
Awareness, Utilization, and Ethical Perception of Artificial Intelligence Among Undergraduate Students A Cross-Sectional Survey Study
1. Ashish Dubey
2. Sabahat Karim
3. Muskan Alone
4. Kanymgul Asanbek kyzy
(1,2,3. Students, International Medical Faculty, Osh State University, Kyrgyz Republic)
(4. Professor, International Medical Faculty, Osh State University, Kyrgyz Republic)
Abstract
The integration of artificial intelligence into medical education has accelerated dramatically in recent years, yet the extent to which undergraduate students are aware of, utilize, and critically evaluate these technologies remains poorly understood. This cross-sectional survey study examined the awareness, utilization patterns, perceived educational benefits, and ethical concerns regarding artificial intelligence among 276 undergraduate students in the context of operative anatomy learning. The survey instrument comprised 19 items assessing demographic characteristics, awareness of AI applications, frequency and purpose of AI tool usage, types of tools employed, perceived educational impacts, trust in AI-generated information, encountered limitations, and attitudes toward regulation. The results revealed that while 76.1 percent of participants were aware of AI applications in operative anatomy, only 65.6 percent had actually used AI tools for learning, with the majority employing them at low to moderate frequencies. AI chat-based tools emerged as the most commonly used platform type, and learning anatomy was the predominant purpose. Participants generally held positive perceptions of AI's educational value, with substantial majorities agreeing that AI improves understanding, enhances visualization, aids surgical planning, reduces anatomical identification errors, improves operative skills through simulation, enhances knowledge retention, and increases procedural confidence. However, significant concerns were also evident: nearly half of participants had encountered incorrect or misleading AI-generated information, limited accessibility was identified as the primary barrier to AI adoption, and a substantial proportion expressed worry that over-reliance on AI may weaken fundamental anatomical knowledge. While a majority supported regulation of AI use in operative anatomy, a considerable segment remained neutral or opposed. These findings illuminate a complex landscape in which students recognize the transformative potential of AI while simultaneously harboring reservations about accuracy, accessibility, and the preservation of foundational learning. The study underscores the urgent need for structured AI literacy programs, validated educational platforms, and clear institutional guidelines to ensure that AI integration enhances rather than undermines the development of competent, critically thinking future clinicians.
Keywords:artificial intelligence, medical education, operative anatomy, undergraduate students, AI literacy, educational technology, medical ethics, survey study
1. Introduction
The landscape of medical education is undergoing a profound transformation, driven by the rapid proliferation of artificial intelligence technologies that promise to reshape how future clinicians learn, reason, and practice. From virtual anatomy platforms that render three-dimensional structures with unprecedented fidelity to AI chatbots capable of generating instant explanations of complex physiological processes, these tools offer opportunities that were inconceivable just a decade ago. Yet beneath the enthusiasm surrounding AI in medical education lies a terrain of uncertainty, where questions of awareness, appropriate utilization, educational efficacy, and ethical responsibility remain insufficiently explored. For undergraduate students standing at the threshold of their medical careers, the encounter with AI is not merely a technical matter of learning to use new software; it is a formative experience that shapes their epistemological habits, their clinical reasoning patterns, and their professional identity.
Operative anatomy occupies a particularly significant place in this evolving educational landscape. Unlike many other domains of medical knowledge, operative anatomy demands not merely intellectual comprehension but spatial reasoning, tactile intuition, and the ability to navigate three-dimensional structures under conditions of uncertainty and time pressure. The surgeon's knowledge of anatomy is not abstract but embodied, acquired through repeated exposure to the variability of human tissue, the unpredictability of pathological change, and the irreducible complexity of living systems. It is precisely this combination of cognitive and practical demands that makes operative anatomy both a promising domain for AI-assisted learning and a field where the limitations of artificial intelligence are most starkly revealed. A virtual platform can render the branches of the celiac trunk with photographic precision, but it cannot replicate the resistance of connective tissue, the pulsation of an artery, or the judgment required to proceed when anatomical variation defies textbook description.
The global discourse on AI in medical education has expanded considerably in recent years, with studies from diverse geographical and institutional contexts documenting student perceptions, faculty attitudes, and institutional responses. Research from Palestine has revealed that while medical students express optimism about AI's future role in medicine, the vast majority have received no formal education in AI during their medical training, with knowledge acquired primarily through social media, self-directed learning, and informal research experiences. Similar patterns have been documented in Canada, Germany, Pakistan, Syria, India, and Vietnam, suggesting a widespread gap between the rapid advancement of AI technology and the capacity of medical curricula to prepare students for its responsible use. This knowledge gap is not merely an academic concern; it has direct implications for patient safety, as clinicians who lack the critical skills to evaluate AI outputs may be vulnerable to errors propagated by algorithmic systems.
The phenomenon of AI-generated hallucinations, in which large language models produce plausible-sounding but factually incorrect information, has emerged as a particularly concerning challenge in medical education. A study evaluating general practice trainees' ability to detect ChatGPT-4o hallucinations found that the model's overall accuracy was 80.8 percent, but for professional practice scenarios, accuracy dropped to 57.0 percent, and after human verification, it fell further to 44.2 percent. The mean accuracy of trainees in detecting these hallucinations was only 55.0 percent, with regression analysis revealing that shorter response times, higher self-assessed AI understanding, and more frequent AI use were paradoxically associated with stricter error detection criteria. These findings suggest that familiarity with AI does not necessarily confer the critical discernment required to identify its errors, a sobering realization for educators seeking to integrate AI into medical training.
The question of over-reliance on AI has also attracted significant scholarly attention. A systematic review of AI's impact on clinical skill acquisition in medical students found that while AI exposure was associated with improved efficiency and basic knowledge acquisition, findings were less consistently supportive of higher-order reasoning outcomes. One randomized controlled trial reported significantly lower medical student performance when using ChatGPT-generated feedback compared to traditional expert feedback for complex clinical scenarios, suggesting that reliance on AI may result in deskilling. Another study found that ChatGPT enabled the fastest responses in clinical decision-making but produced less accurate and less complete decisions compared with guideline-based reasoning, with evidence of error propagation from poor prompts. In a cross-sectional survey of preclinical medical students, 83.2 percent expressed concern about over-reliance on technology, and 77.7 percent worried about potential loss of critical thinking skills, despite concurrently rating AI as effective for problem-solving and decision-making.
These concerns are particularly salient in operative anatomy, where the development of independent spatial reasoning and manual dexterity is foundational to surgical competence. Virtual simulation platforms have demonstrated significant potential in enhancing anatomical knowledge and procedural understanding, with one study showing that students using a virtual simulation teaching platform obtained significantly higher scores on gastrointestinal anatomy tests and laparoscopic appendectomy simulations compared to controls. However, the same study found no significant improvement in simulator-based laparoscopic suturing and knot-tying, suggesting that virtual simulation may be limited in developing the fine motor skills essential for operative procedures. This finding underscores the importance of maintaining a balanced approach in which AI-assisted learning complements rather than replaces hands-on training.
The ethical dimensions of AI integration in medical education extend beyond individual learning outcomes to encompass broader questions of equity, transparency, and professional responsibility. The American Medical Association has advocated for AI frameworks that prioritize transparency, equity, and accountability, while the Association of American Medical Colleges has outlined principles of ethical implementation, inclusive access, cross-disciplinary collaboration, and data security. From a deontological perspective, students are expected to produce authentic work, and using AI to create substantial portions of assignments raises fundamental questions about the integrity of the learning process. Consequentialist analysis suggests that while AI may save time, the potential harm to students' development of independent reasoning may outweigh short-term efficiency gains. Care ethics emphasizes the relational aspects of decision-making, indicating that actions involving AI must demonstrate care for all stakeholders, including patients who will ultimately be cared for by AI-influenced clinicians.
Against this backdrop of rapid technological change, emerging evidence of both promise and peril, and evolving ethical frameworks, the present study was designed to investigate how undergraduate students navigate the complex terrain of AI in operative anatomy. By examining awareness levels, utilization patterns, perceived educational impacts, encountered limitations, and attitudes toward regulation, the study aims to contribute empirical data that can inform curriculum development, institutional policy, and the broader discourse on responsible AI integration in medical education.
2. Materials and Methods
2.1 Study Design and Setting
This study employed a cross-sectional survey design to assess awareness, utilization, and ethical perceptions of artificial intelligence among undergraduate students in the context of operative anatomy education. The survey was conducted using a structured questionnaire distributed to participants through an online platform, with data collection managed via Google Forms. The study was designed and conducted by investigators Sabahat Karim, Muskan Alone, and Asish Dubey, under the guidance of Asanbek Kyzy. Ethical considerations were addressed through a consent form presented at the beginning of the survey, which informed participants that their data would not be shared with third parties and that the survey was conducted solely for research purposes.
2.2 Participants
A total of 276 undergraduate students participated in the survey. The sample size of 276 responses provides adequate statistical power for descriptive and comparative analyses of the survey items. Participants were recruited through convenience sampling, with the survey link distributed through academic channels, social media platforms, and peer networks. The demographic characteristics of the sample, including year of study, institutional affiliation, and prior exposure to AI, were not explicitly collected in the survey instrument, representing a limitation that is addressed in the discussion.
2.3 Survey Instrument
The questionnaire comprised 19 items designed to capture multiple dimensions of the student-AI interface in operative anatomy. The items were organized into thematic domains: awareness and prior knowledge, utilization behavior, perceived educational impact, trust and skepticism, encountered limitations, and attitudes toward regulation. The instrument utilized a combination of binary response options, Likert scales, and multiple-choice formats to accommodate the diverse nature of the constructs being measured.
The specific survey items and their response formats were as follows: awareness of AI in operative anatomy (binary: Yes/No); prior use of AI tools for learning operative anatomy (binary: Yes/No); frequency of AI-based tool usage (five-point ordinal: Never, Rarely, Sometimes, Often, Very Often); primary purpose of AI use (multiple-choice: Learning Anatomy, Surgical Planning, Simulation Training, Research, I do not use AI); type of AI tools primarily used (multiple-choice: Virtual anatomy platforms, Surgical simulators, AI chat-based tools, Imaging/diagnostic AI, None); perceived impact of AI on understanding operative anatomy (five-point Likert: Strongly Disagree to Strongly Agree); perceived impact on visualization of complex structures (five-point Likert); perceived impact on surgical planning ability (five-point Likert); perceived impact on reducing anatomical identification errors (five-point Likert); perceived impact of AI-assisted simulations on operative skills (five-point Likert); perceived impact on anatomical knowledge retention (five-point Likert); perceived impact on procedural confidence (five-point Likert); comparison of AI with traditional learning methods (five-point Likert); trust in AI-generated anatomical information (five-point Likert); experience with incorrect or misleading AI information (three-point: Yes, No, Not Sure); perceived main limitation of AI in operative anatomy (multiple-choice: Lack of accuracy, High cost, Limited accessibility, Lack of realism, Insufficient training); perceived accessibility of AI tools (five-point Likert); concern about over-reliance weakening fundamental knowledge (five-point Likert); and attitude toward regulation of AI use in operative anatomy (five-point Likert).
2.4 Data Collection and Analysis
Data were collected through the Google Forms platform, which automatically recorded responses and generated descriptive statistics including frequencies and percentages for each survey item. The data were extracted from the platform and organized for presentation in the results section. Given the descriptive nature of the study, inferential statistical analyses were not performed; instead, the analysis focused on characterizing the distribution of responses across items and identifying patterns and trends in the data. The presentation of results follows the sequential order of the survey items, with percentages reported to one decimal place as generated by the survey platform.
2.5 Ethical Considerations
The study was conducted in accordance with principles of research ethics, including voluntary participation, informed consent, confidentiality, and data protection. The consent form explicitly stated that participant data would not be shared with third parties and that the survey was intended solely for research purposes. No personally identifiable information was collected, and responses were analyzed in aggregate form.
3. Results
3.1 Awareness of Artificial Intelligence in Operative Anatomy
The first dimension explored in the survey was participants' awareness of AI applications in operative anatomy. Of the 276 respondents, 210 students (76.1 percent) indicated that they were aware of the use of AI in operative anatomy, while 66 students (23.9 percent) reported no awareness. This finding suggests that while a substantial majority of undergraduate students have at least a basic awareness of AI's relevance to operative anatomy, nearly one-quarter remain unaware, indicating a significant knowledge gap that may have implications for equitable access to AI-enhanced learning opportunities. The relatively high awareness rate of 76.1 percent may reflect the increasing visibility of AI in popular media, academic discourse, and institutional communications, yet the persistence of nearly one in four students without awareness underscores the need for more systematic efforts to inform students about emerging educational technologies.
3.2 Utilization of AI Tools for Learning Operative Anatomy
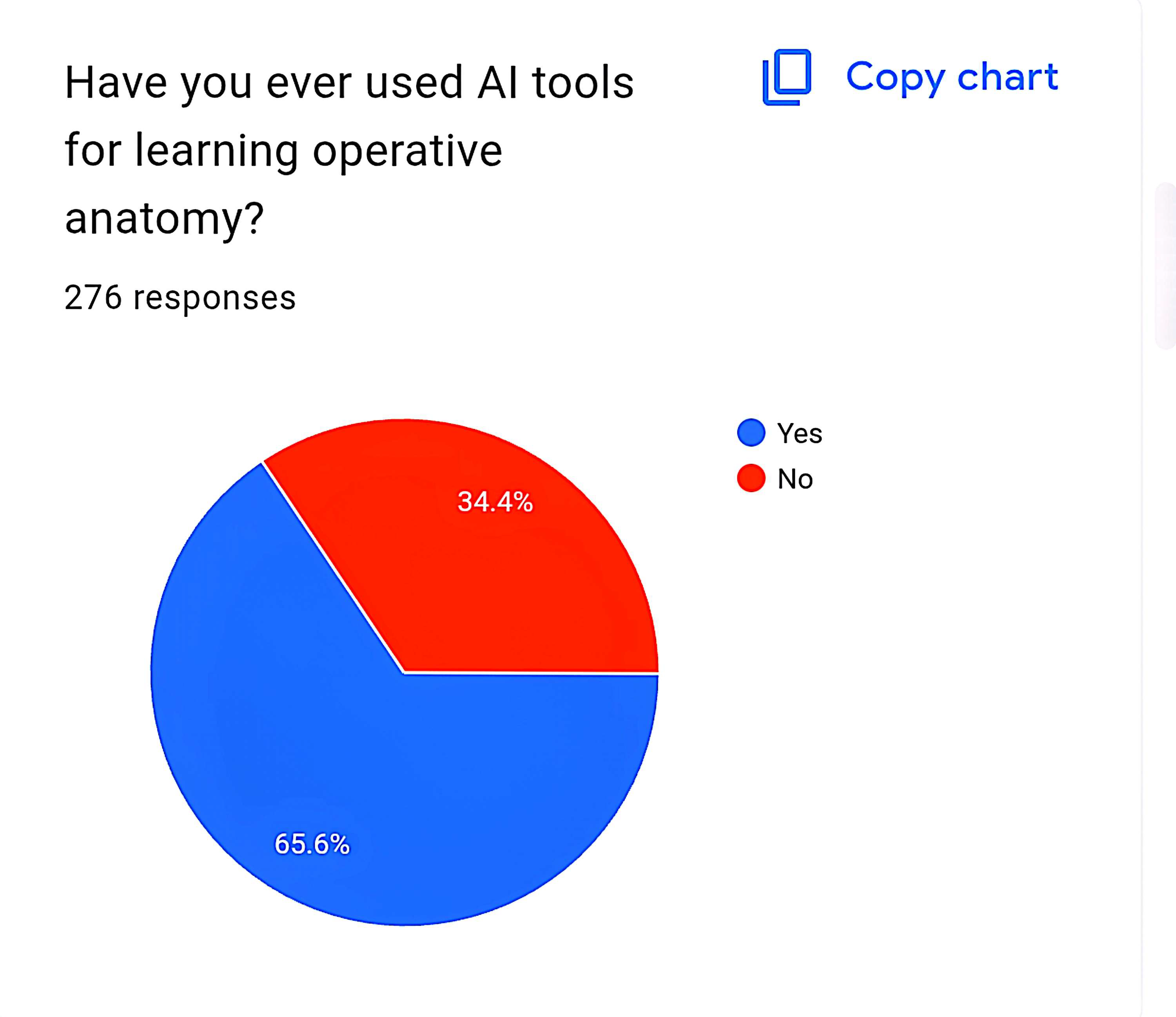
Despite the majority awareness of AI in operative anatomy, actual utilization was considerably lower. When asked whether they had ever used AI tools for learning operative anatomy, 181 students (65.6 percent) responded affirmatively, while 95 students (34.4 percent) had never used such tools. This 10.5 percentage point gap between awareness and utilization suggests that awareness does not automatically translate into adoption, with approximately one-third of aware students not yet having engaged with AI tools for operative anatomy learning. The reasons for this awareness-utilization gap may include lack of access to appropriate tools, uncertainty about how to integrate AI into study routines, preference for traditional learning methods, or concerns about the reliability of AI-generated information.
The frequency of AI-based tool usage among the 276 respondents revealed a distribution skewed toward occasional rather than regular use. The largest group, comprising 117 students (42.4 percent), reported using AI tools "Sometimes." The next largest group, 58 students (21.0 percent), used AI "Rarely." Equal proportions of 25 students each (9.1 percent) reported using AI "Never" and "Very Often," while 51 students (18.5 percent) used AI "Often." These data indicate that while a majority of students (81.5 percent) have at least occasional exposure to AI tools, only 27.6 percent use them with high frequency (Often or Very Often). The predominance of occasional and rare usage suggests that AI has not yet become a fully integrated component of most students' study routines, but rather serves as a supplementary resource accessed on an ad hoc basis.
3.3 Purpose and Type of AI Tool Usage
When asked about the primary purpose for which they used AI, the 276 respondents demonstrated a clear hierarchy of applications. Learning anatomy was the dominant purpose, selected by 173 students (62.7 percent), reflecting the foundational importance of anatomical knowledge in operative training. Research was the second most common purpose, chosen by 47 students (17.0 percent), indicating that a subset of students leverages AI for literature review, data analysis, and academic inquiry. Simulation training was selected by 23 students (8.3 percent), while surgical planning was chosen by 14 students (5.1 percent). Notably, 20 students (7.2 percent) indicated that they did not use AI at all, a figure that aligns closely with the 9.1 percent who reported "Never" using AI in the frequency question, with minor discrepancy likely attributable to differences in question framing and respondent interpretation.
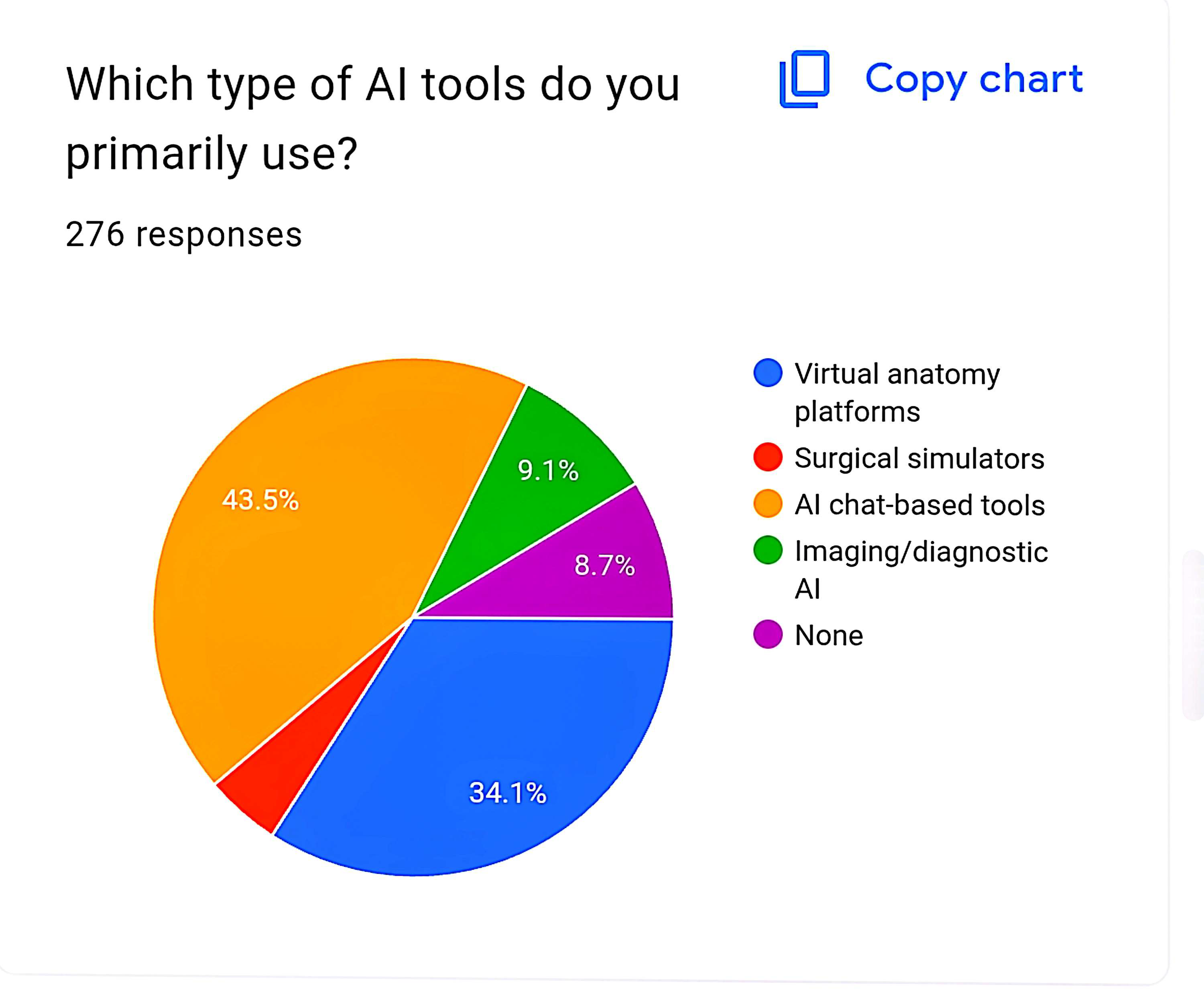
The types of AI tools primarily used by participants revealed an interesting pattern that reflects the current accessibility and familiarity of different platforms. AI chat-based tools emerged as the most commonly used category, selected by 120 students (43.5 percent), suggesting that general-purpose conversational AI platforms such as ChatGPT have penetrated student learning practices more deeply than specialized medical applications. Virtual anatomy platforms were the second most popular, chosen by 94 students (34.1 percent), indicating substantial engagement with dedicated anatomical visualization software. Imaging and diagnostic AI was used by 24 students (8.7 percent), while surgical simulators were employed by only 10 students (3.6 percent). A significant proportion of 28 students (10.1 percent) reported using none of the listed tool types, which may include students who use AI in other forms not captured by the options or who do not use AI at all.
3.4 Perceived Educational Impact of AI on Operative Anatomy Learning
The survey included eight items assessing participants' perceptions of AI's impact on various dimensions of operative anatomy learning, each measured on a five-point Likert scale from Strongly Disagree to Strongly Agree.
Regarding the statement that "AI improves my understanding of operative anatomy," the 276 respondents expressed predominantly positive views. A total of 114 students (41.3 percent) selected "Agree," while 20 students (7.2 percent) selected "Strongly Agree," yielding a combined positive response rate of 48.5 percent. The largest single group, 103 students (37.3 percent), selected "Neutral," indicating a substantial segment of students who neither endorse nor reject the educational value of AI for understanding operative anatomy. Negative responses were relatively limited, with 24 students (8.7 percent) selecting "Strongly Disagree" and 15 students (5.4 percent) selecting "Disagree," for a combined negative rate of 14.1 percent. The high proportion of neutral responses suggests that many students may not yet have formed definitive opinions about AI's educational impact, possibly due to limited experience or uncertainty about how to evaluate its effectiveness.
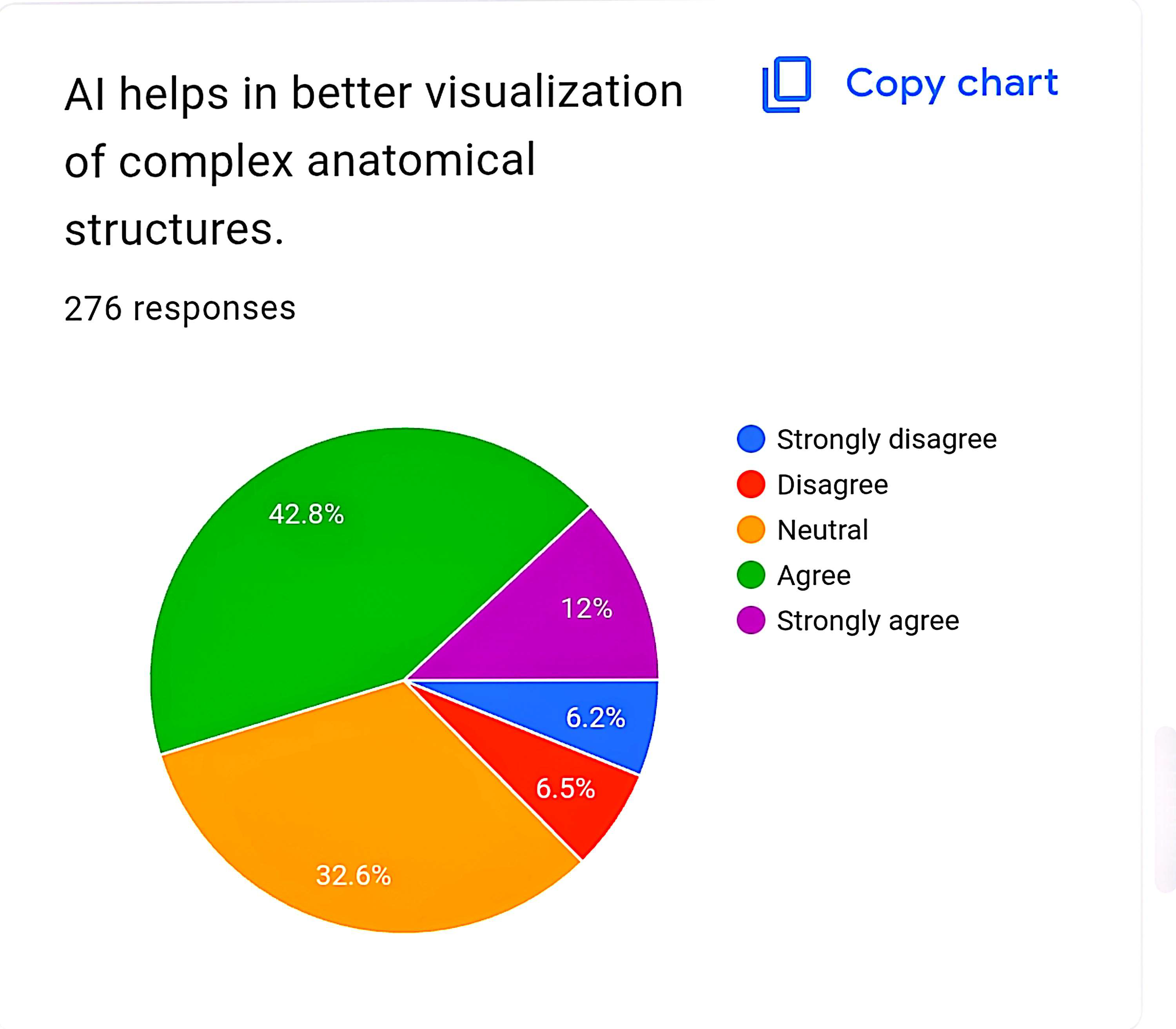
The perception that "AI helps in better visualization of complex anatomical structures" elicited an even more favorable response pattern. A total of 118 students (42.8 percent) agreed with this statement, and 33 students (12.0 percent) strongly agreed, yielding a combined positive rate of 54.8 percent. This represents the highest level of consensus among the eight perception items, suggesting that the visualization affordances of AI are its most widely recognized and appreciated educational benefit. The neutral category comprised 90 students (32.6 percent), while negative responses were minimal: 18 students (6.5 percent) disagreed and 17 students (6.2 percent) strongly disagreed, for a combined negative rate of 12.7 percent. The strong positive response to this item aligns with the known capabilities of virtual anatomy platforms and three-dimensional rendering technologies to represent spatial relationships in ways that traditional two-dimensional textbooks cannot.
The statement that "AI enhances my ability to plan surgical procedures" generated more mixed responses. While 98 students (35.5 percent) agreed and 14 students (5.1 percent) strongly agreed, for a combined positive rate of 40.6 percent, the largest single group of 125 students (45.3 percent) selected "Neutral." This high neutral rate suggests that many students have not yet experienced or do not yet recognize AI's potential contributions to surgical planning, a more advanced application that may be less accessible to undergraduates than basic anatomical learning. Negative responses totaled 39 students (14.1 percent), with 17 students (6.2 percent) strongly disagreeing and 22 students (8.0 percent) disagreeing. The lower positive response rate for surgical planning compared to visualization reflects the reality that AI-assisted surgical planning tools are less commonly available to students and require a higher level of clinical reasoning to appreciate.
Regarding the statement that "AI reduces errors in identifying anatomical structures," 93 students (33.7 percent) agreed and 17 students (6.2 percent) strongly agreed, for a combined positive rate of 39.9 percent. The neutral category was again the largest, comprising 135 students (48.9 percent), while 36 students (13.0 percent) expressed negative views (18 students or 6.5 percent disagreeing, and 18 students or 6.5 percent strongly disagreeing). The substantial neutral response may reflect uncertainty about whether AI actually reduces errors or merely provides alternative sources of information that may themselves contain errors, a concern substantiated by the later survey item on encountered misinformation.
The perception that "AI-assisted simulations improve my operative skills" showed a similar distribution. A total of 111 students (40.2 percent) agreed and 15 students (5.4 percent) strongly agreed, yielding a combined positive rate of 45.6 percent. The neutral category included 119 students (43.1 percent), while negative responses were limited to 30 students (10.9 percent), equally split between 15 students (5.4 percent) strongly disagreeing and 15 students (5.4 percent) disagreeing. The positive response rate for this item, while substantial, is tempered by the large neutral segment, suggesting that many students have not yet had sufficient experience with AI-assisted simulations to form definitive opinions about their impact on operative skills.
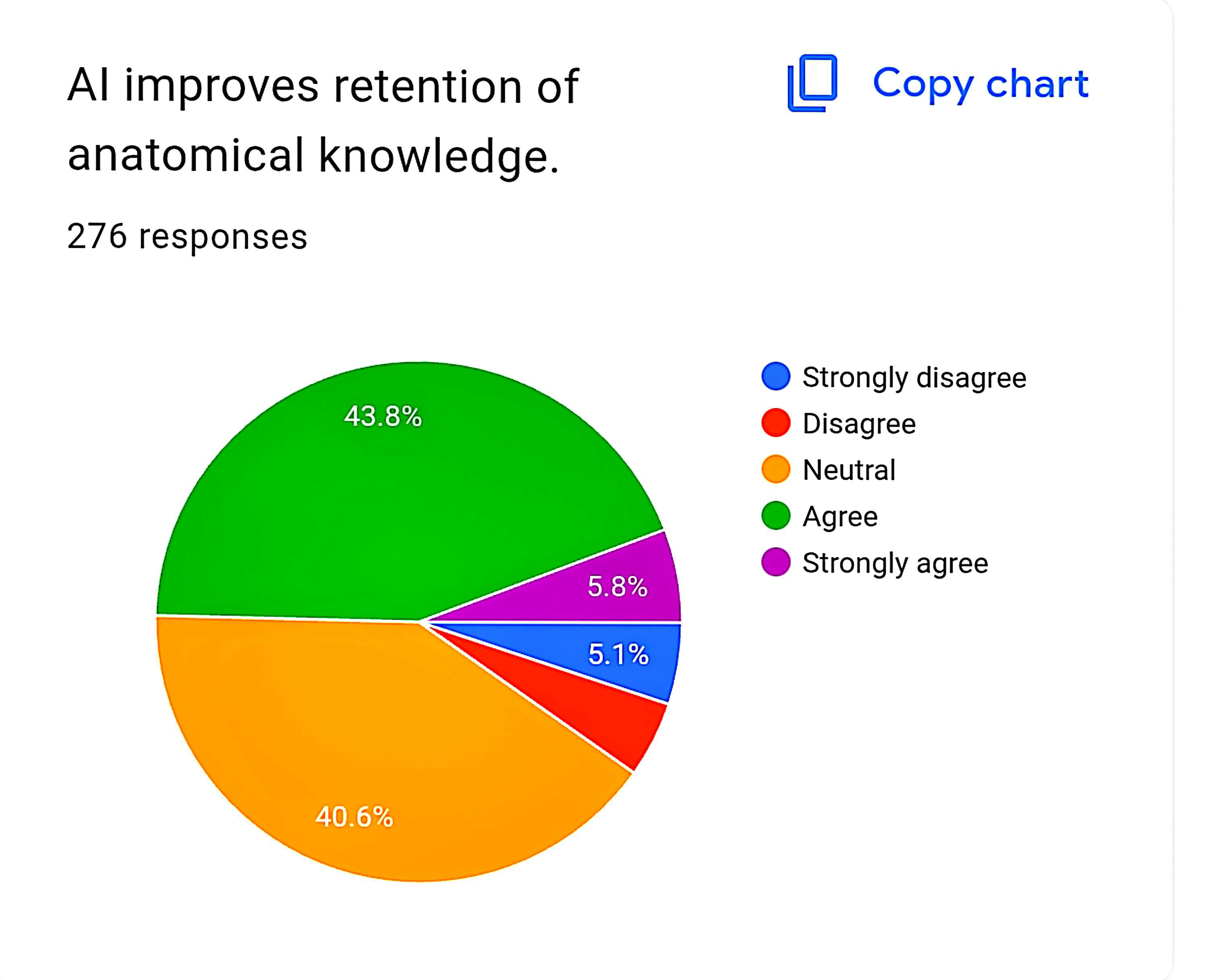
The statement that "AI improves retention of anatomical knowledge" elicited positive responses from 121 students (43.8 percent agreeing) and 16 students (5.8 percent strongly agreeing), for a combined positive rate of 49.6 percent. The neutral category comprised 112 students (40.6 percent), while negative responses totaled 27 students (9.8 percent), with 14 students (5.1 percent) strongly disagreeing and 19 students (6.9 percent) disagreeing. The relatively high positive response rate for knowledge retention, approaching 50 percent, suggests that students who have engaged with AI tools perceive meaningful benefits for long-term memory consolidation, possibly through the interactive and repetitive nature of AI-assisted learning.
The perception that "AI increases my confidence before performing procedures" showed a distribution similar to other items, with 111 students (40.2 percent) agreeing and 19 students (6.9 percent) strongly agreeing, for a combined positive rate of 47.1 percent. The neutral category included 115 students (41.7 percent), while negative responses totaled 31 students (11.2 percent), with 17 students (6.2 percent) strongly disagreeing and 14 students (5.1 percent) disagreeing. The positive response to this item suggests that AI tools may serve a psychological as well as cognitive function, bolstering student confidence through preparatory visualization and rehearsal.
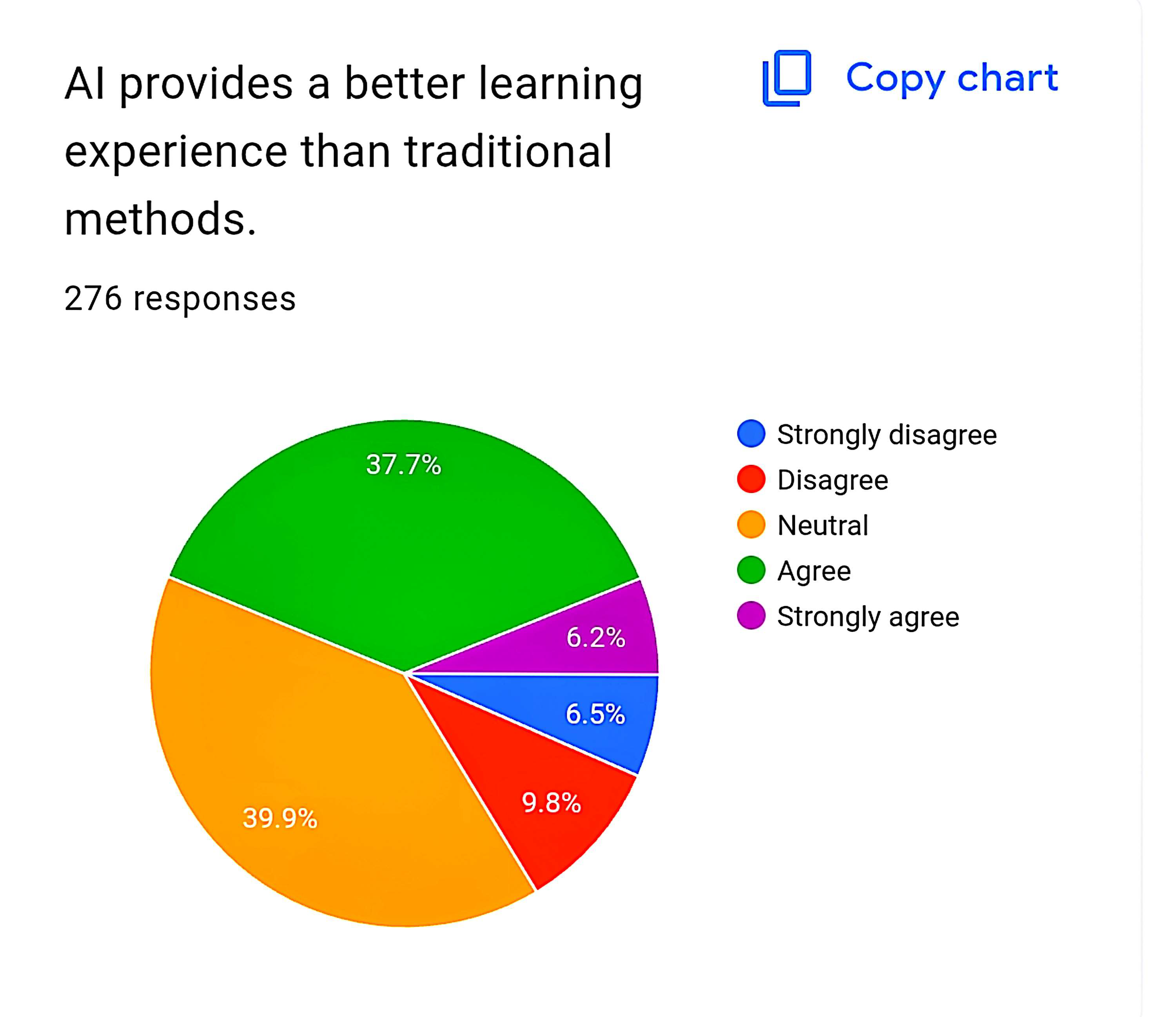
The final perception item, stating that "AI provides a better learning experience than traditional methods," generated a combined positive response from 104 students (37.7 percent agreeing) and 17 students (6.2 percent strongly agreeing), for a total of 43.9 percent. The neutral category was the largest single group at 110 students (39.9 percent), while negative responses were more pronounced than for other items, with 27 students (9.8 percent) disagreeing and 18 students (6.5 percent) strongly disagreeing, for a combined negative rate of 16.3 percent. The lower positive and higher negative response rates for this comparative item suggest that while students appreciate specific affordances of AI, they are not yet prepared to declare it superior to traditional methods overall, reflecting a nuanced and balanced perspective that resists technological determinism.
3.5 Trust in AI-Generated Information
Trust in AI-generated anatomical information was assessed through the statement "I trust AI-generated anatomical information." The responses revealed a cautious and divided attitude among participants. A total of 96 students (34.8 percent) agreed with the statement, and a smaller group of 13 students (4.7 percent) strongly agreed, yielding a combined trust rate of 39.5 percent. However, the largest single category was "Neutral," selected by 131 students (47.5 percent), indicating that nearly half of respondents have not yet committed to trusting or distrusting AI-generated anatomical content. Negative responses totaled 36 students (13.0 percent), with 21 students (7.6 percent) strongly disagreeing and 21 students (7.6 percent) disagreeing. The predominance of neutral responses, combined with the substantial minority expressing explicit distrust, suggests that students are approaching AI-generated information with appropriate skepticism, recognizing the potential for error while remaining open to its utility.
3.6 Experience with Incorrect or Misleading Information
When asked whether they had ever encountered incorrect or misleading information from AI, the 276 respondents provided a revealing distribution that validates the cautious trust patterns observed in the previous item. A total of 135 students (48.9 percent) answered "Yes," indicating that nearly half of participants have personally experienced AI-generated misinformation in the context of their anatomical studies. Only 51 students (18.5 percent) answered "No," while a substantial group of 90 students (32.6 percent) selected "Not Sure," suggesting uncertainty about whether information they received was accurate. The high rate of confirmed misinformation encounters, combined with the large "Not Sure" category, underscores the critical importance of developing students' capacity to critically evaluate AI outputs. The fact that only 18.5 percent of students are confident that they have not encountered misinformation may itself reflect either fortunate experience or, more concerningly, unrecognized exposure to subtle errors.
3.7 Perceived Limitations of AI in Operative Anatomy
Participants were asked to identify the main limitation of AI in operative anatomy from a list of five options. The responses revealed limited accessibility as the dominant concern, selected by 113 students (40.9 percent). This finding suggests that for the largest group of students, the primary barrier to AI adoption is not skepticism about its value but practical constraints on access, which may include cost, institutional availability, internet connectivity, or device requirements. Lack of accuracy was the second most commonly identified limitation, chosen by 58 students (21.0 percent), reflecting concerns validated by the nearly 49 percent of students who reported encountering misinformation. High cost was selected by 53 students (19.2 percent), indicating that financial barriers represent a significant obstacle for a substantial minority. Lack of realism was identified by 31 students (11.2 percent), while insufficient training was chosen by 21 students (7.6 percent). The relatively low selection of "insufficient training" as a primary limitation is noteworthy, suggesting that students may not yet recognize the importance of structured guidance in using AI tools effectively, or that they perceive access and accuracy as more pressing concerns.
3.8 Perceived Accessibility of AI Tools
The statement "AI tools are easily accessible to me" generated a distribution that corroborates the identification of limited accessibility as the primary limitation. Only 91 students (33.0 percent) agreed with the statement, and a mere 7 students (2.5 percent) strongly agreed, for a combined positive rate of 35.5 percent. The neutral category was the largest single group at 141 students (51.1 percent), while negative responses totaled 37 students (13.4 percent), with 17 students (6.2 percent) strongly disagreeing and 20 students (7.2 percent) disagreeing. The fact that only about one-third of students perceive AI tools as easily accessible, despite the widespread availability of free chat-based platforms, suggests that accessibility encompasses more than mere availability. It may include awareness of appropriate tools, knowledge of how to use them effectively, institutional support, and the quality and relevance of available resources for operative anatomy specifically.
3.9 Concerns About Over-Reliance on AI
The statement "Over-reliance on AI may weaken fundamental anatomical knowledge" elicited a distribution that reveals substantial concern among participants about the potential for AI to undermine foundational learning. A total of 95 students (34.4 percent) agreed with this statement, and 26 students (9.4 percent) strongly agreed, yielding a combined concern rate of 43.8 percent. The neutral category comprised 116 students (42.0 percent), while negative responses totaled 39 students (14.1 percent), with 20 students (7.2 percent) strongly disagreeing and 19 students (6.9 percent) disagreeing. The fact that nearly 44 percent of students express explicit concern about over-reliance, with only 14 percent dismissing this worry, suggests that the student body is keenly aware of the deskilling risks documented in the medical education literature. This concern coexists with the generally positive perceptions of AI's educational benefits, creating a tension that students must navigate in their own learning practices.
3.10 Attitudes Toward Regulation of AI in Operative Anatomy
The final survey item assessed attitudes toward regulation through the statement "AI use in operative anatomy should be regulated." The responses revealed a majority in favor of regulation, though with significant neutral and opposing voices. A total of 87 students (31.5 percent) agreed with the statement, and 16 students (5.8 percent) strongly agreed, for a combined supportive rate of 37.3 percent. The neutral category was the largest single group at 140 students (50.7 percent), while negative responses totaled 33 students (12.0 percent), with 16 students (5.8 percent) strongly disagreeing and 20 students (7.2 percent) disagreeing. The substantial neutral response suggests that many students have not yet formed definitive opinions about the appropriate regulatory framework for AI in medical education, possibly due to limited exposure to policy discussions or uncertainty about what effective regulation would entail. The fact that only 12 percent oppose regulation, compared to 37 percent who support it, indicates that among students who have formed opinions, the balance tilts toward favoring structured oversight.
4. Discussion
The findings of this survey paint a nuanced portrait of undergraduate students' engagement with artificial intelligence in operative anatomy, revealing a population that is simultaneously curious and cautious, enthusiastic and skeptical, eager to embrace new technologies yet mindful of their limitations. This complexity defies simplistic narratives of technological adoption and instead points to the need for thoughtful, evidence-based approaches to integrating AI into medical curricula.
The awareness-utilization gap identified in this study, wherein 76.1 percent of students are aware of AI in operative anatomy but only 65.6 percent have actually used AI tools, with an even smaller proportion using them regularly, mirrors patterns documented in international literature. A study of Palestinian medical students found that 71.63 percent knew that AI, neural networks, machine learning, and deep learning techniques are used in medicine, yet 76.79 percent had received no formal education about AI during their medical training, with knowledge acquired primarily through social media, medical training experiences, and self-directed research. Similarly, a European survey found that only one-third of medical students reported knowing the basics of AI, while studies from Germany, Pakistan, Syria, India, and Vietnam have consistently documented insufficient AI knowledge among medical students. The present study's finding that 23.9 percent of students are entirely unaware of AI in operative anatomy, despite the technology's increasing prominence, suggests that awareness campaigns and curricular integration remain incomplete.
The dominance of AI chat-based tools as the most commonly used platform type, selected by 43.5 percent of respondents, is consistent with the global penetration of large language models such as ChatGPT into educational contexts. Research comparing AI platforms for medical education has found that ChatGPT-4 achieved statistically superior accuracy in answering anatomy questions compared to competing platforms, with one study reporting 60.5 percent accuracy and another documenting 100 percent accuracy in specific anatomy question sets. However, the same studies noted significant variability in performance across platforms, with Gemini lagging at 60 percent accuracy. The reliance on general-purpose chat-based tools rather than specialized anatomical platforms may reflect their greater accessibility and familiarity, but it also raises concerns about the appropriateness of using generalist AI for specialized medical learning, particularly given the documented phenomenon of AI hallucinations in clinical contexts.
The finding that 48.9 percent of students have encountered incorrect or misleading information from AI, with an additional 32.6 percent unsure whether they have, aligns with and extends the growing body of evidence on AI reliability in medical education. A study evaluating general practice trainees' ability to detect ChatGPT-4o hallucinations found that the model's accuracy for professional practice scenarios was only 57.0 percent, dropping to 44.2 percent after human verification, with trainees detecting only 55.0 percent of hallucinations on average. The present study's finding that nearly half of undergraduate students have personally encountered AI misinformation, combined with the large proportion who are uncertain about the accuracy of information they have received, suggests that the problem of AI-generated errors is not merely theoretical but a lived reality for students. This has profound implications for patient safety, as students who internalize incorrect anatomical information may carry these errors into their clinical practice.
The perception data reveal a fascinating tension between recognition of AI's educational benefits and awareness of its risks. On one hand, substantial proportions of students acknowledge that AI improves understanding, enhances visualization, aids surgical planning, reduces errors, improves operative skills through simulation, enhances retention, and increases confidence. The visualization affordance received the strongest endorsement, with 54.8 percent of students agreeing or strongly agreeing that AI helps in better visualization of complex structures, a finding that resonates with the established capabilities of three-dimensional rendering and virtual reality platforms to represent spatial relationships. On the other hand, 43.8 percent of students expressed concern that over-reliance on AI may weaken fundamental anatomical knowledge, and only 39.5 percent expressed trust in AI-generated anatomical information. This coexistence of appreciation and apprehension suggests that students are developing a sophisticated, critically informed perspective on AI that resists both uncritical enthusiasm and blanket rejection.
The identification of limited accessibility as the primary limitation of AI in operative anatomy, selected by 40.9 percent of respondents, is a critical finding that demands institutional attention. While 43.5 percent of students use AI chat-based tools, which are generally freely available, the perception of limited accessibility may reflect barriers beyond mere availability. These may include lack of awareness of appropriate specialized tools, insufficient institutional subscriptions to premium anatomical platforms, inadequate device infrastructure, poor internet connectivity, or the absence of guidance on how to effectively integrate AI into study routines. The fact that only 35.5 percent of students perceive AI tools as easily accessible, despite the ubiquity of free chat-based platforms, suggests that accessibility is a multidimensional construct encompassing awareness, usability, relevance, and support, not simply availability.
The concern about over-reliance weakening fundamental knowledge, expressed by 43.8 percent of students, is substantiated by emerging evidence from the medical education literature. A systematic review of AI's impact on clinical skill acquisition found that while AI exposure improved efficiency and basic knowledge, findings were less supportive of higher-order reasoning outcomes. A randomized controlled trial reported significantly lower medical student performance when using ChatGPT-generated feedback compared to expert feedback for complex clinical scenarios, suggesting potential deskilling. Another study found that ChatGPT produced less accurate and less complete clinical decisions compared with guideline-based reasoning, with evidence of error propagation. In a survey of preclinical medical students, 83.2 percent expressed concern about over-reliance and 77.7 percent worried about loss of critical thinking skills. The present study's finding that 43.8 percent of students share this concern, with an additional 42 percent neutral, indicates that the deskilling worry has permeated student consciousness and should inform curricular design.
The attitude toward regulation, with 37.3 percent supporting regulation, 50.7 percent neutral, and only 12 percent opposed, suggests that students are open to structured oversight of AI in medical education, even if many have not yet formed definitive opinions. This finding aligns with broader ethical discourse on AI in medicine, which has emphasized the need for frameworks prioritizing transparency, equity, and accountability. The American Medical Association has advocated for AI frameworks that ensure trust through transparency and accountability, while the Association of American Medical Colleges has outlined principles of ethical implementation, inclusive access, cross-disciplinary collaboration, and data security. From a deontological perspective, students are expected to produce authentic work, and regulation can help ensure that AI use supports rather than supplants genuine learning. Consequentialist analysis suggests that while AI may offer short-term efficiency gains, regulation is necessary to prevent long-term harm to clinical reasoning development.
Several limitations of this study should be acknowledged. The cross-sectional design precludes causal inference and cannot capture changes in awareness, utilization, or perception over time. The absence of demographic data collection, including year of study, institutional affiliation, prior AI training, and socioeconomic background, limits the ability to identify subgroups that may differ in their AI engagement patterns. The survey instrument, while comprehensive, relied on self-reported perceptions rather than objective measures of AI usage or educational outcomes. The convenience sampling method may have introduced selection bias, with students who are more engaged with technology potentially overrepresented. Additionally, the survey did not distinguish between different types of operative anatomy learners, such as medical students, surgical residents, and allied health students, who may have different needs and experiences with AI.
Despite these limitations, the study contributes valuable empirical data to the growing discourse on AI in medical education. The findings suggest several directions for future research and practice. Longitudinal studies tracking students' AI engagement and clinical reasoning development over the course of their training would help clarify the long-term impacts of AI integration. Comparative studies examining the educational outcomes of AI-assisted versus traditional learning in operative anatomy would provide objective evidence to complement the perceptual data reported here. Qualitative research exploring students' lived experiences with AI, including specific instances of misinformation encounters and strategies for error detection, would enrich understanding of the challenges documented in this survey.
From a practical standpoint, the findings support several recommendations for medical educators and institutions. First, structured AI literacy programs should be integrated into medical curricula, providing students with the knowledge and skills to critically evaluate AI outputs, recognize limitations, and use these tools responsibly. Second, institutions should invest in accessible, validated AI platforms specifically designed for anatomical education, reducing reliance on general-purpose tools that may generate inaccurate information. Third, clear guidelines and policies on appropriate AI use should be developed in collaboration with students, ensuring that regulation is perceived as supportive rather than restrictive. Fourth, faculty development programs should prepare educators to guide students in effective AI integration, addressing the "insufficient training" limitation identified by 7.6 percent of respondents but likely affecting a much larger proportion. Fifth, assessment methods should be adapted to evaluate students' independent reasoning abilities, ensuring that AI-assisted learning does not mask deficits in foundational knowledge and clinical judgment.
5. Conclusion
The integration of artificial intelligence into operative anatomy education represents both an extraordinary opportunity and a profound challenge for undergraduate medical training. This survey of 276 students reveals a population that is largely aware of AI's potential, moderately engaged with its tools, generally appreciative of its educational benefits, yet appropriately cautious about its limitations and risks. The findings illuminate a critical juncture in medical education, where the rapid proliferation of AI technologies has outpaced the development of curricula, policies, and pedagogical frameworks necessary for their responsible integration.
The data tell a story of students navigating uncertainty with remarkable thoughtfulness. They recognize that AI can render the invisible visible, transforming abstract anatomical descriptions into immersive three-dimensional experiences. They appreciate the convenience of instant explanations and the confidence that comes from preparatory rehearsal. Yet they also know, from direct experience, that AI can mislead, that accessibility remains uneven, and that the seductive efficiency of algorithmic assistance may come at the cost of the deep, hard-won knowledge that defines surgical mastery. Nearly half have encountered AI-generated errors, and nearly as many worry that over-reliance may erode the very foundations of their anatomical understanding.
This is not a story of technophobic resistance or uncritical adoption, but of emerging professionals grappling with the central question of their education: how to become competent, compassionate, and critically thinking clinicians in an age of intelligent machines. The students who participated in this survey are not passive recipients of technological change but active agents shaping its meaning and direction through their choices, their concerns, and their calls for regulation.
The path forward requires a partnership between students, educators, institutions, and technology developers. Medical curricula must evolve to include AI literacy as a core competency, not an optional add-on. Accessible, validated, and ethically designed AI tools must be made available to all students, regardless of institutional resources or personal means. Assessment practices must be reimagined to evaluate the independent reasoning skills that AI cannot replace. And regulatory frameworks must be developed through inclusive dialogue, ensuring that oversight serves the interests of learners and patients rather than merely managing institutional risk.
Ultimately, the goal is not to determine whether AI belongs in operative anatomy education, for its presence is already established and its potential undeniable. The goal is to ensure that its integration serves the highest purposes of medical education: the cultivation of clinicians who possess not only technical proficiency but also the wisdom to know when to trust and when to question, the humility to recognize the limits of any tool, and the commitment to place patient welfare above convenience or novelty. The students whose voices are captured in this survey are asking for nothing less, and it is the responsibility of the medical education community to respond with the seriousness and urgency that their questions demand.
References
Karim S, Alone M, Dubey A, Kyzy A. Survey on the Use of AI in Operative Anatomy. Unpublished survey data, 276 responses. 2026.
Abu-Rmilah AA, Hamdan M, Khammash H, et al. Perceptions of undergraduate medical students on artificial intelligence in medicine: mixed-methods survey study from Palestine. BMC Medical Education. 2024;24:Article ID 5465.
Teng S, et al. Perspectives of healthcare students on artificial intelligence in Canada. Journal of Medical Education. 2020.
Pinto dos Santos D, Giese D, Brodehl S, et al. Medical students' attitude towards artificial intelligence: a multicentre survey. European Radiology. 2019;29(4):1640-1646.
Grunhut J, Marques O, Wyatt ATM. Educating the educators: a cross-sectional survey of AI in medical education. Medical Science Educator. 2022;32:771-780.
Mousavi Baigi SF, et al. Medical students' knowledge and skills in working with artificial intelligence: a systematic review. Medical Education Online. 2024.
Li X, et al. Generative AI as a teaching assistant in case-based learning: a controlled comparative study. Medical Education. 2025.
Çiçek B, et al. ChatGPT-generated feedback versus expert feedback in clinical reasoning skill acquisition: a randomized controlled trial. Academic Medicine. 2025.
Montagna F, et al. Comparison of clinical decision-support systems: ChatGPT versus clinical practice guidelines. Journal of Medical Internet Research. 2025.
Nwe CM, et al. Perceived educational impact of generative AI among preclinical medical students: a cross-sectional survey. Medical Education. 2025.
Chen Y, et al. Does a virtual simulation teaching platform improve surgical training for medical undergraduate students? BMC Medical Education. 2025.
Mavrych V, et al. Comparative analysis of ChatGPT-4, Copilot, PaLM, and Bard for medical education. Journal of Medical Education. 2024.
Al-Khater K. ChatGPT accuracy in anatomy questions: a comparative study with Gemini. Anatomical Sciences Education. 2024.
Lee J. ChatGPT's ability to provide personalized, real-time feedback in anatomical education. Medical Teacher. 2024.
Integrating AI into clinical education: evaluating general practice trainees' ability to detect AI-generated hallucinations. BMC Medical Education. 2025;25:Article ID 6916.
AI Use for Medical Students: Impact on Clinical Skill Acquisition and Retention. Advances in Medical Education and Practice. 2026.
Ethical considerations for teaching with artificial intelligence. Medical Education. 2024.
Weidener L, Fischer M. Proposing a principle-based approach for teaching AI ethics in medical education. JMIR Medical Education. 2024;10:e55368.
Harnessing the potential of AI in lifelong learning for medical undergraduates. The Asia Pacific Scholar. 2026.
American Medical Association. AI frameworks for transparency, equity, and accountability in medical education. 2023.
Association of American Medical Colleges. Principles for ethical implementation of AI in medical education. 2025.