
Clinical Anatomy of the Cranial Nerves: A Systematic Review of Origin, Course, and Lesion Localization for Clinical Practice
1. Toychieva Zarina
(1. Professor, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
The cranial nerves form the principal communication pathway between the brain and the structures of the head, neck, and thoracoabdominal viscera. Their superficial and often crowded anatomical course through narrow skull base foramina, the cavernous sinus, the cerebellopontine angle, and the neck renders them vulnerable to a wide range of compressive, vascular, infective, traumatic, and neoplastic insults. Because each nerve has a predictable nuclear origin, intracranial trajectory, and peripheral distribution, the pattern of clinical deficit produced by a lesion can be used to localize disease with remarkable precision. This review presents a systematic, clinically oriented account of the anatomy of all twelve cranial nerves, integrating nuclear origin, course, and foraminal exit with the bedside examination findings and lesion syndromes that arise when each nerve, or group of nerves, is damaged. Particular attention is given to clinically important localizing syndromes, including cavernous sinus syndrome, cerebellopontine angle syndrome, jugular foramen syndrome, and the classical crossed brainstem syndromes, with the aim of providing a practical framework for the neurological and otolaryngological assessment of cranial nerve dysfunction.
Keywords: cranial nerves; clinical anatomy; brainstem; skull base; cavernous sinus; cerebellopontine angle; neuro-ophthalmology
Introduction
Twelve paired cranial nerves arise directly from the brain and brainstem to supply the special senses, the muscles of the head and neck, and a major share of the parasympathetic outflow to the thorax and abdomen. Unlike the spinal nerves, which follow a uniform segmental plan, each cranial nerve has its own nuclear configuration, intracranial trajectory, and skull base exit point, reflecting its distinct embryological origin and functional role.
Clinically, the cranial nerves are of disproportionate importance relative to their small size. Because they are gathered closely together at several anatomical “bottlenecks” — the cavernous sinus, the superior orbital fissure, the internal acoustic meatus, the cerebellopontine angle, and the jugular foramen — a single small lesion can produce a recognisable combination of deficits that points directly to its location. This principle of pattern recognition, sometimes called cranial nerve localisation, underlies much of clinical neurology, neuro-otology, and neuro-ophthalmology.
This article reviews the clinical anatomy of each cranial nerve in turn — its nuclear origin, course, and point of exit from the skull — before turning to the bedside tests used to assess it and the lesion syndromes that result from its dysfunction. The final sections integrate this information into the major clinical localising syndromes and outline the investigations used to confirm a suspected diagnosis.
2. General Organisation of the Cranial Nerves
2.1 Functional Classification
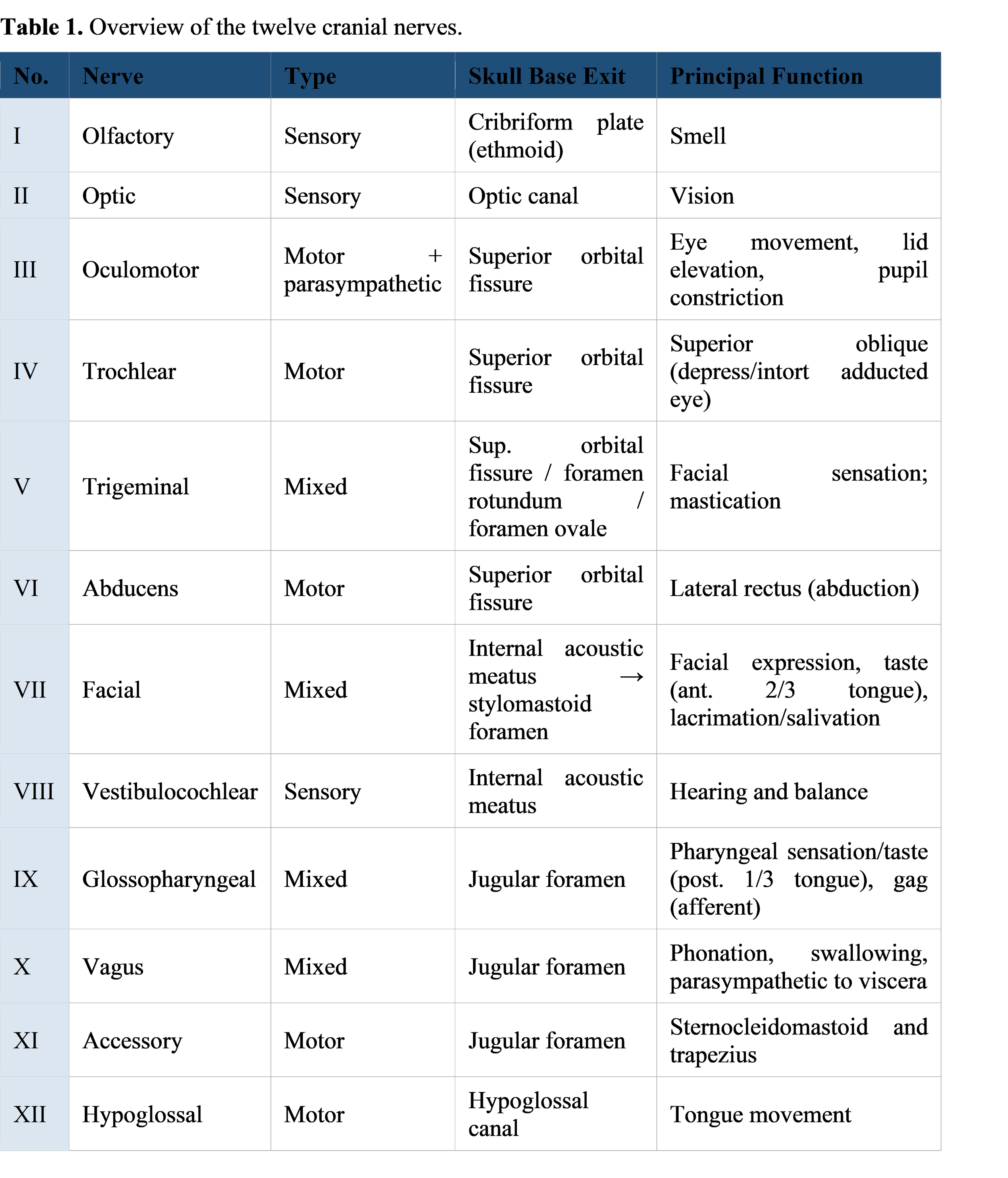
Cranial nerves are classified as purely sensory (CN I, II, VIII), purely motor (CN III, IV, VI, XI, XII), or mixed sensorimotor nerves that also carry autonomic fibres (CN V, VII, IX, X). Four nerves — III, VII, IX, and X — additionally carry parasympathetic fibres to glands and smooth muscle, and CN VII, IX, and X carry special sensory (taste) fibres from the tongue and epiglottis.
2.2 True versus Apparent Origin
Each nerve has a “true” origin — the brainstem or cortical nucleus where its constituent neurons reside — and an “apparent” origin, the point at which it is visible emerging from the surface of the brain. CN I and II are unique in being outgrowths of the forebrain rather than true peripheral nerves; they are surrounded by meninges and cerebrospinal fluid rather than the endoneurium/perineurium/epineurium of true peripheral nerves, which explains why the optic nerve can become swollen in raised intracranial pressure (papilloedema) and inflamed in central nervous system demyelinating disease (optic neuritis).
2.3 Brainstem Attachment
With the exception of CN I and II, all cranial nerve nuclei lie within the brainstem, arranged broadly according to the embryological position of their motor, sensory, and autonomic columns. CN III and IV arise from the midbrain, CN V–VIII from the pons (and pontomedullary junction), and CN IX–XII from the medulla. CN IV is the only cranial nerve to emerge from the dorsal aspect of the brainstem and the only one to decussate fully before reaching its target muscle.
2.4 Skull Base Exit Points
Every cranial nerve leaves the cranial cavity through a specific foramen, canal, or fissure in the skull base. Because several nerves share a single foramen, a lesion at that site characteristically produces a combined deficit affecting all nerves that pass through it — the basis of the localising syndromes discussed in Section 4.
3. Detailed Clinical Anatomy of Individual Cranial Nerves
The following subsections present each cranial nerve in turn, summarising its nuclear origin, intracranial course, exit point, and principal function, followed by the bedside tests used in examination and the clinical correlation that follows from its dysfunction.
3.1 Olfactory Nerve (CN I)
Functional type: Special sensory
Nuclear origin: Bipolar olfactory receptor neurons in the olfactory mucosa of the superior nasal concha and septum (the only cranial nerve whose receptor cells are themselves the first-order neurons).
Course and key relations: Unmyelinated axons (fila olfactoria) pass through the cribriform plate to synapse in the olfactory bulb; the olfactory tract then projects to the primary olfactory cortex (uncus, entorhinal cortex) without an obligatory thalamic relay — unique among the senses.
Site of exit from skull: Cribriform plate of the ethmoid bone.
Principal function: Smell (special sensory, telencephalic in origin).
Bedside testing
• Test each nostril separately using a non-irritant odour (coffee, vanilla, soap).
• Avoid ammonia or other trigeminal irritants, which can produce a false-positive response via CN V.
Clinical correlation — Unilateral or bilateral anosmia. Common causes include head trauma (shearing of the delicate fila olfactoria at the cribriform plate), olfactory groove meningioma, frontal lobe tumours, and upper respiratory tract or viral infection (including post-viral anosmia). An olfactory groove meningioma causing ipsilateral anosmia with ipsilateral optic atrophy and contralateral papilloedema constitutes the Foster Kennedy syndrome.
3.2 Optic Nerve (CN II)
Functional type: Special sensory
Nuclear origin: Retinal ganglion cells; the optic nerve is a CNS white matter tract (a diencephalic outgrowth) rather than a true peripheral nerve, and is ensheathed by meninges.
Course and key relations: Optic nerve → optic chiasm (decussation of nasal retinal fibres) → optic tract → lateral geniculate nucleus of the thalamus → optic radiation → primary visual cortex of the calcarine sulcus. A branch synapses in the pretectal nucleus to mediate the pupillary light reflex.
Site of exit from skull: Optic canal (lesser wing of sphenoid).
Principal function: Vision and the afferent limb of the pupillary light reflex.
Bedside testing
• Visual acuity (Snellen chart) and visual fields by confrontation.
• Direct and consensual pupillary light reflex.
• Fundoscopy to inspect the optic disc for pallor (atrophy) or swelling (papilloedema).
Clinical correlation — Monocular visual loss localises to the nerve itself (e.g. optic neuritis, ischaemic optic neuropathy). Bitemporal hemianopia localises to the chiasm (classically a pituitary macroadenoma compressing decussating nasal fibres). Homonymous hemianopia localises to the optic tract, radiation, or occipital cortex on the side opposite the visual field defect. Papilloedema reflects raised intracranial pressure rather than a primary optic nerve lesion.
3.3 Oculomotor Nerve (CN III)
Functional type: Motor + parasympathetic
Nuclear origin: Oculomotor nucleus in the midbrain at the level of the superior colliculus, together with the adjacent Edinger–Westphal nucleus, which supplies parasympathetic fibres.
Course and key relations: Exits the midbrain in the interpeduncular fossa, passes between the posterior cerebral and superior cerebellar arteries (a site vulnerable to compression by posterior communicating artery aneurysms), runs in the lateral wall of the cavernous sinus, and enters the orbit through the superior orbital fissure.
Site of exit from skull: Superior orbital fissure.
Principal function: Motor supply to superior rectus, inferior rectus, medial rectus, inferior oblique, and levator palpebrae superioris; parasympathetic supply to the sphincter pupillae and ciliary muscle (pupillary constriction and accommodation).
Bedside testing
• Assess the range of eye movement in the cardinal positions of gaze.
• Inspect for ptosis and assess pupil size, symmetry, and reactivity to light.
Clinical correlation — A complete CN III palsy produces a down-and-out eye position, ptosis, and a fixed, dilated (mydriatic) pupil. Because the pupillomotor fibres run superficially in the nerve, compressive lesions (posterior communicating artery aneurysm, uncal herniation) characteristically involve the pupil early, whereas ischaemic/medical lesions (e.g. diabetic mononeuropathy) typically spare the pupil — a distinction of considerable clinical importance, since a pupil-involving CN III palsy warrants urgent vascular imaging to exclude an aneurysm.
3.4 Trochlear Nerve (CN IV)
Functional type: Motor
Nuclear origin: Trochlear nucleus in the midbrain at the level of the inferior colliculus.
Course and key relations: The only cranial nerve to exit the dorsal surface of the brainstem and the only one whose fibres fully decussate before reaching their target; it wraps around the brainstem, traverses the lateral wall of the cavernous sinus, and enters the orbit through the superior orbital fissure.
Site of exit from skull: Superior orbital fissure.
Principal function: Innervates superior oblique, producing depression and intorsion of the adducted eye.
Bedside testing
• Ask the patient to look down and in; weakness of depression in adduction suggests a CN IV lesion.
• Enquire about diplopia on downgaze, e.g. when reading or descending stairs.
Clinical correlation — Vertical diplopia worse on downgaze, often with a compensatory head tilt away from the affected side (to minimise extorsion and diplopia). CN IV is particularly susceptible to closed head injury because of its long, slender intracranial course
3.5 Trigeminal Nerve (CN V)
Functional type: Mixed (sensory + motor)
Nuclear origin: The largest cranial nerve, with four nuclei: the main sensory nucleus (pons, light touch), the spinal trigeminal nucleus (medulla and upper cervical cord, pain and temperature), the mesencephalic nucleus (midbrain, proprioception), and the motor nucleus (pons, muscles of mastication).
Course and key relations: Three peripheral divisions arise from the trigeminal (Gasserian) ganglion: the ophthalmic division (V1) traverses the cavernous sinus and exits via the superior orbital fissure; the maxillary division (V2) exits via foramen rotundum; and the mandibular division (V3) exits via foramen ovale, carrying the motor root with it.
Site of exit from skull: Superior orbital fissure (V1); foramen rotundum (V2); foramen ovale (V3).
Principal function: Sensory innervation of the face, scalp, cornea, and anterior two-thirds of the oral cavity; motor innervation of the muscles of mastication (masseter, temporalis, medial and lateral pterygoids).
Bedside testing
• Light touch and pinprick sensation in each of the three divisions, comparing sides.
• Corneal reflex (afferent limb — efferent is via CN VII).
• Palpate masseter and temporalis on clenching; test jaw opening against resistance (pterygoids) and the jaw jerk.
Clinical correlation — Trigeminal neuralgia produces paroxysms of severe, lancinating facial pain, classically triggered by light touch to a specific trigger zone. Structural lesions cause facial sensory loss, an absent corneal reflex, and weakness of mastication with deviation of the jaw toward the weak (lesioned) side on opening
3.6 Abducens Nerve (CN VI)
Functional type: Motor
Nuclear origin: Abducens nucleus in the dorsal pons, encircled by the looping intra-axial fibres of the facial nerve (the facial colliculus).
Course and key relations: Has the longest intracranial subarachnoid course of any cranial nerve: it exits at the pontomedullary junction, ascends along the clivus, pierces the dura, and traverses the cavernous sinus (uniquely, within the body of the sinus rather than its lateral wall) before exiting via the superior orbital fissure.
Site of exit from skull: Superior orbital fissure.
Principal function: Innervates the lateral rectus, producing abduction of the eye.
Bedside testing
• Assess lateral (outward) gaze in each eye.
• Ask about diplopia that worsens with distance vision and on lateral gaze.
Clinical correlation — Medial deviation of the affected eye (esotropia) with horizontal diplopia maximal on attempted abduction. Because of its long, unsupported intracranial course, CN VI is especially vulnerable to stretch from raised intracranial pressure, producing a CN VI palsy that does not localise to the site of the underlying lesion — a classic “false localising sign.”
3.7 Facial Nerve (CN VII)
Functional type: Mixed (motor + special sensory + parasympathetic)
Nuclear origin: Facial motor nucleus in the pons; the closely associated nervus intermedius carries special sensory (taste) fibres from the anterior two-thirds of the tongue via the chorda tympani, parasympathetic secretomotor fibres to the lacrimal, submandibular, and sublingual glands, and general sensation from the external auditory canal.
Course and key relations: Exits at the pontomedullary junction, traverses the internal acoustic meatus with CN VIII, passes through the facial canal of the temporal bone (forming the geniculate ganglion), crosses the middle ear cavity, and exits the skull through the stylomastoid foramen before arborising within the parotid gland into five terminal motor branches supplying the muscles of facial expression.
Site of exit from skull: Internal acoustic meatus (entry); stylomastoid foramen (exit).
Principal function: Motor supply to the muscles of facial expression and stapedius; taste from the anterior two-thirds of the tongue; secretomotor supply to the lacrimal and submandibular/sublingual glands; minor cutaneous sensation from the external ear.
Bedside testing
• Ask the patient to raise the eyebrows, close the eyes tightly against resistance, smile, and puff out the cheeks.
• Test taste on the anterior tongue and assess for hyperacusis (loss of the stapedius reflex).
Clinical correlation — A lower motor neuron (LMN) lesion, as in Bell’s palsy, weakens the entire ipsilateral face, including the forehead. An upper motor neuron (UMN) lesion, as in stroke, spares the forehead because of bilateral cortical innervation of the frontalis muscle — the single most useful sign in distinguishing central from peripheral facial weakness. Geniculate ganglion involvement by herpes zoster (Ramsay Hunt syndrome) adds vesicles in the external auditory canal and may involve CN VIII.
3.8 Vestibulocochlear Nerve (CN VIII)
Functional type: Special sensory
Nuclear origin: Cochlear nuclei at the pontomedullary junction (hearing) and vestibular nuclei in the floor of the fourth ventricle (balance and eye-movement reflexes).
Course and key relations: The cochlear and vestibular divisions travel together through the internal acoustic meatus alongside CN VII before separating to reach their respective brainstem nuclei.
Site of exit from skull: Internal acoustic meatus.
Principal function: Hearing (cochlear division) and balance/equilibrium (vestibular division).
Bedside testing
• Whisper test and tuning fork tests (Rinne and Weber) to distinguish conductive from sensorineural hearing loss.
• Observe for nystagmus and assess gait and balance; Dix–Hallpike manoeuvre if positional vertigo is suspected.
Clinical correlation — Sensorineural hearing loss, tinnitus, and vertigo. A vestibular schwannoma (acoustic neuroma) arising at the cerebellopontine angle classically presents with progressive unilateral sensorineural hearing loss and tinnitus, later involving CN V and VII as it enlarges (see Section 4.2).
3.9 Glossopharyngeal Nerve (CN IX)
Functional type: Mixed
Nuclear origin: Nucleus ambiguus (motor), nucleus solitarius (visceral sensory and taste), and the inferior salivatory nucleus (parasympathetic) in the medulla.
Course and key relations: Exits the medulla as a series of rootlets and leaves the skull through the jugular foramen alongside CN X and XI.
Site of exit from skull: Jugular foramen.
Principal function: Motor supply to stylopharyngeus; taste and sensation from the posterior third of the tongue; sensation from the pharynx, middle ear, and the carotid body and sinus (chemo- and baroreceptor afferents); parasympathetic secretomotor supply to the parotid gland; afferent limb of the gag reflex.
Bedside testing
• Elicit the gag reflex (afferent limb — efferent is via CN X) and ask about taste on the posterior tongue.
• Assess swallowing and voice quality alongside CN X.
Clinical correlation — Isolated CN IX lesions are uncommon; they produce loss of the gag reflex, mild dysphagia, and, rarely, glossopharyngeal neuralgia (severe throat pain triggered by swallowing). CN IX is usually affected together with CN X and XI in jugular foramen syndrome.
3.10 Vagus Nerve (CN X)
Functional type: Mixed
Nuclear origin: Nucleus ambiguus (motor to pharynx and larynx), dorsal motor nucleus of the vagus (parasympathetic to thoracic and abdominal viscera as far as the splenic flexure), and nucleus solitarius (visceral sensory, taste from the epiglottis).
Course and key relations: Exits the medulla and leaves the skull through the jugular foramen, then descends within the carotid sheath in the neck. The recurrent laryngeal nerves branch from the vagus and loop beneath the aortic arch (left) and subclavian artery (right) before ascending to the larynx — a course that renders the left recurrent laryngeal nerve particularly vulnerable to mediastinal and apical lung pathology.
Site of exit from skull: Jugular foramen.
Principal function: Motor supply to the muscles of the pharynx and larynx (phonation and swallowing); parasympathetic supply to the heart, lungs, and gastrointestinal tract; sensation from the larynx, pharynx, and external ear; efferent limb of the gag reflex.
Bedside testing
• Inspect palatal elevation (the uvula deviates away from the side of the lesion) and assess voice quality for hoarseness.
• Test the efferent limb of the gag reflex and observe swallowing for aspiration risk.
Clinical correlation — Recurrent laryngeal nerve palsy produces hoarseness and a weak, breathy voice; it may follow thyroid or thoracic surgery, or compression by mediastinal or apical lung malignancy. Bilateral or brainstem vagal lesions cause dysphagia, loss of the gag reflex, and risk of aspiration.
3.11 Accessory Nerve (CN XI)
Functional type: Motor
Nuclear origin: Spinal accessory nucleus, formed by anterior horn cells of the upper five cervical spinal segments (C1–C5); the nerve is now generally regarded as a purely spinal motor nerve, with the historic “cranial root” considered part of the vagus.
Course and key relations: The spinal root ascends through the foramen magnum into the posterior cranial fossa before exiting again, together with CN IX and X, through the jugular foramen.
Site of exit from skull: Jugular foramen (with re-entry/exit via the foramen magnum).
Principal function: Motor supply to sternocleidomastoid (head rotation/tilt) and trapezius (shoulder elevation and scapular stabilisation).
Bedside testing
• Ask the patient to shrug the shoulders against resistance (trapezius) and to turn the head against resistance (sternocleidomastoid, contralateral to the direction of turning).
Clinical correlation — A CN XI lesion produces shoulder droop and scapular winging (trapezius) with weakness turning the head to the side opposite the lesion (sternocleidomastoid). The nerve is particularly vulnerable to iatrogenic injury during posterior triangle lymph node biopsy or neck dissection.
3.12 Hypoglossal Nerve (CN XII)
Functional type: Motor
Nuclear origin: Hypoglossal nucleus in the floor of the fourth ventricle, medulla.
Course and key relations: Exits the medulla via the preolivary sulcus and leaves the skull through the hypoglossal canal before passing forward in the neck to reach the tongue.
Site of exit from skull: Hypoglossal canal.
Principal function: Motor supply to all intrinsic and extrinsic muscles of the tongue except palatoglossus (which is supplied by the vagus via the pharyngeal plexus).
Bedside testing
• Ask the patient to protrude the tongue and inspect for deviation, wasting, and fasciculations.
Clinical correlation — In a lower motor neuron lesion, the protruded tongue deviates toward the side of the lesion, with ipsilateral wasting and fasciculations. In an upper motor neuron lesion the tongue deviates away from the side of the cortical lesion, without wasting or fasciculations.
4. Clinical Localisations: Cranial Nerve Syndromes
Because several cranial nerves are gathered together at specific anatomical sites, lesions at these sites produce recognisable combinations of deficits. Recognising these patterns allows the examining clinician to localise disease before imaging is obtained.
4.1 Cavernous Sinus Syndrome
The cavernous sinus is traversed by the internal carotid artery and its surrounding sympathetic plexus, and is flanked by CN III, IV, VI, and the ophthalmic and maxillary divisions of CN V (V1 and V2 lie in its lateral wall; CN VI runs within the body of the sinus itself). Lesions here — cavernous sinus thrombosis, pituitary apoplexy, carotid-cavernous fistula, meningioma, or aneurysm of the cavernous internal carotid artery — typically produce a combination of painful ophthalmoplegia (CN III, IV, VI), sensory loss in the V1/V2 distribution, proptosis or chemosis, and occasionally an ipsilateral Horner syndrome from disruption of the peri-carotid sympathetic fibres.
4.2 Cerebellopontine Angle Syndrome
The cerebellopontine angle is the site at which CN V, VII, and VIII lie in close proximity as they cross from the brainstem toward the internal acoustic meatus. A slowly growing mass here — most often a vestibular schwannoma (acoustic neuroma), less commonly a meningioma — produces a characteristic, sequential pattern: progressive sensorineural hearing loss and tinnitus (CN VIII) typically appear first, followed by facial weakness (CN VII) and facial numbness with an absent corneal reflex (CN V) as the lesion enlarges. Brainstem and cerebellar compression by a large lesion can add ipsilateral limb ataxia and, ultimately, hydrocephalus.
4.3 Jugular Foramen Syndrome (Vernet Syndrome)
CN IX, X, and XI pass together through the jugular foramen. A lesion here — classically a glomus jugulare (paraganglioma) tumour, but also trauma or metastatic disease — produces dysphagia and loss of the gag reflex (IX, X), hoarseness from vocal cord paralysis (X), and weakness of the trapezius and sternocleidomastoid (XI). Extension to involve the adjacent hypoglossal canal adds tongue weakness (Collet–Sicard syndrome), and further extension to involve the sympathetic chain or facial nerve produces the more extensive Villaret syndrome.
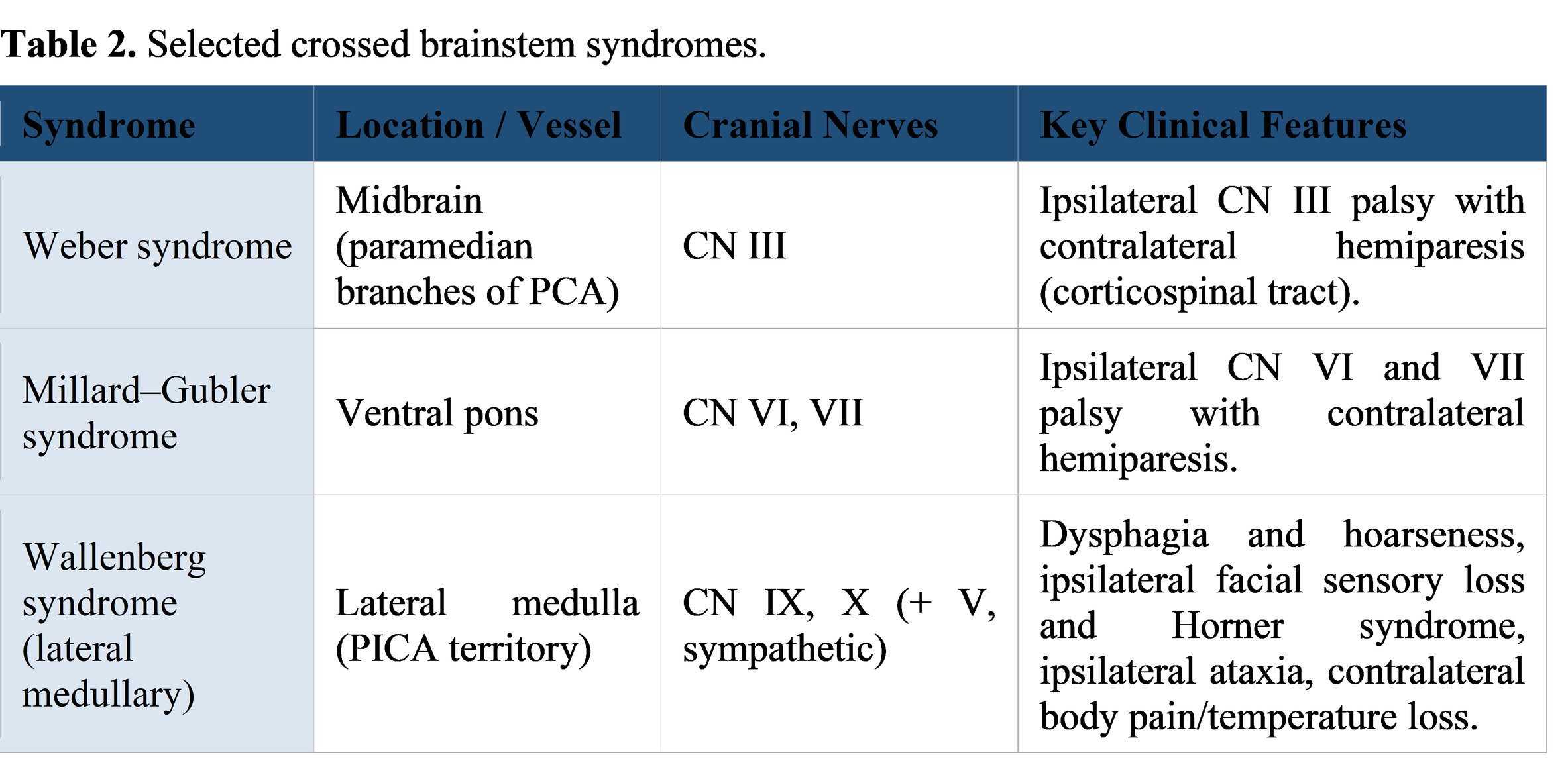
4.4 Crossed Brainstem (“Alternating”) Syndromes
Lesions within the brainstem itself — typically ischaemic strokes in a brainstem perforator or cerebellar artery territory — characteristically produce an ipsilateral cranial nerve palsy combined with a contralateral long-tract sign (hemiparesis or hemisensory loss), because the corticospinal and spinothalamic pathways have not yet decussated at the level of the lesion while the cranial nerve nucleus or fascicle has already exited on the same side.A
5. A Practical Approach to Cranial Nerve Examination
A systematic bedside examination groups the cranial nerves by region rather than testing them strictly in numerical order, which is both more efficient and more memorable:
• Smell and vision: CN I (smell, often omitted unless specifically indicated) and CN II (acuity, fields, pupils, fundoscopy).
• Eye movements and pupils: CN III, IV, and VI assessed together by examining the cardinal positions of gaze, eyelid position, and pupillary light reflex.
• Facial sensation and movement: CN V (facial sensation, corneal reflex, jaw muscles) and CN VII (facial expression, taste).
• Hearing and balance: CN VIII (whisper test, Rinne and Weber, nystagmus).
• Palate, pharynx, and larynx: CN IX and X assessed together (palatal elevation, gag reflex, voice, swallowing).
• Neck and tongue: CN XI (shoulder shrug, head turn) and CN XII (tongue protrusion).
Throughout, the examiner should specifically seek the distinguishing features described above — forehead sparing in facial weakness, pupil involvement in CN III palsy, and the direction of tongue or uvula deviation — since these details most often determine whether a lesion is central or peripheral, and where along the nerve it lies.
6. Diagnostic Imaging and Ancillary Investigations
Although cranial nerve disorders are diagnosed primarily on clinical examination, imaging and electrophysiological studies are frequently required to confirm the suspected lesion and guide management.
• MRI brain with thin sections through the internal acoustic meatus and contrast enhancement is the investigation of choice for suspected cerebellopontine angle lesions (vestibular schwannoma, meningioma) and for most causes of multiple cranial neuropathy.
• MR or CT angiography is indicated whenever a CN III palsy involves the pupil, to exclude a compressive posterior communicating artery aneurysm.
• High-resolution CT of the skull base demonstrates bony erosion or foraminal widening in jugular foramen and skull base tumours.
• Pure-tone audiometry and brainstem auditory evoked responses characterise and help localise CN VIII dysfunction.
• Nerve conduction studies and electromyography (e.g. of the facial nerve) provide prognostic information in selected peripheral cranial neuropathies.
• Lumbar puncture and cerebrospinal fluid analysis are indicated when an inflammatory, infective, or neoplastic (carcinomatous meningitis) cause of multiple cranial neuropathy is suspected.
7. Conclusion
The twelve cranial nerves occupy a disproportionately important place in clinical neurology because their tightly packed anatomical course through the skull base and cavernous sinus means that disease at a single site produces a distinctive, recognisable constellation of deficits. A secure understanding of the nuclear origin, intracranial trajectory, and foraminal exit of each nerve — together with the bedside signs that follow from its dysfunction — allows the clinician to localise a lesion accurately at the bedside, often before any imaging has been obtained. The localising syndromes discussed here — cavernous sinus syndrome, cerebellopontine angle syndrome, jugular foramen syndrome, and the crossed brainstem syndromes — represent the clinical application of this anatomy and remain central to the assessment of any patient presenting with cranial nerve dysfunction.
References
1. Snell RS. Clinical Neuroanatomy. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2019.
2. Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 8th ed. Philadelphia: Wolters Kluwer; 2018.
3. Standring S, ed. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Edinburgh: Elsevier; 2020.
4. Wilson-Pauwels L, Akesson EJ, Stewart PA, Spacey SD. Cranial Nerves: Function and Dysfunction. 4th ed. Shelton: PMPH-USA; 2013.
5. Ropper AH, Klein JP, Prasad S. Adams and Victor’s Principles of Neurology. 11th ed. New York: McGraw-Hill; 2019.
6. Blumenfeld H. Neuroanatomy through Clinical Cases. 3rd ed. Sunderland: Sinauer Associates / Oxford University Press; 2021.
7. Patten J. Neurological Differential Diagnosis. 2nd ed. London: Springer; 1996.
8. Fuller G, Manford M. Neurology: An Illustrated Colour Text. 4th ed. Edinburgh: Elsevier; 2021.