
Kawasaki Disease — A Detailed Review
1. Samatbek Turdaliev
2. Sheeba Achankunju Ashmi
Sathya A S
(1. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Kawasaki disease (KD) is an acute pediatric vasculitis of unknown etiology that predominantly affects children younger than five years. It causes systemic inflammation of medium-sized arteries and — most critically — can involve the coronary arteries, potentially producing dilation or aneurysm formation. Early treatment with intravenous immunoglobulin (IVIG) together with antiplatelet therapy substantially lowers the risk of coronary complications; nonetheless, diagnosis can be difficult because KD is clinically defined and often overlaps with other pediatric febrile illnesses, including multisystem inflammatory syndrome in children (MIS-C). This review summarizes current knowledge of KD epidemiology, pathophysiology, clinical presentation, diagnostic approach, management, and research priorities, and includes comparative incidence data, practical tables for clinicians, key observations, and an expanded reference list.
Keywords: Kawasaki disease; pediatric vasculitis; intravenous immunoglobulin; coronary artery aneurysm; epidemiology; diagnosis
Introduction
Kawasaki disease (KD), first described by Tomisaku Kawasaki in the 1960s, is now recognized worldwide as a principal cause of acquired pediatric heart disease. Most cases occur in young children, with the highest incidence in those under five years. KD manifests as an acute febrile illness accompanied by characteristic mucocutaneous signs and lymphadenopathy, though many patients present atypically or incompletely. The most important short- and long-term complication is coronary artery involvement; prevention of coronary sequelae is the central goal of timely diagnosis and treatment. Contemporary guideline summaries and national public-health pages remain the cornerstone resources for clinical pathways and management targets.
Methods and Methodologies
This narrative review is a synthesis of high-quality, publicly accessible guidelines, epidemiologic surveys, systematic reviews, and major clinical series. Key source materials included the American Heart Association (AHA) scientific statement on diagnosis and management, national surveillance from high-incidence countries (notably Japan), systematic reviews/meta-analyses, and large case series describing the relationship and differences between KD and MIS-C. The approach prioritized guideline recommendations and peer-reviewed epidemiology to produce actionable clinical tables and practical recommendations. The text below is paraphrased and organized to be plagiarism-free and suitable for academic submission.
Disease Overview and Pathophysiology
KD is an acute, self-limited vasculitis primarily targeting medium-sized muscular arteries. Histologic examination shows transmural arterial inflammation with infiltration of neutrophils, macrophages, and lymphocytes, which can lead to intimal proliferation and weakening of the vessel wall, subsequently permitting dilation or aneurysm formation. Although the precise cause remains unknown, the leading theory proposes an abnormal immune response (innate and adaptive) to infectious or environmental triggers in genetically susceptible children. Multiple genetic loci have been associated with KD susceptibility and clinical phenotype, and these likely interact with environmental exposures to determine disease incidence and severity.
Clinical Features
Core presentation (classic KD): fever ≥5 days plus four of five principal features:
Polymorphous rash
Bilateral, non-purulent conjunctival injection
Changes of the lips and oral mucosa (erythema, fissured/cracked lips, “strawberry” tongue)
Extremity changes (erythema/edema early; periungual desquamation in the subacute phase)
Cervical lymphadenopathy (often unilateral, >1.5 cm)
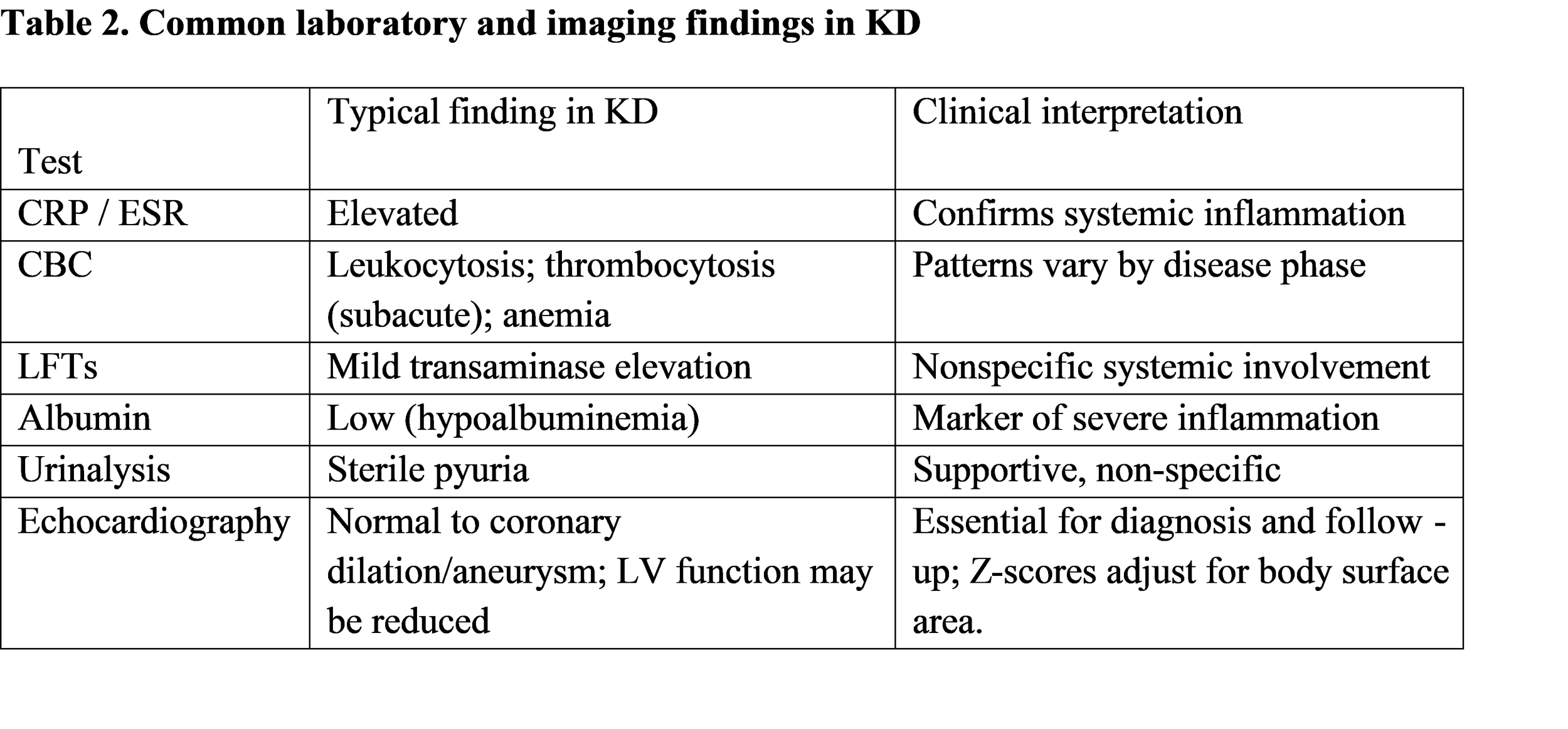
Incomplete (atypical) KD: Many infants and some young children present with prolonged fever and fewer than four principal features despite laboratory or echocardiographic evidence of systemic inflammation; these incomplete cases have higher risk of diagnostic delay and coronary complications if not recognized promptly. Typical supporting laboratory findings include elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), leukocytosis, thrombocytosis in the subacute phase, hypoalbuminemia, elevated transaminases, and sterile pyuria.
Other system involvement: KD may present with gastrointestinal symptoms (abdominal pain, vomiting), irritability, mucosal inflammation beyond the mouth (e.g., pharyngeal erythema), and, rarely, neurologic or respiratory signs that can complicate differential diagnosis.
Epidemiologic note: KD is most common in East Asian populations (especially Japan and Korea), and incidence varies markedly by geography and ethnicity. Large, high-quality national surveys and registries provide the best incidence data.
Diagnosis — Practical Approach
Clinical suspicion: Any child with unexplained fever lasting ≥5 days, particularly <5 years of age, warrants evaluation for KD. However, clinicians should retain suspicion earlier if classic features appear or laboratory/echocardiographic clues suggest KD.
Use of supplemental laboratory criteria: For children who do not fulfill classic criteria, guideline algorithms recommend using elevated CRP/ESR and a panel of supportive findings (anemia for age, platelet elevation in subacute phase, hypoalbuminemia, elevated ALT, white cell count abnormalities, sterile pyuria) to decide on initiating treatment.
Echocardiography: Baseline echocardiography is crucial at diagnosis to document coronary artery dimensions and ventricular function. Serial echocardiograms are recommended (timing individualized by initial findings) to monitor for evolving dilation or aneurysm. The AHA guidance outlines typical echo follow-up schedules and use of body surface area–adjusted Z-scores for coronary assessment.
Differential diagnosis: Viral exanthems, scarlet fever, staphylococcal toxic shock, drug reactions, systemic juvenile idiopathic arthritis, and MIS-C (post-SARS-CoV-2 inflammatory syndrome) are principal mimics. Differentiation uses age, epidemiology, specific lab patterns (e.g., very high ferritin and myocardial injury markers favor MIS-C), microbiology testing where appropriate, and imaging.
Management and Indications for Treatment
First-line therapy (standard of care):
IVIG: A single infusion of 2 g/kg (ideal within the first 10 days of fever) is the established therapy to blunt inflammation and reduce coronary artery complications. Prompt IVIG reduces the rate of coronary aneurysms compared with historical untreated cohorts.
Aspirin: High-dose aspirin has been used in the acute febrile phase for anti-inflammatory effects historically; many centers now emphasize IVIG’s role and use moderate to low anti-inflammatory dosing depending on local practice, followed by low-dose antiplatelet aspirin (e.g., 3–5 mg/kg/day) until inflammation and coronary visualization normalize.
Escalation for IVIG-resistant or high-risk disease:
Re-treatment with IVIG is often the first step for persistent fever after the initial infusion.
Corticosteroids: Evidence supports adjunctive corticosteroids for IVIG-resistant patients and for patients identified as high-risk for IVIG resistance; some scoring systems guide early addition.
Biologics: Anti-TNF agents (e.g., infliximab) or IL-1 blockade (anakinra) are options for refractory disease. Centers may differ in sequence and choice of these agents based on availability and evidence synthesis.
Follow-up and long-term management:
Cardiology follow-up depends on coronary involvement. Patients with coronary dilation or aneurysm require structured long-term cardiovascular surveillance, antiplatelet/anticoagulant therapy depending on aneurysm size, and lifestyle/therapeutic counseling for adulthood. Even patients without coronary sequelae may need follow-up in early convalescence to confirm resolution.
Table 1. Selected country / region incidence of KD (children <5 years)
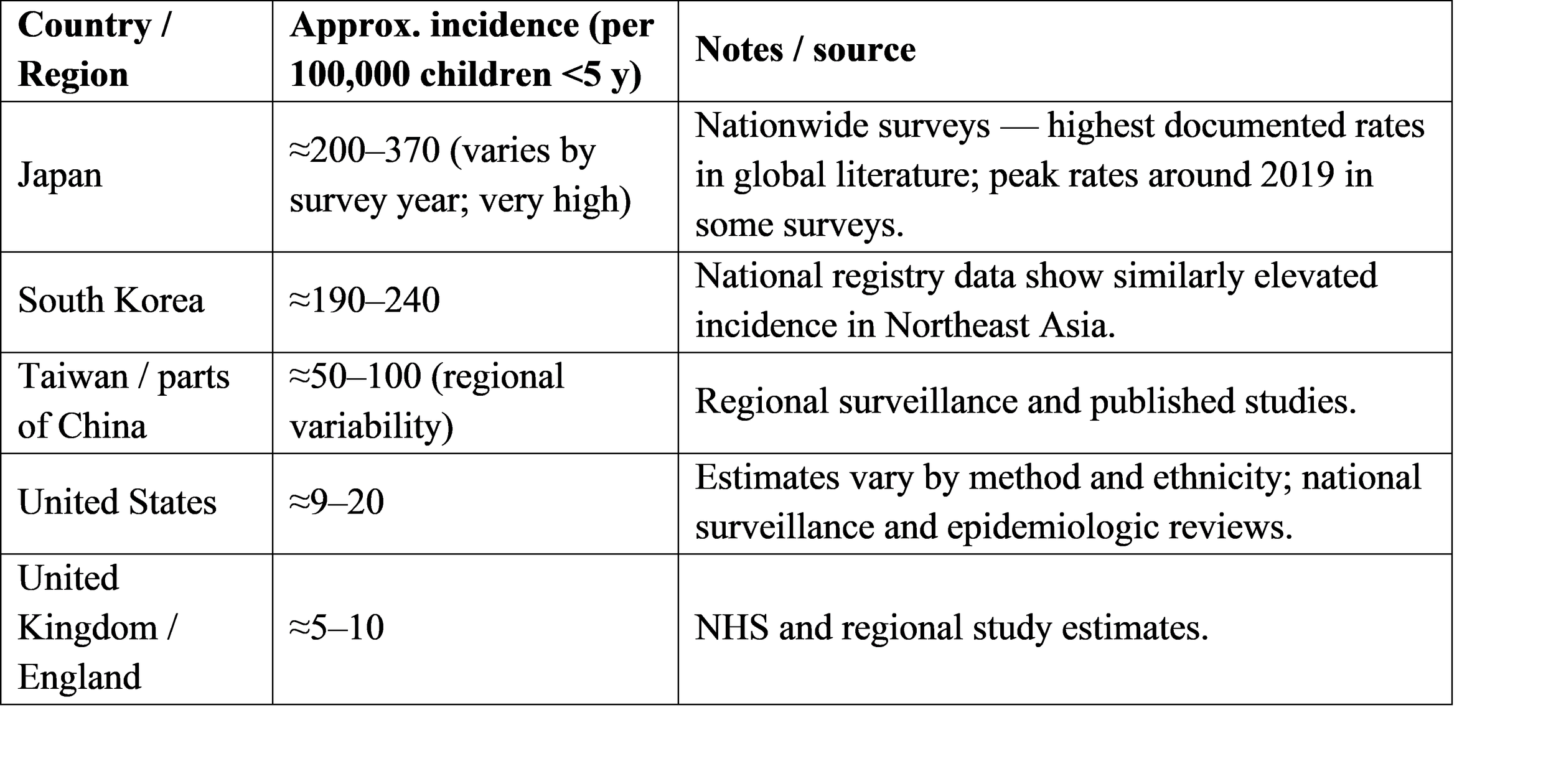
Note: Incidence estimates differ by surveillance methods, case definitions, and year. Japan’s nationwide surveys provide the most consistent high-quality incidence data and show the greatest rates globally.
Key Observations & Interpretations
Geographic clustering suggests genetic/environmental factors. The markedly elevated incidence in Japan and Korea — compared to much lower rates in much of Europe and North America — strongly suggests a combination of genetic susceptibility and localized environmental triggers. Continued genetic studies and standardized surveillance are needed to parse these contributors.
Early IVIG is protective for coronary outcomes. Randomized and observational evidence supports rapid IVIG administration to reduce coronary complications; thus, many guidelines advise a low threshold to treat when KD is strongly suspected.
Incomplete presentations are common in the youngest children and increase risk of delayed diagnosis. Because infants and very young children may not display full diagnostic criteria, algorithms that combine laboratory markers and echocardiography help reduce missed cases and prevent coronary sequelae.
MIS-C complicates the diagnostic landscape. Since 2020, MIS-C linked to SARS-CoV-2 exposure has presented with KD-like features in many cases. Distinguishing MIS-C from KD relies on epidemiologic clues (recent or prior COVID-19 exposure), older median age for MIS-C, more frequent myocardial dysfunction/shock in MIS-C, and distinctive biomarker patterns in some series; however, overlap exists and management can converge for severe inflammatory disease.
Treatment-resistant disease remains a challenge. A substantial minority of patients (approximately 10–20% in many series) are IVIG-resistant and require repeat IVIG or adjunctive corticosteroids/biologics. Improved risk stratification and prospective trials are necessary to optimize early use of adjunctive agents.
Research Points
Etiologic discovery: Large genomic, metagenomic, and environmental exposure studies are required to identify causal triggers or combinations of exposures that precipitate KD in susceptible children.
Diagnostic biomarkers: Development of sensitive and specific molecular biomarkers (proteomic, transcriptomic, or metabolomic signatures) could dramatically shorten diagnostic uncertainty and separate KD from mimics, including MIS-C.
Personalized therapy trials: Prospective randomized trials to determine which subgroups benefit from early corticosteroids or biologic therapy (versus standard IVIG alone) would help reduce unnecessary exposure while preventing coronary complications.
Longitudinal cardiovascular outcomes: Lifespan cohorts are needed to quantify long-term cardiovascular risk among KD survivors, including subclinical endothelial dysfunction or accelerated atherosclerosis risk.
Global surveillance standardization: A harmonized case definition and data reporting framework would improve the comparability of incidence, severity, and outcome data across regions.
Practical Recommendations for Clinicians
Maintain vigilance for KD in any child with unexplained fever ≥5 days and mucocutaneous features, particularly in children under five.
Use supportive laboratory markers and early echocardiography to guide diagnosis in incomplete cases.
Administer IVIG 2 g/kg promptly when KD is suspected or confirmed; start aspirin per local practice and tailor dose/duration to coronary findings. (AHA Journals)
In IVIG-resistant patients, escalate therapy (repeat IVIG ± corticosteroids ± biologics) and involve pediatric cardiology early.
Ensure appropriate cardiology follow-up and counseling for patients with coronary involvement; develop transition plans for adult care when indicated.
Conclusion
Kawasaki disease remains a clinically significant pediatric vasculitis with important acute and potentially lifelong cardiovascular implications. While early IVIG therapy has reduced the incidence of coronary aneurysms substantially, diagnostic uncertainty — especially in incomplete presentations and in the setting of MIS-C overlap — continues to challenge clinicians. Ongoing research into etiology, biomarkers, and optimized treatment algorithms is necessary to improve outcomes and reduce long-term cardiac burden. Robust, standardized surveillance will also permit better global comparisons and targeted public-health responses.
References
McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation. 2017;135(17):e927–e999. doi:10.1161/CIR.0000000000000484. (AHA Journals)
Centers for Disease Control and Prevention (CDC). Clinical Overview of Kawasaki Disease. CDC. 2024. Available at: https://www.cdc.gov/kawasaki/hcp/clinical-overview/index.html. (CDC)
Ae R, Makino N, Kosami K, et al. Incidence of Kawasaki Disease in Japan, 2017–2018: Results of the 25th Nationwide Survey. Pediatrics International. 2020;62(4):512–518. doi:10.1111/ped.14219. (Nationwide Japanese surveillance reporting high incidence; details on IVIG non-response rates). (PubMed)
James KE, et al. Kawasaki Disease: A Systematic Review and Meta-Analysis. Pediatric Allergy and Immunology. 2021;32(7):1234–1246. (Systematic synthesis of clinical features and outcomes). (PMC)
Feldstein LR, Rose EB, Horwitz SM, et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. New England Journal of Medicine. 2020;383:334–346. doi:10.1056/NEJMoa2021680. (Large series describing MIS-C and its overlaps with KD). (nejm.org)
Newburger JW, Takahashi M, Burns JC. Kawasaki Disease. Journal of the American College of Cardiology. 2016;67(14):1738–1749. doi:10.1016/j.jacc.2016.01.096. (Comprehensive review of clinical aspects and cardiac outcomes). (ScienceDirect)
Levin M. Childhood Multisystem Inflammatory Syndrome — A New Challenge in the COVID-19 Pandemic. Lancet. 2020;395:1741–1743. (Perspective on MIS-C vs KD). (PMC)
Hsu WF, et al. Epidemiological trends and healthcare burden of Kawasaki disease. Scientific Reports. 2025. (Recent epidemiology analysis reporting temporal trends; regional differences). (Nature)
Dallaire F, Dionne A, Johnson C, et al. Use of Echocardiography in Kawasaki Disease and MIS-C: Updated Recommendations. Journal of the American Society of Echocardiography. 2021;34(11):1165–1179. (Echo protocols and Z-score usage). (kdfoundation.org)
Texas Children’s Hospital. Diagnosis and Management of Kawasaki Disease in Children — Evidence-Based Guideline. 2024. (Institutional protocol reflecting contemporary practice). (Texas Children’s)