
A Comprehensive Review of the Clinical Classification of Tuberculosis in the Era of Precision Medicine
1. Kurmanaliev Nurlan Kambaralyevich
2. Aditi Kshirsagar
Darshani Dhiwar
Gargi Patodekar
Gayatri Jadhav
Harsh Anerao
(1. Teacher, International Medical Faculty, Osh State University, Kyrgyzstan)
https://orcid.org/0000-0002-5952-1463
(2. Students, International Medical Faculty, Osh State University, Kyrgyzstan)
Abstract
The clinical classification system for tuberculosis (TB) has experienced fundamental changes since Robert Koch discovered Mycobacterium tuberculosis in 1882. The medical profession and research institutions and public health authorities have followed the dual system which divides tuberculosis into latent TB infection and active TB disease for more than 40 years. Advanced imaging and molecular di- agnostics and longitudinal cohort studies have revealed a complex range of host- pathogen interactions that go beyond initial scientific findings. The article analyzes the historical development of TB classification systems while assessing the International Consensus for Early TB (ICE-TB) framework and evaluating new findings from PET-CT imaging which enhance our knowledge about subclinical disease conditions. The article examines how new classification systems will impact clinical practice because they will lead to new treatment methods and new vaccine research and new strategies for worldwide disease elimination. The review shows that TB classification needs a precision medicine approach because it serves as an essential solution to the ongoing disease spread which the existing binary system fails to control.
Keywords: Tuberculosis, clinical classification, latent tuberculosis infection, subclinical tuberculosis, ICE-TB framework, PET-CT imaging
Introduction
People die from tuberculosis because it remains the deadliest infectious disease which exists throughout the world and this disease kills more than 1.3 million people every year although effective treatment has existed for more than 70 years. The ongoing worldwide crisis shows that our current understanding of TB must be reevaluated because it has created a conceptual framework which prevents us from controlling this disease. The medical field has existed since its beginning, but researchers have studied TB classification, which extends back to ancient times. Hippocrates and other ancient Greek doctors identified “phthisis” as a deadly disease that caused patients to experience cough and hemoptysis and progressive weight loss. The skeletal deformities found in Egyptian mummies from 2400 BC demonstrate that Pott’s disease has existed throughout human history because the disease affects bone structure. Robert Koch discovered the tubercle bacillus in 1882 which established the first microbial understanding of tuberculosis transmission and its related disease.
The need for consistent classification systems developed during the first half of the twentieth century. Dr. Edward Livingston Trudeau established the requirement for universal diagnostic criteria because he understood their importance for medical treatment and scientific exploration which informed his creation of the first Diagnostic Standards and Classification of Tuberculosis which the National Tuberculosis Association published in 1917. The mid-twentieth century saw multiple subsequent editions which established new standards through the inclusion of radiographic evidence and bacteriological test results as essential classification elements.
Public health organizations used the binary system that defines latent infection and active disease which became their standard practice for several decades. The system proved effective because it enabled health workers to identify cases while it established uniform procedures for treating patients with visible symptoms and it saved countless lives. The system did not effectively reduce disease spread or infection rates because the majority of tuberculosis patients fail to seek medical assistance for their condition. The traditional binary system needs to be modified according to Esmail and his team who discovered that people with subclinical disease can spread infectious agents without showing any signs of illness.
The review intends to achieve five objectives which are to connect the historical development of TB classification systems through time to their present state and to assess the new ICE-TB framework together with its supporting evidence and to combine new research results from advanced imaging studies which show the different stages of TB infection and to examine how better classification systems will affect both clinical practice and public health efforts and to determine which research areas need attention for better results from classification system advancements.
Methods
The narrative review combines historical documents, consensus statements, primary re- search studies, and clinical guidelines to establish its evidence base. The researchers performed a comprehensive literature search which used PubMed and MEDLINE and Google Scholar to find articles published between 1950 and 2024. The search terms which were used for the research included “tuberculosis classification” and “latent tuberculosis infection” and “subclinical tuberculosis” and “ICE-TB framework” and “PET-CT tuberculosis” and “tuberculosis spectrum disease.” The researchers identified additional sources by examining reference lists from retrieved articles and by consulting subject matter experts.
Researchers focused on the International Consensus for Early TB (ICE-TB) frame- work which developed this framework through an international Delphi exercise that included 71 participants from different fields and sectors and economic backgrounds and all regions of World Health Organization. The consensus process which reached its conclusion at a 2023 in-person symposium created a shared understanding of conceptual states and research terminology and existing research gaps.
Researchers obtained primary evidence about tuberculosis infection structural and metabolic heterogeneity from a prospective cohort study which tracked asymptomatic household contacts who tested positive through serial [18F] Fluorodeoxyglucose (FDG) PET-CT imaging and targeted invasive sampling at sites of abnormal uptake. The 2024 Thorax study delivers precise details about pre-clinical infection phenotypes which exist between clinical and infection states.
Results
The Historical Trajectory of TB Classification
The evolution of TB classification reflects parallel advances in diagnostic technology and pathophysiologic understanding. Table 1 summarizes key milestones in this evolution.
Table 1: Historical Milestones in Tuberculosis Classification
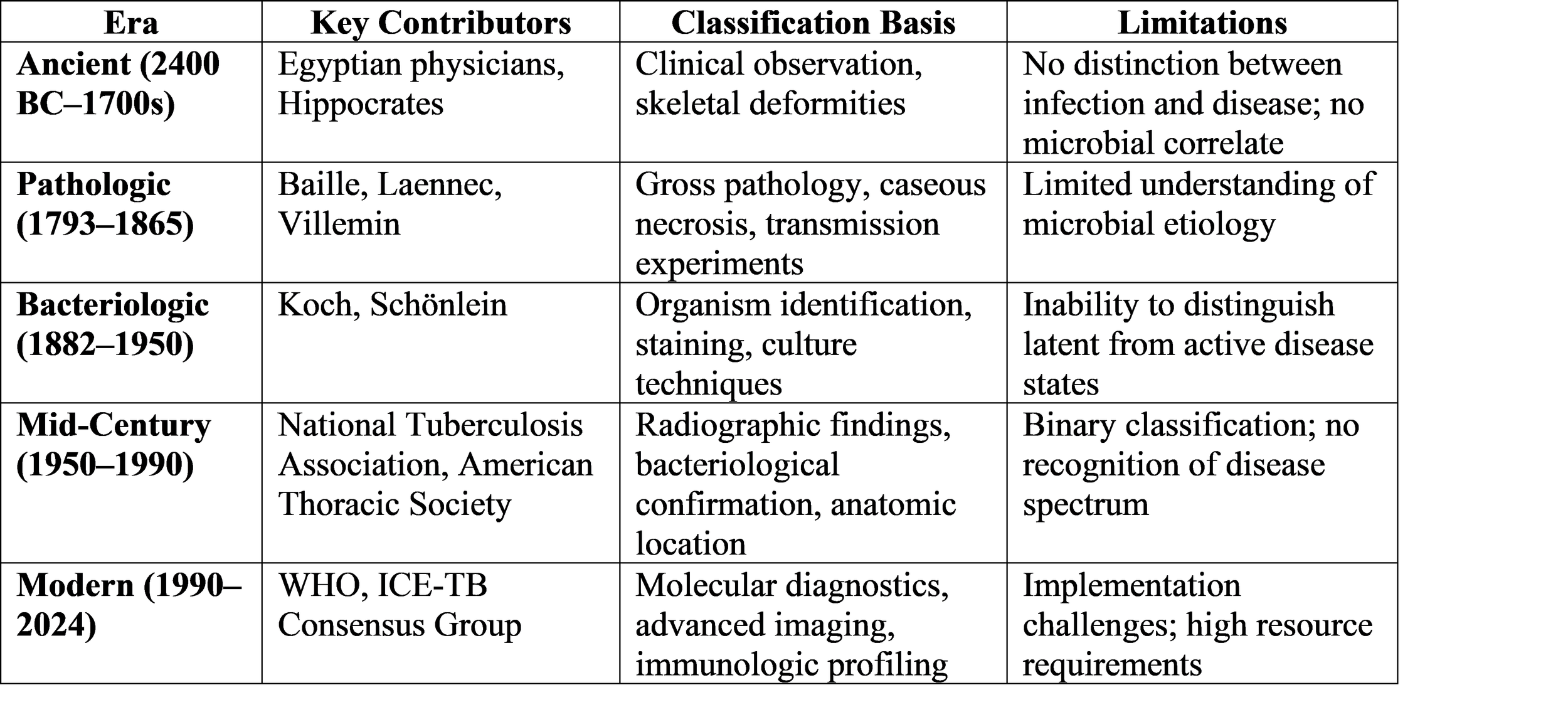
The morphological foundation which enables tuberculosis research began during the pathologic era which extended from the late 1700s until the mid-1800s. In 1793, Scottish pathologist Matthew Baille described caseous necrosis as “cheese-like” phthisic abscesses he termed “tubercles”. The French physician René Laennec who invented the stethoscope provided precise descriptions about disease progression which included details about lung development and miliary tubercles which grew into larger tubercles that contained caseous material and then transformed into pus before forming cavities. The experiment which Jean-Antoine Villemin conducted in 1865 showed that tuberculosis spreads through contact when he infected rabbits with purulent material from human tuberculous cavities and the rabbits developed the disease.
The bacteriologic revolution began with Koch’s 1882 announcement which depended on two technical innovations. The organism was named Mycobacterium tuberculosis in 1883. This discovery enabled researchers to identify actual infected individuals while establishing the disease as an infectious condition.
The Binary Paradigm: Latent Infection and Active Disease
The scientific understanding of tuberculosis throughout most of the twentieth century existed as a binary framework. Medical professionals considered people who had been infected with M. tuberculosis either to have latent TB infection (LTBI) or to show active symptoms of the disease. Diagnostic standards established through their multiple editions continue to influence medical practice today because healthcare professionals use tuberculin skin tests and interferon-gamma release assays (IGRAs) to determine test results as either “positive” (which shows infection) or “negative” (which shows no infection).
The binary public health system has delivered major public health benefits. The development of standardized treatment protocols for active disease which occurred during the 1940s and 1950s British Medical Research Council trials led to a substantial decrease in death rates. The initial use of isoniazid followed by rifamycin-based regimens for LTBI preventive therapy decreased the likelihood of progression for infected patients. Spanish health officials who created current guidelines recommend TB screen- ing for high-risk groups which include pulmonary TB contacts and people living with HIV and immunocompromised individuals. Healthcare providers should use 3HR treatment which combines daily isoniazid with rifampicin for three months.
The emerging evidence shows that the binary framework used for analysis does not meet its required standards of performance. The ongoing research from longitudinal studies shows that under 10 percent of recent TB contacts will develop the disease, which leads to the conclusion that more than 90 percent of LTBI patients would have remained healthy without treatment. The small number of events that occur in clinical trials requires researchers to obtain large participant groups while observing them for extended periods, which creates major obstacles for conducting their investigations. The binary system fails to classify people who have active pathogens which they can spread but who do not show any signs of illness because this group now receives recognition for its important role in disease distribution.
The ICE-TB Framework: A Five-State Model
The International Consensus for Early TB (ICE-TB) group introduced its new framework in March 2024 which establishes a five-state framework that differentiates between infection and disease while distinguishing between clinical and subclinical conditions which further divide into different levels of infectiousness. The framework presented in Table 2 shows its details.
The framework establishes its basic rule which states that all infection and disease states require both Mycobacterium tuberculosis and its corresponding host reaction to exist. The disease manifests through visible bodily damage which serves as a practical diagnostic method that works in various medical resource environments. The system differentiates between subclinical and clinical states through the existence of tuberculosis.
Table 2: The International Consensus for Early TB (ICE-TB) Framework
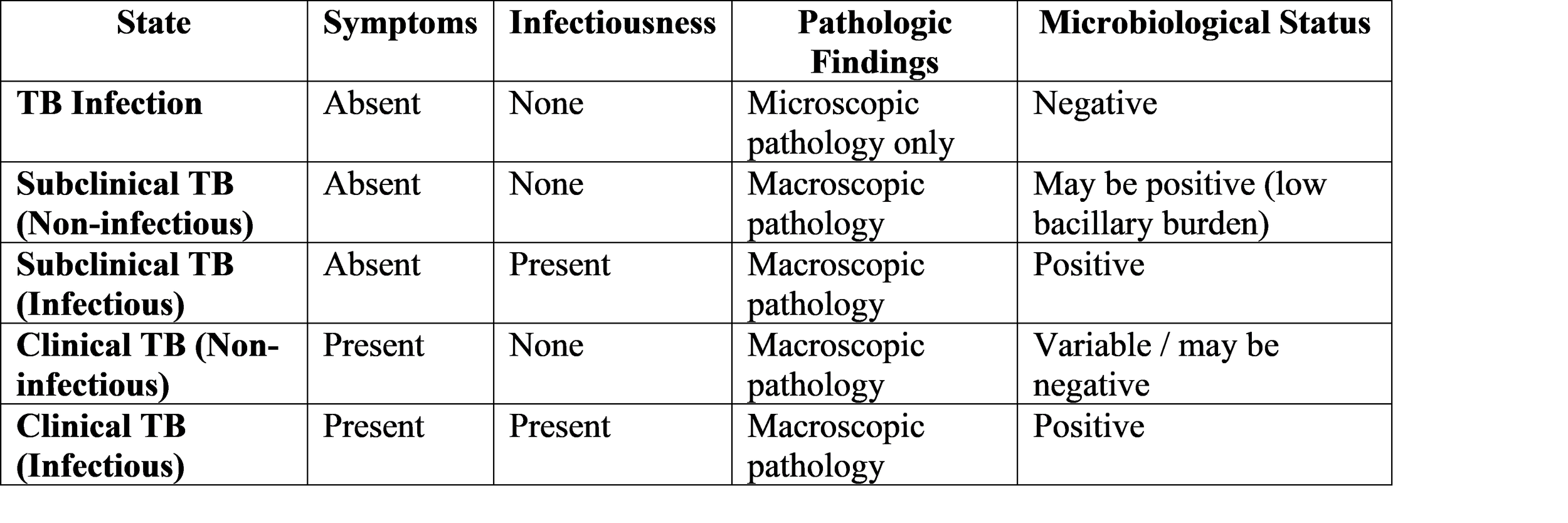
Source: Adapted from Esmail et al. (2024) and Coussens et al. (2024)
The ICE-TB framework establishes that infectiousness exists beyond two distinct states because it develops through various stages which include subclinical disease as a potential transmission element. The framework functions as a comprehensive tool for national tuberculosis programs because it includes all types of tuberculosis cases which encompass both extrapulmonary disease and pediatric patients.
Evidence from Advanced Imaging: Characterizing the Spectrum
The ICE-TB framework proves its ability to recognize intermediate states through high- resolution imaging research which shows this capacity. The 2024 prospective cohort study used [18F]FDG PET-CT to analyze structural and metabolic aspects of 16 asymptomatic household contacts who lived with pulmonary TB patients but showed normal chest radiographs and positive QuantiFERON-TB Gold Plus tests.
The study found four different ways of showing features which confirmed three dif- ferent ways that people with active TB infection show their symptoms (Table 3). The participants had two imaging sessions which occurred at the start and after three months. The researchers conducted targeted invasive sampling through bronchoalveolar lavage and endobronchial ultrasound-guided transbronchial needle aspiration to collect samples from areas showing active metabolism.
Several findings from this study merit emphasis. First, among participants with posi- tive PET and positive CT (Group 1), culture isolates of M. tuberculosis were obtained in three of four, and all received anti-tuberculosis therapy. The investigators propose that these features represent “an advanced state of pre-clinical infection that immediately precedes radiographically visible subclinical TB”.
Findings
Viable M. tu culosis prese Detectable conventional sampling Detectable conventional sampling Detectable conventional sampling Detectable conventional sampling Table 3: PET-CT-Defined Phenotypes of Tuberculosis Infection
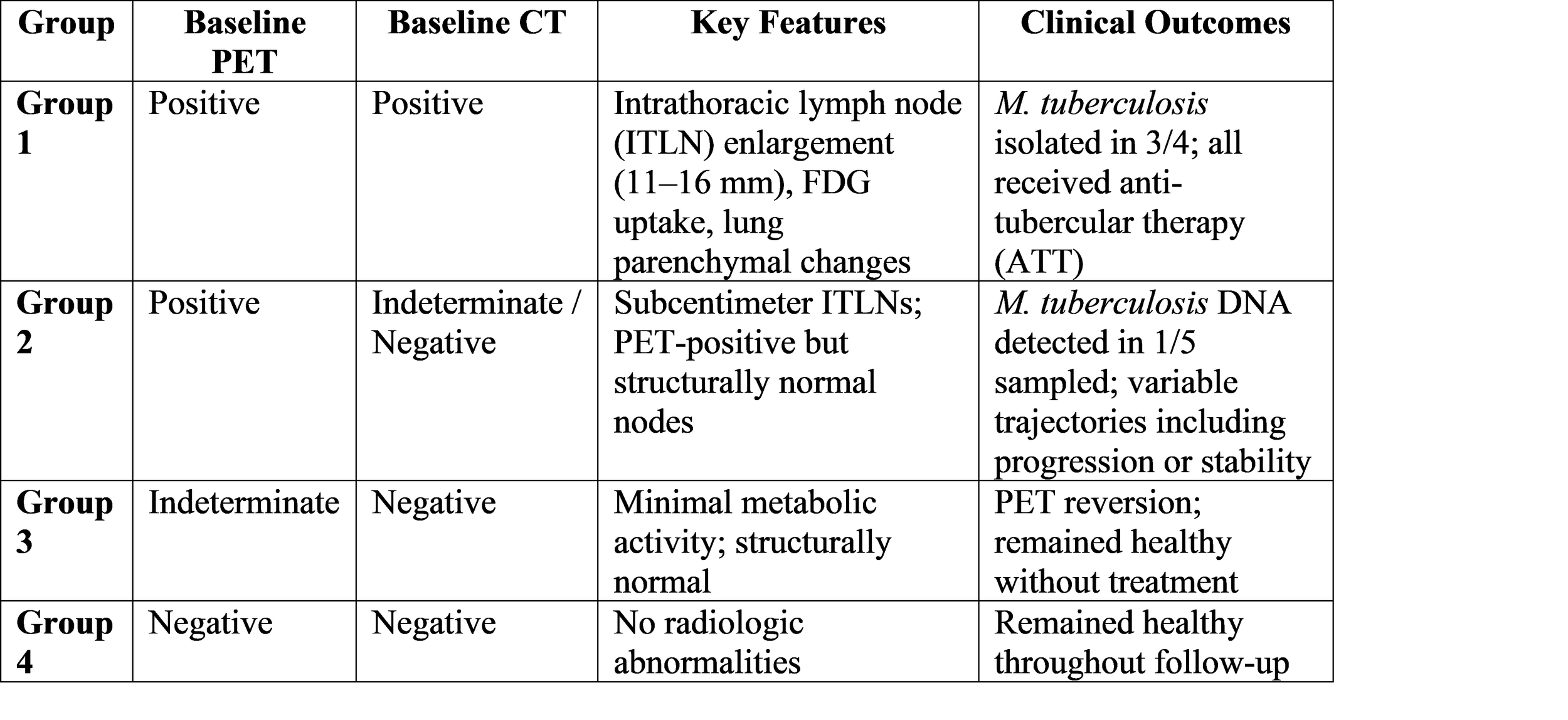
ITLN: intrathoracic lymph node; ATT: anti-tuberculosis therapy; FDG: fluorodeoxyglucose; PET: positron emission tomography; CT: computed tomography
Source: Data from Vozianova et al. (2024)
Second, the Group 2 participants (positive PET with indeterminate or negative CT) demonstrated remarkable heterogeneity in their three-month trajectories. One contact with stable PET changes developed symptoms after 18 months, with progressive FDG up- take at the original metabolic activity site and microbiologically confirmed intrathoracic lymph node TB. The study participants showed two outcomes which included resolution of indeterminate CT features that maintained stable PET activity and CT progression with PET changes that resolved. The evidence shows that people with infections display different paths which lead to disease development because some of them can control their early pathologic changes.
The participants of Group 3 which included participants with indeterminate PET and negative CT showed PET reversion through their treatment-free period during which they remained healthy. The minimal metabolic activity in the host may show transient containment which protects against active infection.
Anatomic and Drug-Resistance Classification
TB classification extends beyond its infectious disease classification by including both the specific body part affected and the patterns of resistance to treatment. These two aspects of medical practice serve as vital components for complete evaluation of the ICE- TB framework.
Anatomic Classification: Tuberculosis exists in three forms which include pulmonary TB that affects lung parenchyma and extrapulmonary TB that affects all other body parts and the combination of both forms. Droplet transmission primarily spreads pulmonary TB which constitutes 90 to 95 percent of all TB cases. Extrapulmonary TB can affect multiple areas of the body including pleura lymph nodes abdominal cavity genitourinary system skin bones and joints and meninges. Health authorities report patients with both pulmonary and extrapulmonary involvement as pulmonary TB cases.
Drug Resistance Classification: The World Health Organization recognizes several categories of drug-resistant TB:
• Mono-resistance: Resistance to one first-line anti-TB drug.
• Poly-resistance: Resistance to more than one first-line anti-TB drug, other than both isoniazid and rifampicin.
• Multidrug-resistant TB (MDR-TB): Resistance to at least isoniazid and rifampicin.
• Pre-extensively drug-resistant TB (pre-XDR-TB): MDR-TB with additional resistance to any fluoroquinolone.
• Extensively drug-resistant TB (XDR-TB): Resistance to any fluoroquinolone and at least one additional Group A drug (levofloxacin, moxifloxacin, bedaquiline, linezolid) in addition to MDR-TB.
The classification system establishes both the treatment methods and their respective time periods because drug-resistant conditions necessitate extended periods of specialized treatment which carries higher risks of severe side effects.
The Spectrum of TB Infection: A Unified Framework
A complete understanding of tuberculosis infection and disease can be achieved by combining evidence from immunology with imaging studies and clinical epidemiological research.
The spectrum framework establishes multiple key principles. First, the boundaries between states are fluid; individuals may transition in either direction depending on host immunity, bacterial factors, and environmental influences. Second, diagnostic test performance varies across the spectrum—for example, urine antigen detection becomes positive only in more extensive disease. Third, transcriptomic signatures may distinguish states before conventional diagnostics become positive, offering potential for early intervention.
Discussion
Clinical and Public Health Implications
The medical world needs to recognize tuberculosis as a disease that exists on a continuum instead of a condition that people either have or lack. The medical field will change because people now understand tuberculosis as a disease that exists on a continuum instead of a condition that people either have or lack.
Diagnostic Implications: The existing diagnostic methods work best for cases which show signs of the disease and have laboratory-confirmed bacterial infection. The ICE-TB framework highlights the need for tools capable of detecting subclinical disease and predicting progression risk. As Dheda and Migliori note, “no established method for determining the level of infectiousness in subclinical TB” currently exists. PET- CT systems provide research benefits but their design makes them unsuitable for use in regular medical practice. The development of accessible biomarkers – whether blood- based transcriptomic signatures, breath tests, or novel imaging approaches – represents a critical research priority.
Therapeutic Implications: The binary system creates a treatment protocol which uses one universal antibiotic solution to treat all patients who carry the most serious ver- sion of the disease. Shorter, simpler regimens may suffice for early disease states; Dheda and Migliori suggest that people with subclinical TB “could probably receive shorter ef- fective two-month treatment regimens”. The system will identify people who face the highest risk of disease progression, which allows for focused preventive treatment, while protecting 90% of the population who will never develop the disease from unnecessary medical procedures.
Transmission Implications: The study shows that subclinical TB transmission contributes to infectious spread which makes it impossible for case-finding methods that target only sick people to stop transmission routes. The ICE-TB framework enables active case-finding methods through its identification of contagious subclinical conditions which support both contact tracking and community screening initiatives that use advanced molecular testing methods.
Vaccine Development: Vaccine trials have traditionally used prevention of active disease as their primary endpoint. The ICE-TB framework suggests additional endpoints which include preventing subclinical disease and stopping infectees from developing any disease state. This expanded endpoint menu could accelerate vaccine development and enable evaluation of candidates that might not prevent disease entirely but could shift individuals toward more favorable positions on the spectrum.
Challenges and Limitations
The ICE-TB framework needs to overcome multiple implementation hurdles even though its framework shows conceptual value. First, the assessment of subclinical and clinical medical conditions depends on dependable symptom evaluation methods which face challenges because different groups show various symptom patterns that cultural elements and existing medical conditions and personal memory limitations affect. Second, the absence of symptoms makes it necessary to use validated proxies for infectiousness which include three types of proxies that lack standardization: radiographic findings and bacillary load and cough aerosol sampling. Third, the framework needs to develop simplified algorithms together with point-of-care tools which currently do not exist because most TB cases occur in low-resource environments that have high disease burden.
The PET-CT evidence provides valuable insights but needs testing with bigger and more varied groups because it comes from a small sample size of 16 QFT-positive participants. The study found that baseline PET and CT features showed only slight agreement (κw = 0.371), which demonstrates the intricate nature of infection state identification, which requires multiple assessment methods.
Research Priorities
The ICE-TB consensus process pinpointed various research priorities which need investigation.
1. Treatment optimization: Researchers need to discover the optimal antibiotic combination which maintains effectiveness through total treatment duration for all tuberculosis stages including subclinical tuberculosis infections.
2. Diagnostic development: The development of diagnostic tools requires the ability to differentiate between various infection stages while simultaneously assessing infectious potential and estimating disease advancement probabilities.
3. Natural history studies: Researchers will execute longitudinal cohort studies which use advanced phenotyping methods to track disease transitions while studying the factors that cause either disease advancement or recovery.
4. Transmission studies: Researchers will measure how subclinical disease spread contributes to disease transmission within communities by using molecular epidemiology and modeling methods.
5. Implementation science: The research examines how national TB programs should implement spectrum-based classification through training methods and recording and reporting systems and clinical decision support mechanisms.
Conclusion
The clinical classification of tuberculosis currently stands at a critical development point. The existence of two disease categories in tuberculosis medicine – active disease and latent infection – has been used by medical professionals and researchers since more than 100 years ago to study the disease which brought substantial advances for research but failed to achieve complete eradication. The International Consensus for Early TB framework introduces a new model which creates a continuum between two extreme points that includes subclinical cases and shows different levels of infectiousness while it establishes a basis for precise medical treatment development.
Advanced imaging studies provide evidence that supports the new conceptual frame- work because they show that people without symptoms who have normal chest radio- graphs show different structural and metabolic abnormalities which lead to different clinical development paths. The disease progression of some people with PET-CT abnormalities leads to the development of illness while others are able to manage or restore their condition without medical help. The field of TB research needs to develop methods that will help researchers understand how different factors lead to different outcomes.
The situation carries extreme importance. Tuberculosis remains the world’s leading infectious killer, not because we lack effective drugs, but because our conceptual frame- work has rendered millions of affected individuals invisible to the health system. The ICE-TB framework enables medical professionals to observe complete tuberculosis progression from infection to present-day clinical manifestations. The research community needs to create and test implementation tools for this conceptual advance to produce benefits at the population level while the global health community needs to use those tools in essential areas.
The ICE-TB authors created their framework, which provides “tuberculosis research direction that will lead to progress in both clinical treatment of tuberculosis and its elimination through development of better health policies.” The path from binary to spectrum is neither simple nor short, but it is essential. After 140 years of living with the tubercle bacillus since Koch’s discovery, we can no longer afford to see only half the picture.
References
[1] Coussens, Anna K., et al. “Classification of Early Tuberculosis States to Guide Re- search for Improved Care and Prevention: An International Delphi Consensus Exer- cise.” The Lancet Respiratory Medicine, vol. 12, no. 6, 2024, pp. 484–498. PubMed, doi:10.1016/S2213-2600(24)00128-1.
[2] Esmail, Hanif, et al. “New TB Framework for Improved Diagnosis and Care.” The Lancet Respiratory Medicine, 2024. Reported in MedicalBrief, 2 Apr. 2024, www.medicalbrief.co.za/new-tb-framework-for-improved-diagnosis-and-care/.
[3] Esmail, Hanif, et al. “New Tuberculosis Framework May Im- prove Research, Clinical Care.” MedPage Today, 27 Mar. 2024, www.medpagetoday.com/pulmonology/tuberculosis/109392.
[4] National Tuberculosis Association. “Diagnostic Standards and Classification of Tu- berculosis.” Journal of the American Medical Association, vol. 148, no. 5, 1952, p.
415. JAMA Network, doi:10.1001/jama.1952.02930050087031.
[5] NTEP India. “Discovery of Mycobacterium TB [M.tb].” National Tuberculosis Elimi- nation Programme, ntep.in/node/243/CP-discovery-mycobacterium-tb-mtb.
[6] “Recommendations on the Diagnosis and Treatment of Tuberculosis Infection: SEPAR/SEIMC/Spanish Ministry of Health Consensus Statement.” Archivos de Bronconeumología, 2026. PubMed, PMID: 41545280.
[7] “The Immunodiagnostic, Clinical and Radiological Features of the Spectrum of TB Infection.” Nature Reviews Disease Primers, 2024, Table 1. Nature.com, www.nature.com/articles/s41572-024-00504-2/tables/1.
[8] “Tuberculosis: Definitions and Classifications.” Estonian Tuberculosis Register, National Institute for Health Development, statistika.tai.ee/Resources/PX/Databases/Andmebaas/02Haigestumus/03Tuberkuloos/Tbinfo
[9] Vozianova, S., et al. “A Structural and Metabolic Framework for Classifying Pre-Clinical Tuberculosis Infection Phenotypes Using 18F-FDG PET-CT: A Prospective Cohort Analysis Following M. tuberculosis Exposure.” Thorax, vol. 79, no. 12, 2024, pp. e221470. PMC, doi:10.1136/thorax-2024-221470.