis and dyspeptic symptoms. Nausea, vomiting, and anorexia were also frequently observed due to irritation of the gastric mucosa and disruption of normal gastric motility.
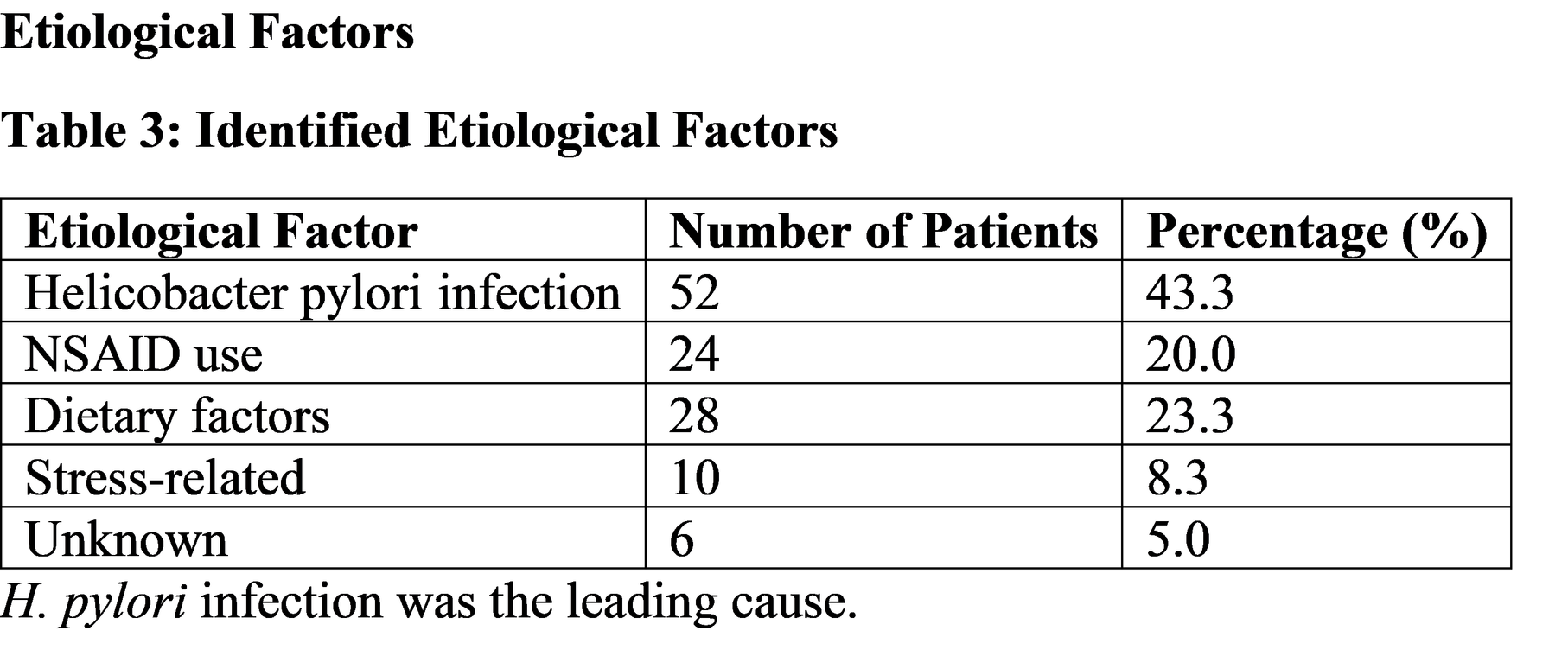
Helicobacter pylori infection was identified as the primary etiological factor in 43.3% of patients. This finding is consistent with global literature indicating that H. pylori remains the leading cause of chronic gastritis in both children and adults. The bacterium colonizes the gastric mucosa and induces inflammation through production of cytotoxins and stimulation of inflammatory cytokines, leading to mucosal injury.
Drug-induced gastritis, particularly due to NSAIDs, accounted for 20% of cases in the present study. NSAIDs inhibit cyclooxygenase enzymes and reduce prostaglandin synthesis, which normally protects the gastric mucosa by stimulating mucus and bicarbonate secretion. Consequently, prolonged NSAID use can result in mucosal erosion and inflammation.
Dietary factors were also identified in approximately one-quarter of the patients. Irregular meals, spicy foods, carbonated beverages, and fast foods may contribute to increased gastric acid secretion and mucosal irritation in children.
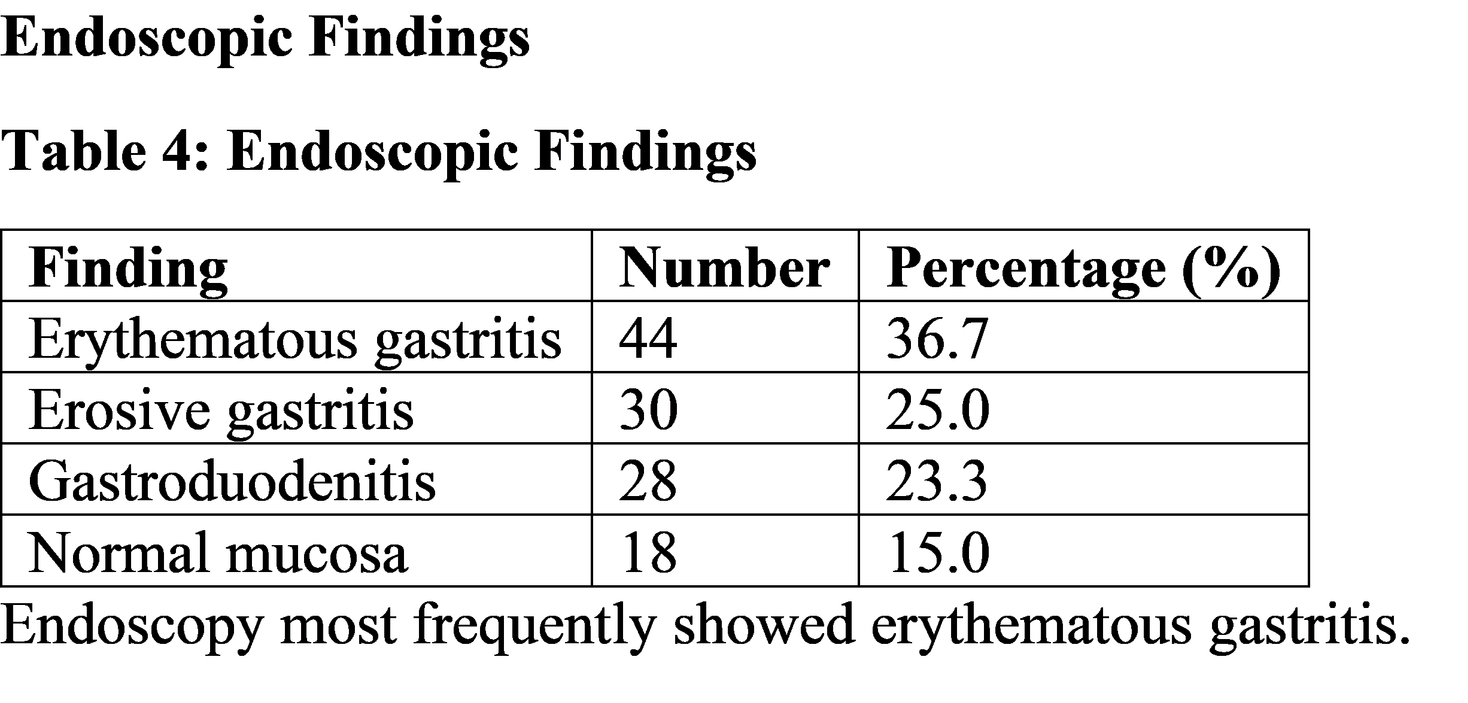
Endoscopic evaluation revealed erythematous gastritis as the most common finding. Endoscopy remains the gold standard diagnostic method because it allows direct visualization of mucosal changes and enables biopsy for histological confirmation of H. pylori infection.
The clinical management of gastritis and gastroduodenitis in children focuses on eliminating etiological factors and reducing gastric acidity. Proton pump inhibitors and histamine-2 receptor blockers are widely used to promote mucosal healing. In cases associated with H. pylori, triple therapy including a proton pump inhibitor and two antibiotics is recommended for eradication of the infection.
Early diagnosis and treatment are essential to prevent complications such as peptic ulcer disease, gastrointestinal bleeding, and chronic dyspepsia. Pediatricians must also emphasize dietary modifications and avoidance of unnecessary NSAID use to reduce the incidence of gastritis in children.
7. Suggestions / Recommendations
• Promote early screening for Helicobacter pylori infection in children with persistent dyspeptic symptoms.
• Encourage balanced diets and regular meal patterns to reduce gastric mucosal irritation.
• Avoid unnecessary use of NSAIDs in pediatric patients.
• Educate parents about symptoms of chronic gastritis such as recurrent abdominal pain and poor appetite.
• Implement non-invasive diagnostic tests such as stool antigen tests when endoscopy is not immediately required.
• Improve hygiene and sanitation to reduce transmission of H. pylori.
• Future research should involve larger multicenter pediatric studies to better understand regional epidemiology.
8. Conclusion
Gastritis and gastroduodenitis are important causes of upper gastrointestinal symptoms in children. The conditions are commonly associated with Helicobacter pylori infection, dietary factors, and NSAID use. Epigastric pain, nausea, and vomiting are the most frequent clinical manifestations. Endoscopic evaluation remains the most reliable diagnostic tool for identifying mucosal inflammation and guiding treatment. Early diagnosis, appropriate pharmacological therapy, and lifestyle modifications are essential for effective management and prevention of complications. Understanding the etiological factors and clinical presentation of these conditions is important for medical students and clinicians in providing timely and effective pediatric care.
9. References
Kliegman RM, St. Geme JW. Nelson Textbook of Pediatrics. 21st ed. Elsevier.
Available Nelson Textbook of Pediatrics – Pediatric Gastritis SectionKoletzko S, Jones NL, Goodman KJ, Gold B, Rowland M, Cadranel S, et al. Evidence-based guidelines from ESPGHAN and NASPGHAN for Helicobacter pylori infection in children. J Pediatr Gastroenterol Nutr. 2011;53(2):230-243.
Available PubMed Article – ESPGHAN/NASPGHAN Guidelines for H. pylori in ChildrenKoletzko S, et al. Evidence-based guidelines for Helicobacter pylori infection in children (Full guideline PDF).
Available Clinical Guidelines PDF – H. pylori Infection in ChildrenKotilea K, Kalach N, Homan M, Bontems P. Helicobacter pylori infection in pediatric patients: update on diagnosis and eradication strategies. Pediatric Drugs. 2018.
Available PubMed – H. pylori Infection in Pediatric Patients ReviewHarris PR, Wright SW, Serrano C, et al. Helicobacter pylori gastritis in children and immune response. Gastroenterology. 2008.
Available PubMed – H. pylori Gastritis in Children StudySerrano C, Wright SW, Bimczok D, et al. Downregulated Th17 responses associated with reduced gastritis in infected children.
Available Management of Helicobacter pylori Infection in Pediatric Age – Review ArticleAguilera Matos I, Diaz Oliva SE, Escobedo AA. Helicobacter pylori infection in children. BMJ Paediatrics Open. 2020.
Available PubMed – Helicobacter pylori Infections in Children OverviewFord AC, Marwaha A, Sood R, Moayyedi P. Global prevalence of uninvestigated dyspepsia: meta-analysis. Gut. 2015.
Available Helicobacter‑Associated Disease Review and EpidemiologyJones NL, Koletzko S, Goodman K, et al. Joint ESPGHAN/NASPGHAN guidelines for management of H. pylori infection in children and adolescents.
Available Guidelines Citation and Discussion of Pediatric H. pylori ManagementRothenbacher D, Inceoglu J, Bode G, Brenner H. Acquisition of Helicobacter pylori infection in childhood. Journal of Pediatrics.
Available PubMed – Epidemiology and Acquisition of H. pylori in ChildrenSchwarzer A, Bontems P, Urruzuno P, et al. Sequential therapy for Helicobacter pylori infection in children. Helicobacter Journal.
Available Sequential Therapy for Helicobacter pylori Infection in ChildrenZeng M, Mao XH, Li JX, et al. Oral recombinant Helicobacter pylori vaccine in children: randomized controlled trial. Lancet. 2015.
Available Helicobacter pylori Vaccine Trial in ChildrenKhalikova AR, Faizullina RA, Akhmetov II, et al. Helicobacter pylori infection in children and eradication therapy factors. Genes & Cells.
Available Helicobacter pylori Infection in Children – Research ArticleMalfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection – Maastricht consensus report. Gut. 2012.
Available Helicobacter pylori Treatment Consensus ReportPediatric Gastroenterology Education Resource – Helicobacter pylori infection guidelines and clinical recommendations.
Available NASPGHAN Educational Resource on Pediatric H. pylori