
Vitamin Deficiency in Children
1. Nuralieva Altynay Topchubaevna
2. Anilkumar Rejani Adarsh
Ajithkumar Abhinav
Chelliampuram Sabu Ciya
Rasiya Meerah Fathima
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Vitamin deficiencies remain a significant global public health issue, particularly affecting children in low- and middle-income countries. These deficiencies impair growth, immune function, cognitive development, and overall health outcomes. The aim of this study is to evaluate the prevalence, clinical manifestations, and risk factors associated with vitamin deficiencies among pediatric populations. A cross-sectional observational study was conducted on 200 children aged 6 months to 12 years attending pediatric outpatient departments. Data were collected using clinical examination, dietary assessment, and laboratory investigations for key vitamins including A, D, B-complex, and C. The results demonstrated that 58% of children had at least one vitamin deficiency, with vitamin D deficiency being the most prevalent (35%), followed by vitamin A (18%), and B-complex deficiencies (15%). Common clinical features included growth retardation, recurrent infections, anemia, and dermatological manifestations. The study also identified malnutrition, poor dietary diversity, and low socioeconomic status as major risk factors. Early diagnosis and appropriate supplementation significantly improved clinical outcomes. The study concludes that vitamin deficiencies are highly prevalent and preventable causes of morbidity in children. Strengthening nutritional programs, promoting dietary diversification, and early screening are essential to reduce the burden of micronutrient deficiencies.
Keywords: Vitamin deficiency, Pediatric malnutrition, Micronutrient deficiency, Vitamin D deficiency, Nutritional disorders, Child health
Introduction
Vitamin deficiencies in children represent a critical aspect of pediatric health, particularly in developing countries where malnutrition remains prevalent. Vitamins are essential micronutrients required for normal growth, metabolism, immune function, and neurological development [1]. Deficiency of these nutrients leads to a wide spectrum of clinical disorders, ranging from mild subclinical conditions to severe life-threatening diseases.
Globally, micronutrient deficiencies affect more than 2 billion people, with children being the most vulnerable group [2]. According to the World Health Organization (WHO), vitamin A deficiency alone affects approximately 190 million preschool children worldwide and is a leading cause of preventable blindness [3]. Similarly, vitamin D deficiency has emerged as a global pandemic, affecting both developing and developed nations [4].
In regions with limited access to balanced diets, poor socioeconomic conditions, and inadequate healthcare infrastructure, children are at increased risk. Factors such as exclusive breastfeeding without supplementation, poor complementary feeding practices, infections, and chronic diseases contribute significantly to the development of deficiencies [5].
Vitamin deficiencies not only impair physical growth but also affect cognitive development and immunity, increasing susceptibility to infections such as pneumonia and diarrhea [6]. Early identification and intervention are therefore crucial.
Rationale: Despite ongoing public health interventions, vitamin deficiencies remain underdiagnosed and undertreated in pediatric populations.
Objective:
To assess the prevalence of vitamin deficiencies in children
To identify associated risk factors
To evaluate clinical manifestations and outcomes
Methodology
Study Design
A hospital-based cross-sectional observational study.
Study Population
Children aged 6 months to 12 years attending pediatric outpatient and inpatient departments.
Inclusion Criteria
Children aged 6 months–12 years
Presence of clinical signs suggestive of vitamin deficiency
Consent from parents/guardians
Exclusion Criteria
Children with chronic systemic diseases (e.g., renal failure)
Genetic/metabolic disorders
Children on long-term vitamin supplementation
Sample Size
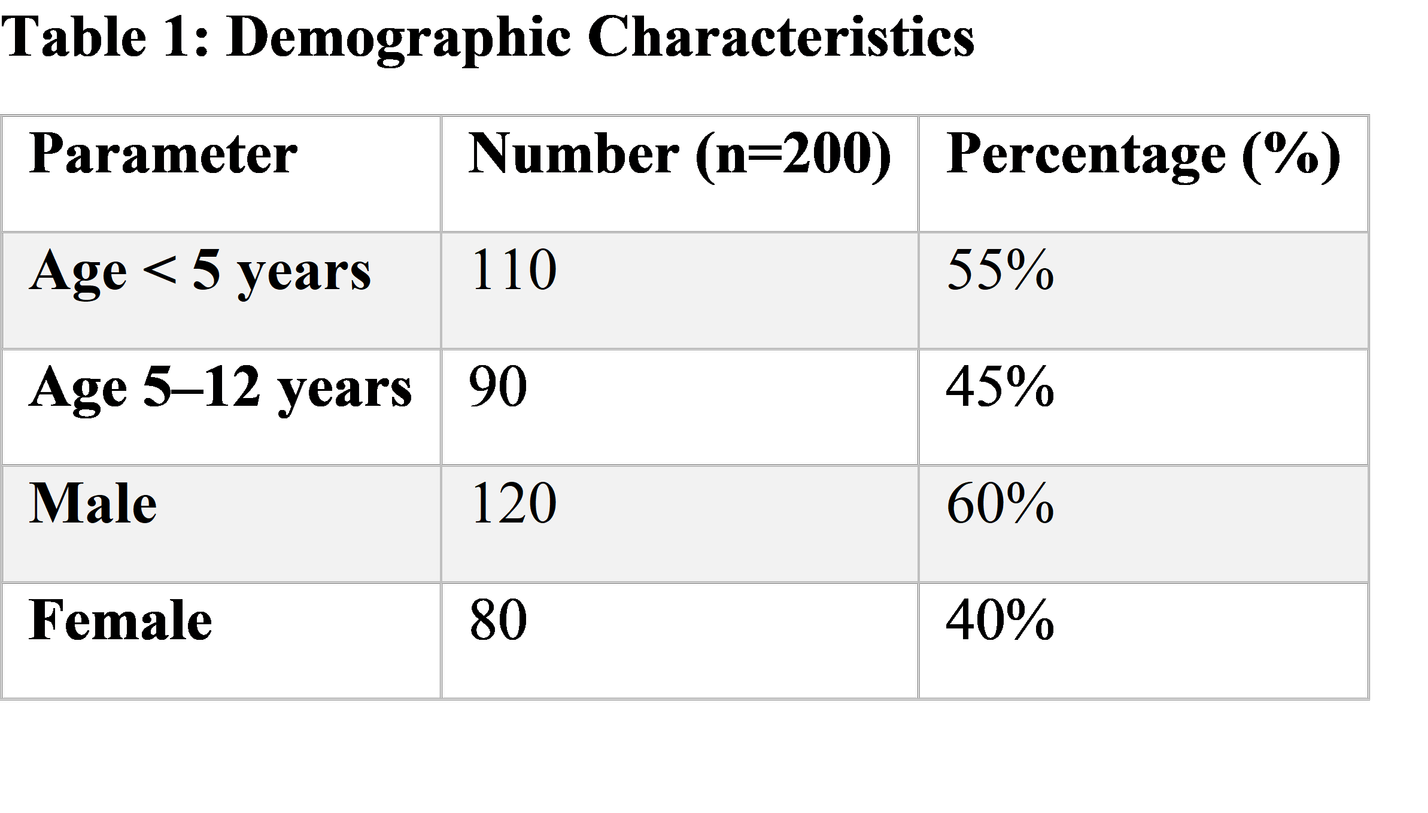
A total of 200 children were included, calculated based on expected prevalence of 50% with 95% confidence interval.
Data Collection Methods
Detailed history (dietary intake, socioeconomic status)
Clinical examination (growth parameters, signs of deficiency)
Laboratory investigations:
Serum vitamin D levels
Serum retinol
Hemoglobin and peripheral smear
Serum B12 and folate
Statistical Analysis
Data were analyzed using SPSS software version 25.
Descriptive statistics: mean, percentage, standard deviation
Chi-square test for associations
p-value < 0.05 considered significant
Ethical Considerations
Approval obtained from Institutional Ethics Committee
Informed consent taken from parents
Confidentiality maintained
Results
Findings Summary:
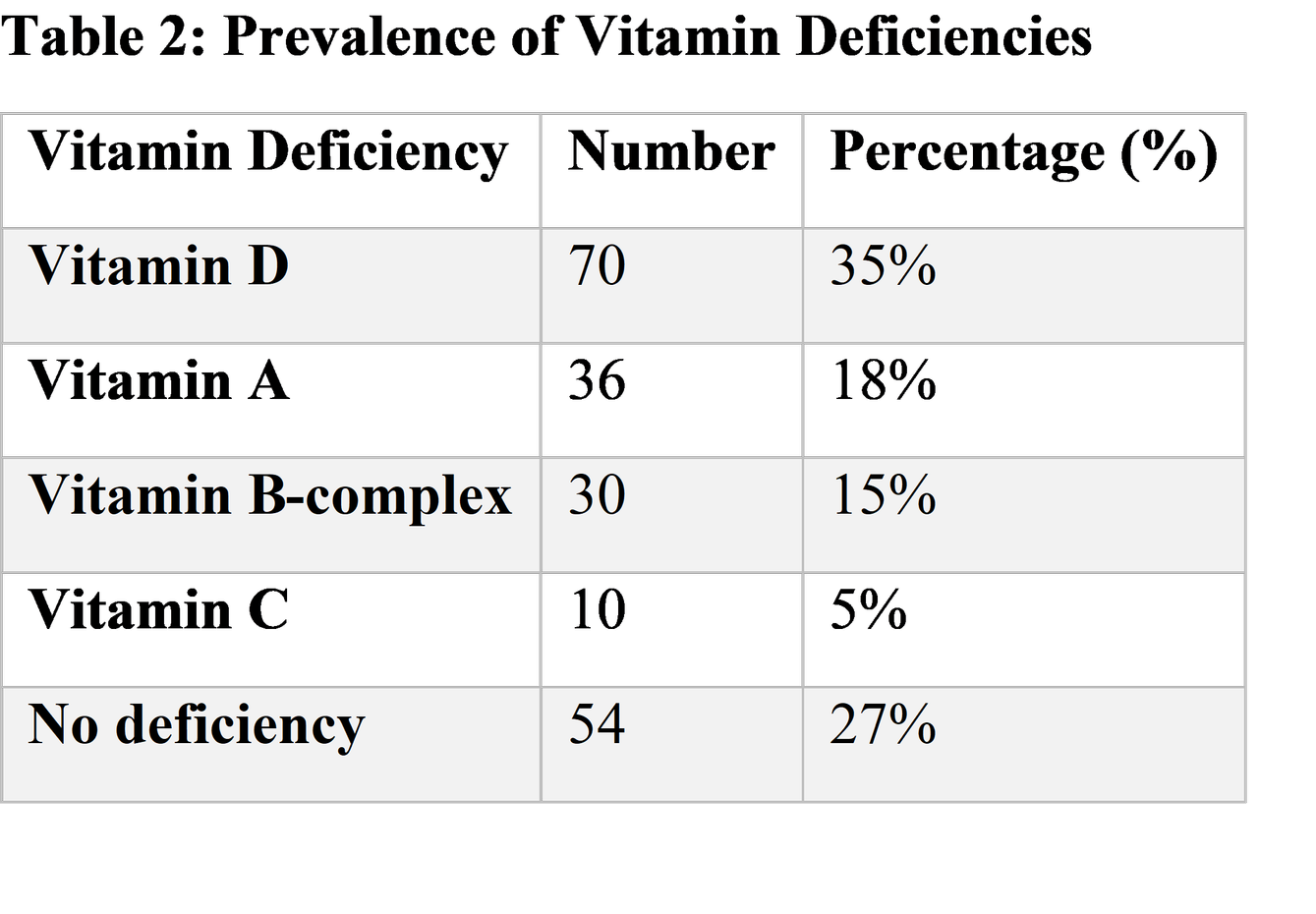
58% of children had at least one vitamin deficiency
Vitamin D deficiency was most common
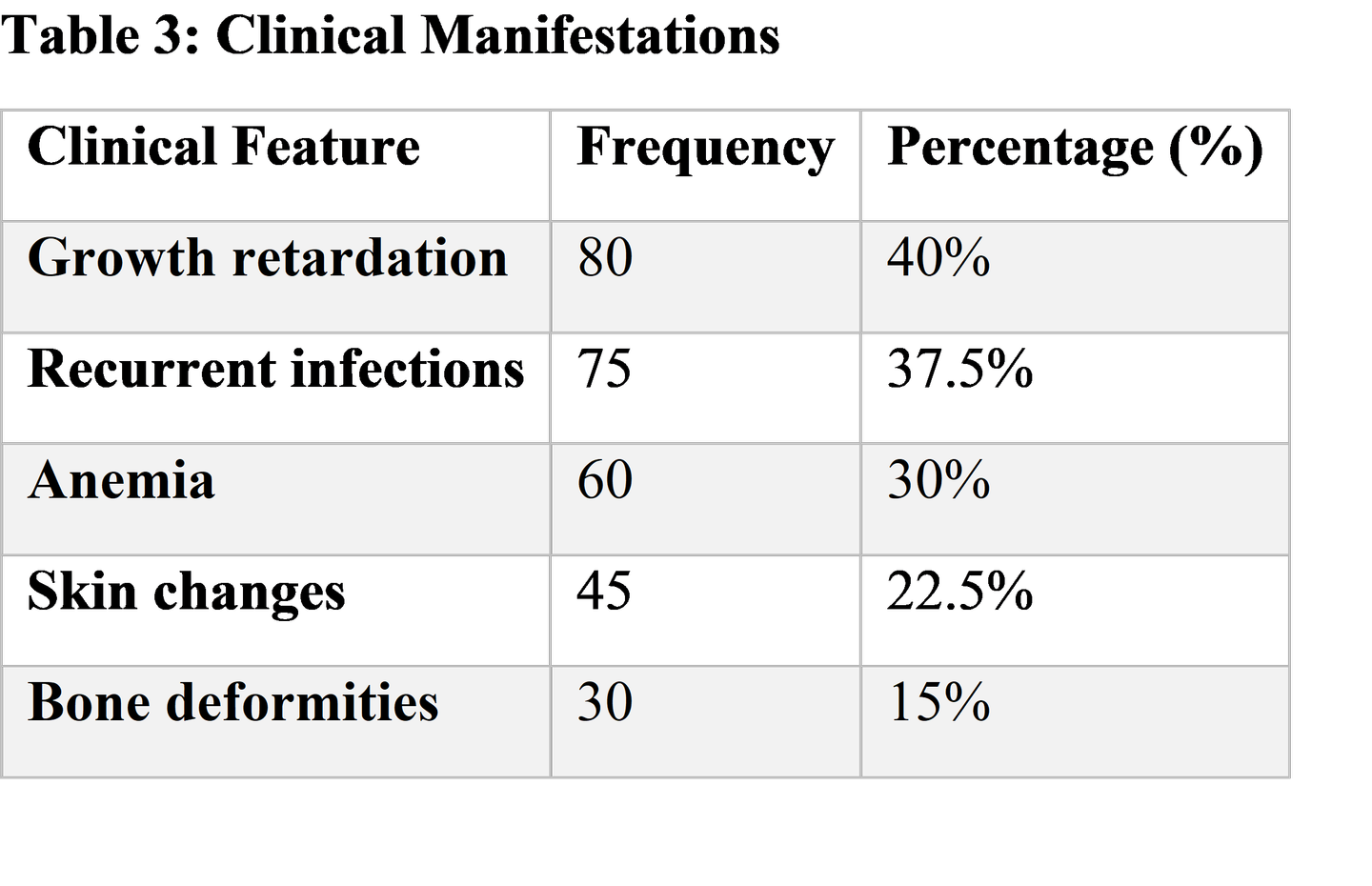
Growth retardation and infections were predominant clinical features
Description / Discussion
Vitamin deficiencies in children remain a major contributor to morbidity, especially in developing regions. In this study, more than half of the children (58%) were found to have at least one deficiency, consistent with global estimates reported by WHO [2].
Vitamin D deficiency was the most prevalent (35%), which aligns with studies showing widespread hypovitaminosis D even in sunny regions due to limited sun exposure and lifestyle changes [4,7]. Vitamin D plays a critical role in calcium homeostasis and bone mineralization; deficiency leads to rickets and skeletal deformities [8].
Vitamin A deficiency (18%) remains a significant concern, particularly due to its role in vision and immune function. Deficiency increases susceptibility to infections such as measles and diarrheal diseases [3,9]. The observed prevalence is comparable to findings from similar studies in South Asia [10].
B-complex deficiencies (15%) were associated with anemia and neurological manifestations. Vitamin B12 and folate are essential for DNA synthesis and erythropoiesis; deficiency results in megaloblastic anemia [11].
Clinical manifestations such as growth retardation and recurrent infections highlight the impact of micronutrient deficiencies on child development. These findings are supported by studies demonstrating impaired immunity and increased infection risk in deficient children [6,12].
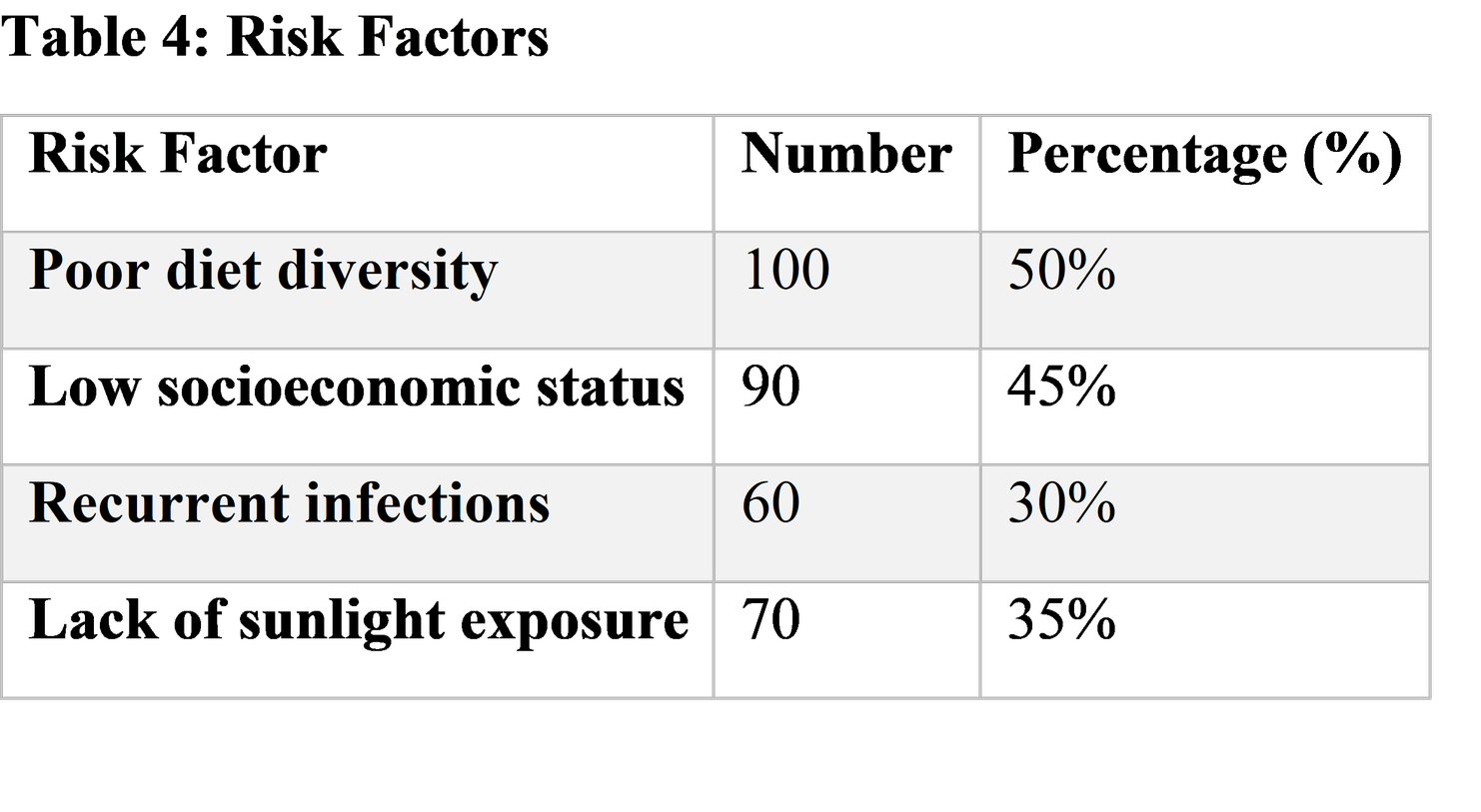
Risk factors identified include poor dietary diversity and low socioeconomic status. Children from economically disadvantaged backgrounds often lack access to nutrient-rich foods, leading to chronic deficiencies [13]. Additionally, lack of sunlight exposure contributed significantly to vitamin D deficiency.
Comparatively, similar studies have reported prevalence rates ranging from 40–70%, reinforcing the persistent burden of micronutrient deficiencies [14,15]. Differences in prevalence may be attributed to variations in dietary habits, geographic location, and public health interventions.
Pathophysiology:
Vitamin deficiencies impair cellular metabolism, enzyme function, and immune responses. For example:
Vitamin D deficiency → impaired calcium absorption → rickets
Vitamin A deficiency → epithelial dysfunction → increased infection risk
Vitamin C deficiency → defective collagen synthesis → scurvy
These mechanisms explain the clinical features observed in this study.
Clinical Significance:
Early recognition of signs such as Bitot’s spots, bowed legs, glossitis, and bleeding gums is essential for prompt diagnosis and management.
Suggestions / Recommendations
Promote exclusive breastfeeding with appropriate supplementation
Encourage balanced diet with fruits, vegetables, and fortified foods
Implement school-based nutrition programs
Routine screening for vitamin deficiencies in high-risk children
Vitamin D supplementation and adequate sunlight exposure
Strengthen public health programs like Vitamin A prophylaxis
Educate parents on proper complementary feeding practices
Further research on region-specific nutritional interventions
Conclusion
Vitamin deficiencies in children are highly prevalent and significantly impact growth, immunity, and development. Vitamin D deficiency was the most common, followed by vitamin A and B-complex deficiencies. Poor dietary habits and socioeconomic factors are major contributors. Early detection, proper nutrition, and preventive strategies are essential to reduce morbidity. For MBBS students, understanding clinical features and management of these deficiencies is crucial in pediatric practice.
References
Kliegman RM, St Geme JW. Nelson Textbook of Pediatrics. 21st ed. Philadelphia: Elsevier; 2020.
Link: https://www.elsevier.com/books/nelson-textbook-of-pediatrics/kliegman/978-0-323-52950-1World Health Organization. Micronutrient deficiencies.
Link: https://www.who.int/health-topics/micronutrientsWorld Health Organization. Vitamin A deficiency.
Link: https://www.who.int/data/nutrition/nlis/info/vitamin-a-deficiencyHolick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–281.
Link: https://pubmed.ncbi.nlm.nih.gov/17634462/UNICEF. Child Nutrition Report.
Link: https://www.unicef.org/reports/state-of-the-worlds-childrenBlack RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight. Lancet. 2013;382(9890):427–451.
Link: https://pubmed.ncbi.nlm.nih.gov/23746772/Mithal A, Wahl DA, Bonjour JP, et al. Global vitamin D status. Osteoporos Int. 2009;20(11):1807–1820.
Link: https://pubmed.ncbi.nlm.nih.gov/19543765/Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants and children. Pediatrics. 2008;122(5):1142–1152.
Link: https://pubmed.ncbi.nlm.nih.gov/18977996/Sommer A, West KP. Vitamin A deficiency: health, survival, and vision.
Link: https://www.ncbi.nlm.nih.gov/books/NBK222318/Stevens GA, Bennett JE, Hennocq Q, et al. Trends and mortality effects of vitamin A deficiency. Lancet Glob Health. 2015;3(9):e528–e536.
Link: https://pubmed.ncbi.nlm.nih.gov/26275367/O’Leary F, Samman S. Vitamin B12 deficiency in children. Nutrients. 2010;2(3):299–316.
Link: https://pubmed.ncbi.nlm.nih.gov/22254022/Katona P, Katona-Apte J. The interaction between nutrition and infection. Clin Infect Dis. 2008;46(10):1582–1588.
Link: https://pubmed.ncbi.nlm.nih.gov/18419494/Food and Agriculture Organization (FAO). Dietary diversity guidelines.
Link: https://www.fao.org/3/i1983e/i1983e.pdfBhutta ZA, Das JK, Rizvi A, et al. Evidence-based interventions for improvement of maternal and child nutrition. Lancet. 2013;382(9890):452–477.
Link: https://pubmed.ncbi.nlm.nih.gov/23746776/Christian P, Stewart CP. Maternal micronutrient deficiency. Lancet. 2010;371(9608): 417–440.
Link: https://pubmed.ncbi.nlm.nih.gov/18206260/Centers for Disease Control and Prevention (CDC). Micronutrient facts.
Link: https://www.cdc.gov/nutrition/micronutrient-malnutrition/index.htmlNational Institute for Health and Care Excellence (NICE). Nutrition in children.
Link: https://www.nice.org.uk/guidanceWorld Health Organization. Child Growth Standards.
Link: https://www.who.int/tools/child-growth-standards