
Hospital-Based Evaluation and Management of Radiation Syndrome
1. Samatbek Turdaliev
2. Muruganathan Boovaneshwaran
Lina Abdul Latheef
(1. Teacher, International Medical Faculty, Osh State University, Kyrgyz Republic)
(2. Students, International Medical Faculty, Osh State University, Kyrgyz Republic)
ABSTRACT:
Radiation syndrome, also known as acute radiation syndrome (ARS), is a constellation of systemic effects that occur after exposure to high doses of ionizing radiation over a short period. The severity of the condition depends on the radiation dose, rate of exposure, and tissues involved. ARS typically progresses through four phases—prodromal, latent, manifest illness, and either recovery or death—and presents with gastrointestinal, hematopoietic, neurovascular, and cutaneous manifestations. Early identification of exposure level and organ system involvement is crucial for prognosis and timely management, which includes supportive care, hematopoietic growth factors, infection control, and in severe cases, stem cell transplantation. Understanding the pathophysiology and clinical course of radiation syndrome is essential for medical preparedness in nuclear accidents, radiologic emergencies, and potential radiologic terrorism scenarios.
Keywords: Radiation syndrome, ionizing radiation, organ system, exposure expanded newborn screening, improved healthcare access, and continued research into safe, widely accessible curative treatments.
INTRODUCTION:
Radiation syndrome, commonly referred to as acute radiation syndrome (ARS), encompasses the clinical consequences that arise following exposure to a significant dose of ionizing radiation delivered over a short duration. Ionizing radiation has the capacity to damage cellular DNA, disrupt normal tissue function, and trigger widespread systemic effects. Although low-level radiation is routinely encountered in medical imaging and environmental sources without causing harm, high-dose exposures—such as those occurring in nuclear accidents, radiologic emergencies, or unshielded industrial sources—can overwhelm the body’s repair mechanisms. ARS manifests as a predictable sequence of symptoms involving rapidly dividing tissues, most notably the bone marrow, gastrointestinal tract, and neurovascular system. The severity and pattern of illness are determined primarily by the absorbed radiation dose, dose rate, and extent of exposure. Because ARS can progress rapidly to life-threatening complications, early recognition and timely intervention are essential. Understanding the mechanisms, clinical course, and management strategies of radiation syndrome is crucial for healthcare professionals, particularly in the context of increasing global emphasis on radiation safety and disaster preparedness1.
ETIOLOGY:
Acute radiation syndrome can result from direct exposure or contamination by radioactive materials. Direct exposure can be caused by a nuclear blast, while contamination can result from the ingestion of nuclear-contaminated food, water, and skin contact with the nuclear material. Acute radiation syndrome is divided into 3 groups: hematopoietic, gastrointestinal, and cardiac/neurological systems. Each system will require a different dose of radiation to manifest the symptoms of acute radiation syndrome2. The timing of symptoms is also subdivided into prodrome, latent, and manifest phases. The dose, symptom onset, and acute radiation syndrome subdivision are below3.
EPIDEMIOLOGY:
Radiological or nuclear emergencies are rare but can involve significant numbers of people. After the Chornobyl nuclear power plant disaster in 1986, nearly 6000 children developed thyroid cancer. Radioactive iodine that was either inhaled or consumed from local contamination caused this cancer4. Immediately after an accident, local health facilities will be overwhelmed with people wanting to be screened and treated. Areas with local nuclear power plants need to plan accordingly. Major cities now have to worry about the possibility of a dirty bomb5.
PATHOPHYSIOLOGY:
Radiation is detrimental to body tissues based on how quickly their cells turn over. Those with a high mitotic index will be more severely affected at a lower dose. These include bone marrow, the gastrointestinal tract, and skin6.
EVALUATION:
All patients with nuclear or radiation exposure should have a baseline complete blood cell count (CBC) with a differential, blood type and screen, and electrolytes. A CBC should be repeated every 6 to 12 hours so as to be able to monitor the white cell count depletion if any. Lymphocyte depletion kinetics are the best predictor of radiation exposure and clinical outcome. Mucosal surface swabs for radiation should be sent to the appropriate labs. Make every effort to document all baseline labs appropriately, as they can help determine future therapies. All baseline radiation levels should be taken before and after decontamination7.
TREATMENT:
The staff must be protected from contamination, and all patients with a history of contamination should be disrobed and bathed. You can decrease exposure by 80% just by removing any contaminated clothing. Those individuals with life-threatening injuries are decontaminated as well as possible, but surgical and trauma emergencies will have priority. Surgery should be done within the first 24 hours as significant changes in the patient's ability to fight infection can result from radiation exposure. Supportive care saves lives when it comes to acute radiation syndrome. Fluid management and early treatment of any signs of infection will be fundamental to a better outcome. Prevention of thyroid cancer must be a priority. All children and pregnant women must be offered potassium iodide to protect the thyroid from the uptake of radioactive iodine. Mothers who are breastfeeding should be encouraged to stop if possible. The following potassium iodide doses should be used daily while in the area of exposure: adult 130 mg, child 65 mg, and infants 1 month to child 3 years old 32 mg. This is especially important in the case of nuclear power plant accidents. Anti-emetics will be helpful to control nausea. Pain control for burns and other injuries should be a priority. In moderate exposures, it may be necessary to use cytokines and colony-stimulating factors. Early use of antibiotics should be the rule. The use of bone marrow transplant has been used for large dose exposures but remains controversial. Chelating agents are used in some exposures but should be started only after consultation with a nuclear specialist (see Resources). Keep in mind the psychological trauma that can result from radiation exposure. This trauma is more pronounced in children as they will be displaced from their homes and routines8.
DIFFERENTIAL DIAGNOSIS:
The differential diagnosis for radiation toxicity includes the following:
Acute gastric dilation
Acetaminophen toxicity
Adrenal insufficiency
Appendicitis
Aspirin toxicity
Central nervous system tumor
Digoxin toxicity
Elevated intracranial pressure
Pancreatitis
Peritonitis
Research:
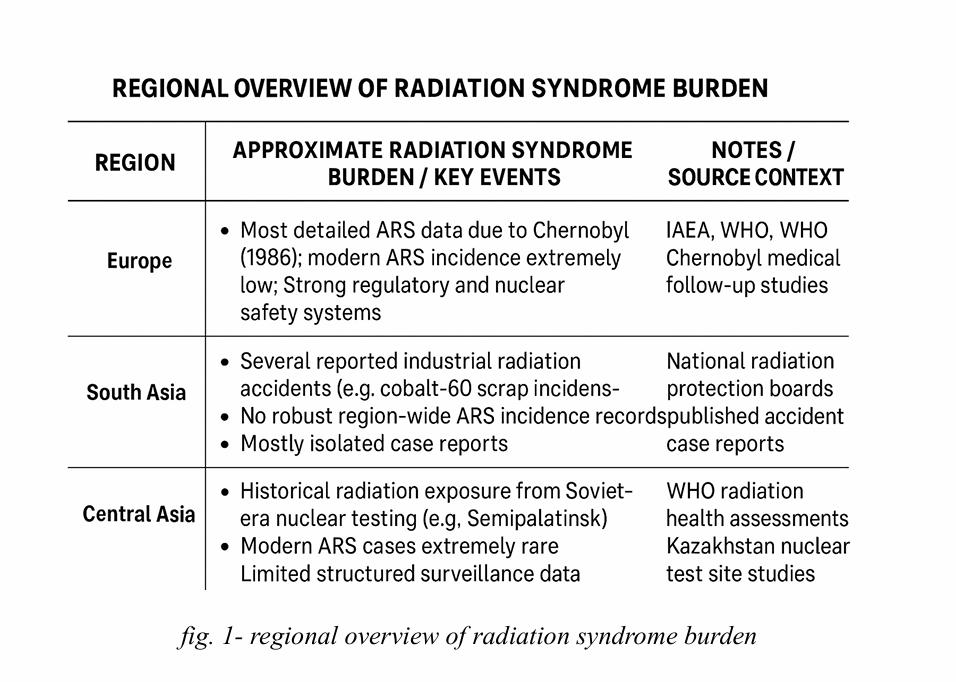
• Estimated Incidence of Acute Radiation Syndrome (ARS)
• Acute radiation syndrome is rare and typically occurs only after significant exposure to ionizing radiation. Estimated global incidence is very low and mostly linked to nuclear accidents, industrial radiation mishaps, or radiation-related disasters. fig. 1- regional overview of radiation syndrome burden
• Major historical data points show the highest case clusters from Chernobyl, Fukushima, Goiania, and Tokaimura accidents.
• In routine healthcare settings, ARS incidence is 10–20 Gy) and is universally fatal. In reported radiation-accident cohorts, 60–80% of patients show hematopoietic involvement with lymphocyte depletion. • Mortality and Progression
• Without treatment, moderate to severe ARS can have mortality rates up to 50–90%, depending on dose.
• With modern care (growth factors, antibiotics, transfusions), survival improves significantly for patients exposed to <6-7 Gy
• Severe GI or neurovascular involvement remains associated with very high fatality despite supportive care.
• Diagnostic Delay and Challenges
• Early symptoms (nausea, vomiting, fatigue) are nonspecific, leading to frequent delays in recognizing radiation exposure.
• In many radiation accidents, diagnosis was made hours to days later, often after blood counts declined.
• Lack of immediate dose-estimation tools contributes to delayed triage and treatment.
REFERENCE:
1. Qutob SS, O'Brien M, Feder K, McNamee J, Guay M, Than J. Prevalence of laser beam exposure and associated injuries. Health Rep. 2019 Jan 16;30(1):3-9.
2. MacVittie TJ, Farese AM, Parker GA, Jackson W, Booth C, Tudor GL, Hankey KG, Potten CS. The Gastrointestinal Subsyndrome of the Acute Radiation Syndrome in Rhesus Macaques: A Systematic Review of the Lethal Dose-response Relationship With and Without Medical Management. Health Phys. 2019 Mar;116(3):305-338.
3. Barbati ME, Gombert A, Schleimer K, Kotelis D, Wittens CHA, Bruners P, Jalaie H. Assessing radiation exposure to patients during endovascular treatment of chronic venous obstruction. J Vasc Surg Venous Lymphat Disord. 2019 May;7(3):392-398.
4. Sushko VO, Kolosynska OO, Tatarenko OM, Nezgovorova GA, Berestjana ZM, Ustinov SI, Hapeyenko DD. Probl Radiac Med Radiobiol. 2018 Dec;23:471-480.
5. Bazyka OD, Bilyi DO. DISEASES OF CIRCULATORY SYSTEM AND COMORBID TYPE II DIABETES MELLITUS IN THE CHORNOBYL ACCIDENT CONSEQUENCES CLEAN-UP WORKERS. Probl Radiac Med Radiobiol. 2018 Dec;23:246-253.
6. Chobotko HM, Raichuk LA, Landin VP.). Probl Radiac Med Radiobiol. 2018 Dec;23:216-228.
7. MacVittie TJ, Farese AM, Parker GA, Jackson W. The Time Course of Radiation-induced Lung Injury in a Nonhuman Primate Model of Partial-body Irradiation With Minimal Bone Marrow Sparing: Clinical and Radiographic Evidence and the Effect of Neupogen Administration. Health Phys. 2019 Mar;116(3):366-382.
8. Story MD, Durante M. Radiogenomics. Med Phys. 2018 Nov;45(11):e1111-e1122.