
Diabetes Mellitus in Children: An Indian Perspective
1. Endesh kyzy Gulsara
2. Tajamul Tariq
Sharwaq Waseem
Ali Ahmish
Shehroz Muhammad
Pankaj Kumar
Aboo Salman
Saleh Muhammad
Gulrukh Goni
(1. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Diabetes mellitus in childhood represents one of the most challenging chronic conditions facing pediatric healthcare providers in India today. With the highest number of children and adolescents with type 1 diabetes mellitus (T1DM) globally—estimated at approximately 95,600 prevalent cases and 15,900 new incident cases annually—the burden of pediatric diabetes in India demands urgent attention from clinicians, policymakers, and healthcare systems alike
This review examines the epidemiology, pathophysiology, clinical presentation, and management of diabetes mellitus in Indian children, with particular emphasis on the unique socioeconomic, cultural, and healthcare access challenges that characterize the Indian context. Drawing upon recent data from the International Diabetes Federation, the Indian Council of Medical Research's Young Diabetes Registry, and contemporary clinical practice guidelines from the International Society for Pediatric and Adolescent Diabetes (ISPAD), providing a comprehensive overview of current best practices while acknowledging the substantial gaps that remain in delivering equitable diabetes care to India's youngest patients. The discussion encompasses type 1 diabetes as the predominant form in childhood, the emerging epidemic of type 2 diabetes among adolescents, the often-overlooked monogenic forms of diabetes, and the critical importance of psychosocial support, transition care, and emerging technologies in optimizing outcomes for this vulnerable population.
Introduction
The landscape of pediatric diabetes in India has undergone profound transformation over the past three decades. What was once considered a relatively rare condition in Indian children has emerged as a significant public health concern, with India now bearing the unfortunate distinction of hosting the largest population of children with T1DM anywhere in the world
This dramatic increase in disease burden reflects not only improved survival and detection rates but also a genuine rise in incidence that parallels trends observed in many developing nations undergoing rapid socioeconomic transition.
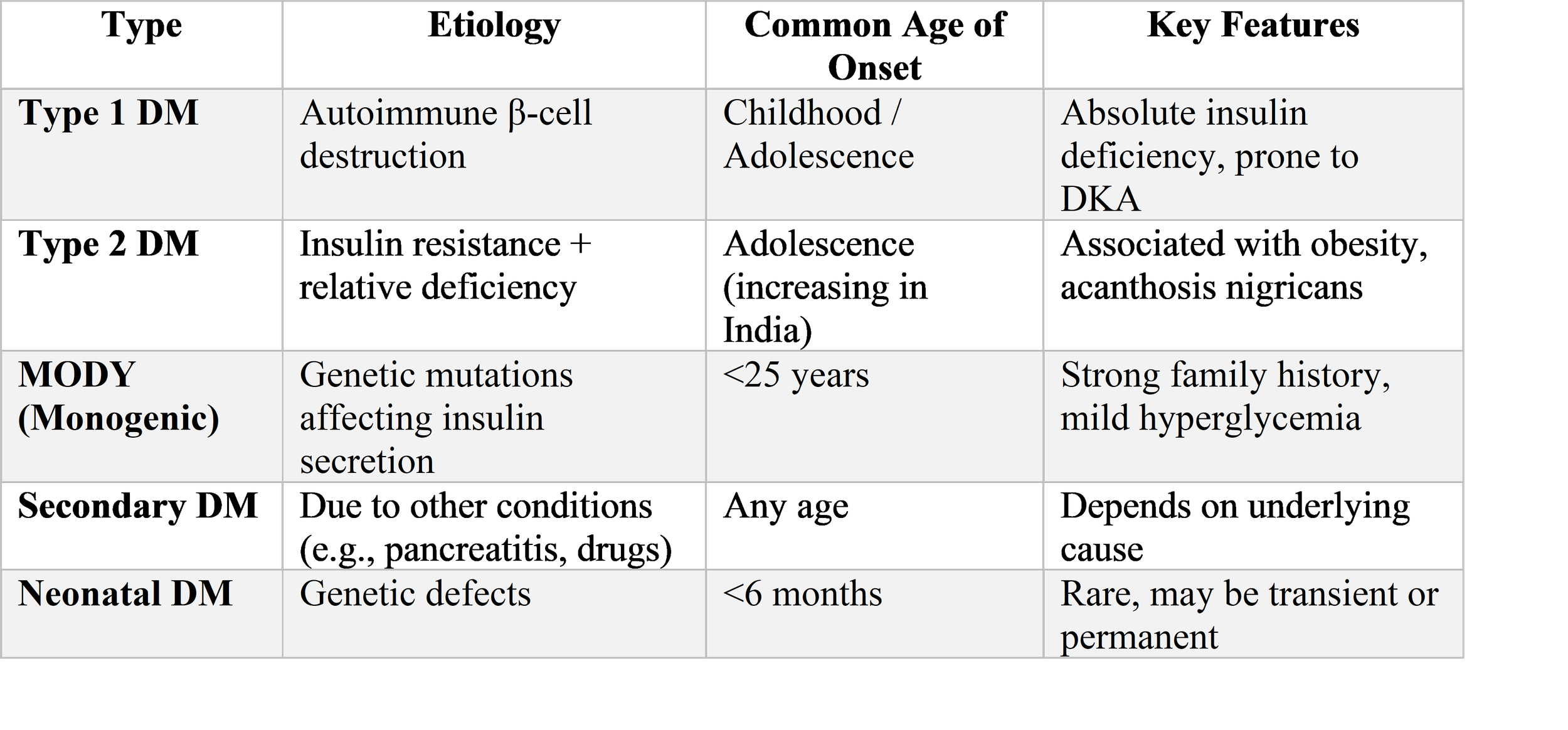
Diabetes mellitus in children encompasses a spectrum of disorders unified by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. While T1DM remains the predominant form encountered in pediatric practice, accounting for the vast majority of cases in prepubertal children, the past two decades have witnessed an alarming rise in type 2 diabetes mellitus (T2DM) among adolescents, particularly in urban areas where lifestyle changes have been most pronounced
Additionally, monogenic forms of diabetes, including maturity-onset diabetes of the young (MODY) and neonatal diabetes mellitus, represent important though frequently underdiagnosed entities that carry significant implications for treatment and genetic counseling
The management of pediatric diabetes in India occurs against a backdrop of remarkable diversity—in geography, socioeconomic status, dietary practices, healthcare infrastructure, and health literacy. A child with diabetes in a metropolitan private hospital in Delhi faces a fundamentally different set of challenges and opportunities compared to a similarly affected child in a rural district of Bihar or Odisha. This heterogeneity demands that clinicians not only possess technical expertise in diabetes management but also cultural competence and sensitivity to the socioeconomic realities that shape treatment adherence and outcomes.
The consequences of suboptimal diabetes management in childhood extend far beyond the immediate risks of diabetic ketoacidosis (DKA) and hypoglycemia. Children with diabetes face lifelong vulnerability to microvascular and macrovascular complications, with the duration of disease and quality of metabolic control during the growing years serving as critical determinants of long-term health. Moreover, the psychosocial burden of living with a chronic condition from childhood—navigating school, peer relationships, family dynamics, and emerging independence while managing an unrelenting medical regimen—cannot be overstated. Studies from across India have documented alarmingly high rates of psychological distress among children and adolescents with T1DM, with prevalence estimates exceeding 50% in several cohorts
The discussion integrates contemporary scientific evidence with practical clinical insights, emphasizing throughout the human dimensions of this condition—the fears of parents receiving the diagnosis, the daily struggles of children managing blood glucose fluctuations, the dedication of healthcare workers in resource-constrained settings, and the collective imperative to improve outcomes for this vulnerable population.
Methods
This narrative review was conducted through systematic literature searches of PubMed, PMC, and relevant Indian medical journals using combinations of the following search terms: "pediatric diabetes India," "type 1 diabetes children India," "type 2 diabetes adolescents India," "diabetic ketoacidosis management children," "continuous glucose monitoring India," "monogenic diabetes India," "psychosocial diabetes children India," and "diabetes transition care India." Priority was given to publications from 2020 onward, with particular attention to the 2024 ISPAD Clinical Practice Consensus Guidelines and recent studies from the Indian Council of Medical Research and major Indian medical institutions. The search strategy also incorporated grey literature from diabetes advocacy organizations operating in India, including the Diabetic Child Society and the International Diabetes Federation's Life for a Child program.
Information synthesis emphasized data relevant to the Indian context, including epidemiological studies from diverse geographic regions, clinical outcome data from Indian centers, and policy documents addressing diabetes care in resource-limited settings. The methodological approach prioritized integration of quantitative epidemiological data with qualitative insights regarding the lived experience of pediatric diabetes in India, recognizing that effective clinical care requires understanding both biological disease mechanisms and the social realities that shape health behaviors.
Results
Epidemiology and Disease Burden
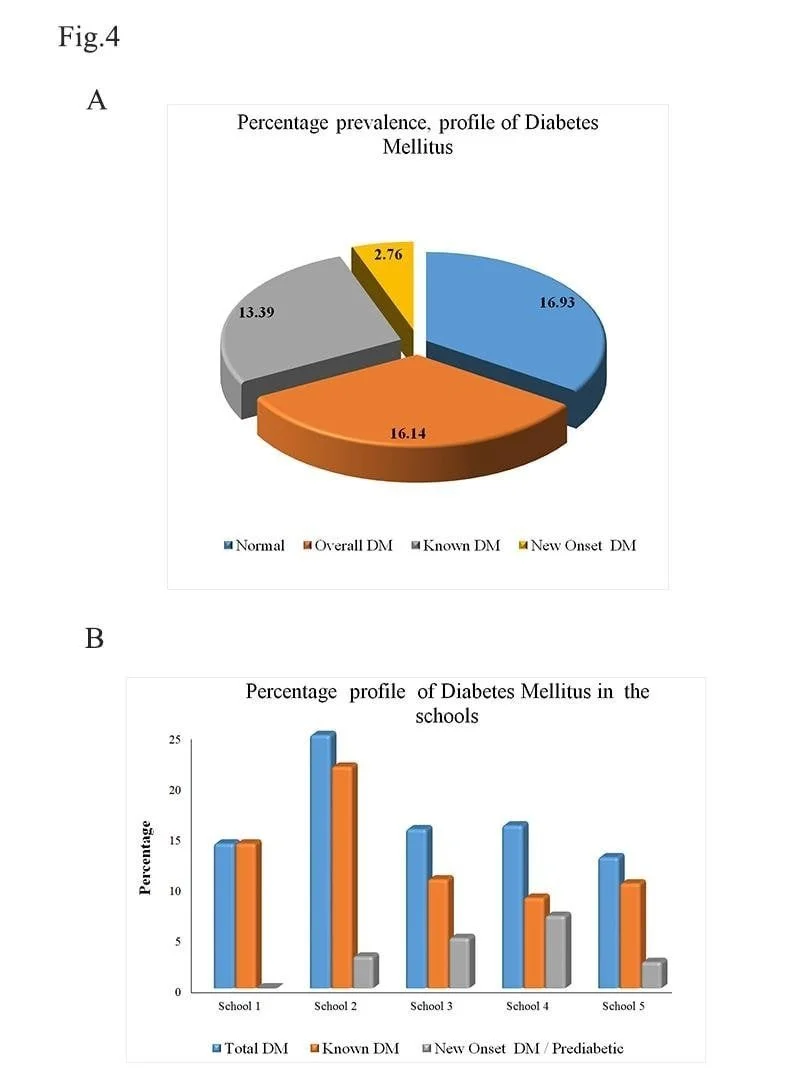
The epidemiology of pediatric diabetes in India reveals a complex and evolving picture. According to the International Diabetes Federation Atlas, India reports approximately three new cases of T1DM per 100,000 children aged 0–14 years annually. However, regional studies suggest substantial geographic variation in disease prevalence. The Karnataka state T1DM registry documented an incidence of 3.7 per 100,000 in boys and 4.0 per 100,000 in girls over 13 years of data collection, while studies in Karnal, Haryana, revealed striking urban-rural disparities with prevalence of 26.6 per 100,000 in urban areas compared to 4.27 per 100,000 in rural districts. A school-based survey conducted under the National Program for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke examined over 92,000 children across Nainital, Ratlam, and Bhilwara, identifying suspected diabetes in 1.467% of participants—a figure that, while likely overestimating true T1DM prevalence given screening methodology, nonetheless underscores the magnitude of the challenge.
The demographic profile of Indian children with T1DM reveals certain consistent patterns. The mean age at diagnosis typically ranges between 8 and 10 years, though presentation in infancy and early childhood is well documented. A modest male predominance has been observed in multiple cohorts, with male-to-female ratios ranging from 1.1:1 to 1.4:1. Notably, socioeconomic patterns differ from those observed in Western populations. While early Indian registries suggested higher prevalence among affluent families, more recent hospital-based studies have identified substantial disease burden among lower middle and upper lower socioeconomic strata, likely reflecting improved access to diagnostic facilities among disadvantaged populations rather than a true shift in disease distribution
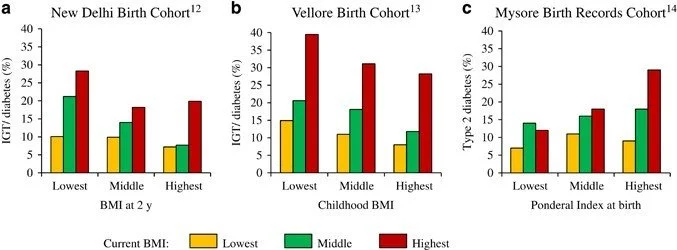
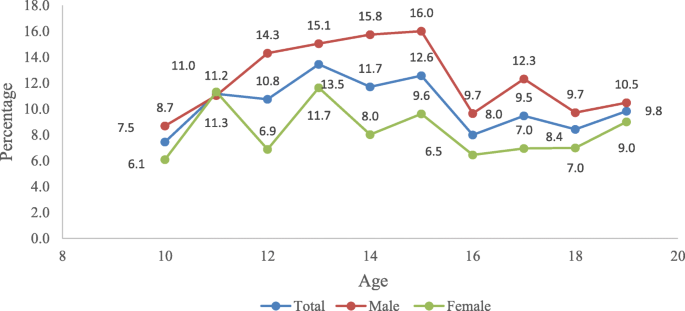
The emergence of T2DM in Indian adolescents represents a particularly concerning development. Traditionally considered a disease of middle-aged adults, T2DM now accounts for a growing proportion of diabetes cases among Indian teenagers, driven by the dual epidemics of childhood obesity and sedentary lifestyle. The National Family Health Survey-5 documented alarming rates of overweight and obesity among Indian adolescents, with subsequent studies demonstrating strong associations between adiposity measures and hyperglycemia in this age group. Particularly noteworthy is the phenomenon of "normal weight obesity" prevalent among Indian adolescents, wherein individuals with normal body mass index exhibit high body fat percentage and central adiposity, placing them at elevated metabolic risk despite appearing lean by conventional anthropometric criteria
This metabolic phenotype, increasingly recognized as characteristic of South Asian populations, complicates screening efforts and underscores the need for measures of central adiposity beyond simple body mass index calculations. Monogenic diabetes, though accounting for only 1–5% of pediatric diabetes cases, represents an important diagnostic category given its implications for treatment selection and genetic counseling. The most common varieties identified in Indian tertiary care centers include HNF1A-MODY, HNF4A-MODY, ABCC8-MODY, GCK-MODY, and HNF1B-MODY.
Neonatal diabetes mellitus, defined as diabetes with onset before six months of age, constitutes a medical emergency requiring urgent genetic diagnosis, as many cases result from mutations in KCNJ11 or ABCC8 genes that respond dramatically to sulfonylurea therapy, potentially allowing insulin discontinuation. The establishment of the Monogenic Diabetes Registry at the Madras Diabetes Research Foundation represents an important step toward systematic characterization of these rare forms in the Indian population.
Clinical Presentation and Acute Complications
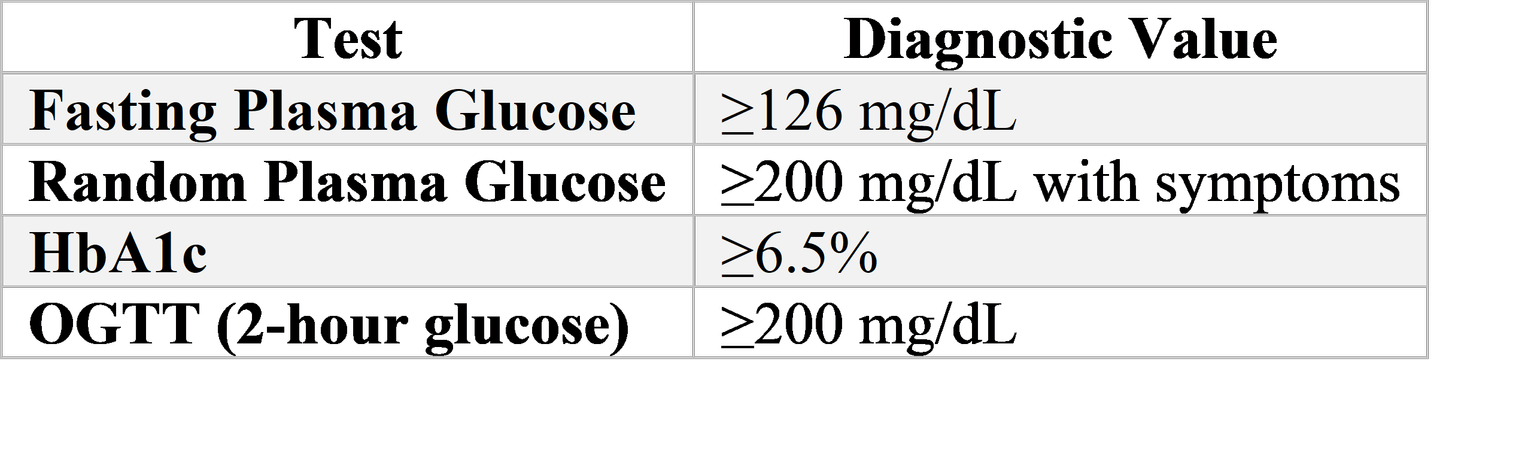
The clinical presentation of T1DM in Indian children follows patterns familiar to pediatric endocrinologists worldwide, with polyuria, polydipsia, and weight loss constituting the classic triad of presenting symptoms. A hospital-based study in Uttarakhand documented osmotic symptoms in over 90% of presenting children, with polyuria reported in 96.9% and polydipsia in 90.6% of confirmed T1DM cases. Weakness, weight loss, polyphagia, vomiting, and lethargy represent common accompanying features. Despite increasing awareness, a substantial proportion of Indian children continue to present with DKA, reflecting delayed recognition of symptoms in communities with limited diabetes awareness and restricted access to primary care.
DKA management in children requires particular attention to the unique vulnerabilities of the pediatric population. Current ISPAD guidelines and Indian clinical practice recommendations emphasize that pediatric DKA management differs fundamentally from adult protocols, with particular attention to fluid administration rates, timing of insulin initiation, and vigilance for cerebral edema—the most feared complication of DKA therapy. The management approach prioritizes restoration of circulatory volume with initial isotonic saline bolus (10–20 mL/kg), followed by careful replacement of estimated 5–10% dehydration over subsequent hours using 0.45% saline with dextrose added when blood glucose falls below 300 mg/dL
Insulin infusion at 0.05–0.1 units/kg/hour should commence only after initial fluid resuscitation and never as an intravenous bolus, with careful monitoring to ensure glucose decline does not exceed 50–150 mg/dL per hour. Potassium replacement must begin early, as acidosis masks profound total body potassium depletion, and bicarbonate administration is contraindicated in pediatric DKA due to risks of paradoxical central nervous system acidosis and cerebral edema. The "two-bag system"—simultaneous administration of dextrose-containing and dextrose-free fluids allowing precise titration of glucose delivery—has gained favor in many centers as a method to achieve smooth glycemic control during DKA resolution.
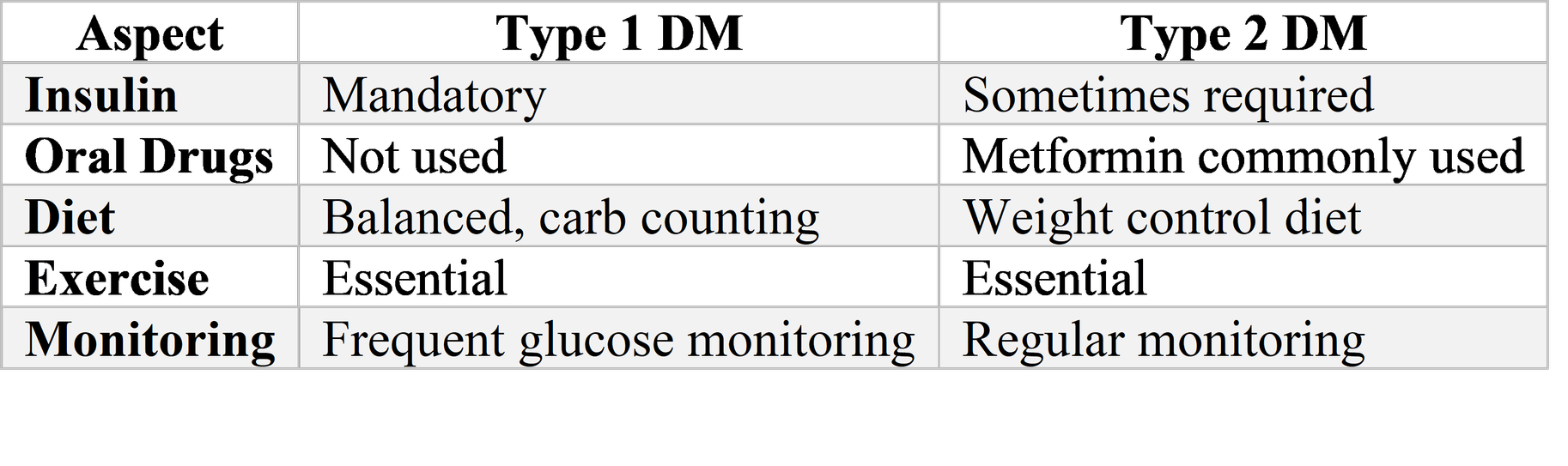
Chronic Management and Glycemic Targets
The chronic management of pediatric diabetes in India centers on insulin therapy for T1DM, with multiple daily injection (MDI) regimens representing the standard of care for most patients. The fundamental challenge lies in replicating physiological insulin secretion through exogenous administration—basal insulin to suppress hepatic glucose production between meals and overnight, and prandial insulin to manage post-meal glucose excursions. Conventional human insulins (regular and NPH) remain widely used in Indian public health facilities due to cost considerations, though analog insulins (rapid-acting lispro, aspart, glulisine; long-acting glargine, detemir, degludec) offer pharmacokinetic advantages that may translate into improved glycemic control and reduced hypoglycemia risk for appropriately selected patients.
The ISPAD 2024 guidelines emphasize that sensor-augmented pump (SAP) therapy—combining continuous subcutaneous insulin infusion with continuous glucose monitoring—demonstrates superior glycemic outcomes compared to MDI with self-monitoring of blood glucose, provided that sensor wear time exceeds 60% of the time.
However, the reality of diabetes technology access in India presents stark disparities. While affluent families in metropolitan centers may access insulin pumps and continuous glucose monitoring systems, the vast majority of Indian children with diabetes rely on conventional insulin injections with glucometer-based monitoring, if indeed they can afford regular glucose testing at all. The cost of diabetes care—including insulin, syringes, glucose monitoring supplies, and clinical consultations—imposes a crushing burden on many families, with documented instances of insulin rationing and catastrophic health expenditure. Flash glucose monitoring systems, particularly the FreeStyle Libre, have emerged as a more accessible technology option for some Indian families, with sensor costs approximately INR 2000 for 14-day wear representing a potentially cost-effective alternative to frequent fingerstick monitoring when utilized consistently.
Studies in Indian children have demonstrated the capacity of flash glucose monitoring to detect nocturnal hypoglycemia events that would otherwise remain unrecognized, with one pilot study documenting nocturnal hypoglycemia in 75% of participants wearing flash glucose monitors. The expansion of such technologies, along with telemedicine consultations and digital health tools, offers promise for improving diabetes care delivery in resource-constrained settings, though significant barriers to widespread adoption persist. Nutritional management of pediatric diabetes in India requires culturally sensitive adaptation of carbohydrate counting principles to Indian dietary patterns. Traditional Indian diets, with their emphasis on cereals (wheat, rice, millets), legumes, and seasonal vegetables, can be compatible with diabetes management when appropriate attention is paid to glycemic index, portion sizes, and meal timing
The incorporation of high-fiber, low-glycemic index grains such as unpolished millets, buckwheat, and amaranth can improve postprandial glycemic control while maintaining cultural acceptability. Traditional dairy products—milk, yogurt, buttermilk, and paneer—offer protein-rich options with modest carbohydrate content that serve well as between-meal snacks or bedtime treats to prevent nocturnal hypoglycemia. The challenge of managing festival foods, school meals, and social eating occasions requires ongoing education and support for families, emphasizing that no foods are absolutely forbidden but rather require appropriate insulin coverage and portion awareness.
Complications and Comorbidities
The complications of pediatric diabetes, both acute and chronic, demand systematic surveillance and prevention efforts. Screening studies in Indian cohorts have documented diabetic retinopathy in 3.6% of children, nephropathy in 3–7%, and sensory neuropathy in 3%, with prevalence increasing with disease duration and poor glycemic control. Dyslipidemia, characterized by elevated LDL cholesterol and triglycerides, affects approximately one-third of Indian children with diabetes, reflecting the interplay of genetic predisposition, dietary patterns, and glycemic status. The ISPAD 2024 guidelines recommend annual screening for dyslipidemia, nephropathy, retinopathy, and neuropathy beginning at diabetes onset for T2DM and after five years duration for T1DM, with earlier and more frequent assessment in high-risk individuals. Autoimmune comorbidities represent an important consideration in Indian children with T1DM, given the shared genetic susceptibility underlying autoimmune endocrinopathies. Screening for autoimmune hypothyroidism and celiac disease is recommended, with studies from Western India documenting celiac disease in nearly 25% and autoimmune hypothyroidism in 14% of children with T1DM. The prevalence of these associations in the broader Indian population remains incompletely characterized, suggesting the need for systematic multicenter studies.
Psychosocial Dimensions and Quality of Life
The psychosocial impact of childhood diabetes in India has received insufficient attention relative to its profound influence on outcomes. A cross-sectional study utilizing the Childhood Psychopathology Measurement Schedule documented psychological distress in 53.85% of pediatric T1DM patients, with anxiety, conduct disorder, and depression constituting the most common manifestations. Distress was significantly associated with increased frequency of insulin injections and noncompliance with dietary and drug regimens, creating a vicious cycle wherein psychological suffering impairs self-management, which in turn exacerbates glycemic instability and psychological distress.
Postpubertal males from rural areas, nuclear families, and lower socioeconomic backgrounds demonstrated particular vulnerability, highlighting the intersection of developmental stage, gender, geography, and economic constraint in shaping diabetes experience. The school environment represents a critical domain for children with diabetes, yet Indian schools have historically lacked systematic policies for supporting students with T1DM. Recent policy developments offer grounds for cautious optimism. The Central Board of Secondary Education issued a circular permitting student with T1DM to carry snacks, water, glucometers, and insulin pumps during examinations, while the National Commission for Protection of Child Rights directed all schools to allow glucose testing, insulin administration, and snack access during classes.
Kerala's pioneering "Mittayi Scheme" represents India's first government-supported comprehensive care program for children with T1DM, integrating medical care, diabetes education, and school-based support through linkages with pediatric endocrinologists, diabetes educators, and telemedicine follow-up. The Indian Society for Pediatric and Adolescent Endocrinology's "IDEAS" initiative provides online training modules for school staff in eight languages, aiming to build capacity for supporting students with diabetes across diverse educational settings.
Transition from Pediatric to Adult Care
The transition from pediatric to adult diabetes care represents a vulnerable period for emerging adults with T1DM, with documented risks of clinic non-attendance, deterioration in glycemic control, and acute complications during this transfer. Qualitative research in Delhi has revealed that only 10–50% of young adults with T1DM maintain recommended quarterly clinic follow-up, with visit frequencies as low as once every two to three years commonly reported due to geographic displacement, suboptimal provider relationships, and competing social and economic priorities. In response to these challenges, researchers at the All India Institute of Medical Sciences developed "PATHWAY" (Pediatric to Adult Transition Care for the Health and Wellness of Adolescents with Young Diabetes in India)—a structured 15-month transition program delivered by diabetes educators at pediatric and adult clinics, incorporating educational and behavioral sessions, a one-year overlap period of alternating visits between pediatric and adult providers, and attention to psychosocial drivers of care engagement. This program, currently undergoing randomized evaluation, represents an important adaptation of transition care principles to the Indian context, recognizing that successful transition support must address not only diabetes knowledge but also the economic constraints, geographic mobility, and evolving independence characteristic of emerging adulthood in contemporary India.
Discussion
The management of pediatric diabetes in India stands at an inflection point, characterized by simultaneous expansion of diagnostic capabilities, gradual improvement in treatment access, and persistent challenges rooted in socioeconomic inequality and healthcare system limitations. The sheer scale of the disease burden—nearly 100,000 children with T1DM and growing numbers with T2DM—demands that diabetes care be integrated into mainstream pediatric practice rather than remaining confined to specialized endocrine centers. This integration requires substantial investments in healthcare worker training, particularly at the primary care level where initial recognition of diabetes symptoms and prevention of DKA can be achieved through relatively modest educational interventions.
The disparities in diabetes technology access observed across Indian healthcare settings raise profound ethical questions about equitable care. While insulin pumps and continuous glucose monitoring systems offer genuine clinical benefits, their current cost places them beyond reach for the majority of Indian families. Advocacy for subsidized insulin, universal access to glucose monitoring supplies, and eventual inclusion of advanced diabetes technologies in public health programs must remain priorities for the diabetes community. In the interim, optimization of conventional insulin regimens through structured education, peer support, and telemedicine consultation represents a pragmatic approach to improving outcomes with existing resources.
The cultural adaptation of diabetes management to Indian contexts extends beyond dietary counseling to encompass family dynamics, gender roles, and community support systems. In many Indian families, the diagnosis of diabetes in a child mobilizes extended family networks, with grandparents, aunts, and uncles participating in care provision. This collective approach offers potential advantages for treatment adherence but may also generate conflict when generational differences in health beliefs emerge. The role of women—mothers and grandmothers primarily—as primary caregivers for children with diabetes intersects with broader patterns of gendered care work in Indian society, requiring that healthcare providers engage respectfully with family decision-making structures while ensuring that the child's emerging autonomy is supported, particularly as adolescence approaches.
The emergence of T2DM in Indian adolescents signals a need for expanded primary prevention efforts targeting childhood obesity and physical inactivity. However, the unique metabolic phenotype of Indian children—characterized by normal weight obesity and central adiposity—suggests that conventional BMI-based screening may miss substantial numbers of at-risk youth. Integration of waist circumference measurement and body composition assessment into routine pediatric care, alongside culturally appropriate promotion of active lifestyles and reduction of sedentary behavior, represents an important preventive agenda.
The psychosocial burden of pediatric diabetes documented in Indian studies demands integration of mental health support into routine diabetes care. The identification of depression, anxiety, and eating disorders in over half of affected children underscores that diabetes management cannot be reduced to glycemic metrics alone. The development of culturally adapted psychological interventions, peer support networks, and family-based therapies should accompany biomedical treatment advances. The diabetes camp model, exemplified by organizations such as the Diabetic Child Society in Visakhapatnam, offers a valuable approach to building community, reducing isolation, and delivering education in supportive group settings.
Looking forward, several developments offer promise for transforming pediatric diabetes care in India. The expansion of genetic testing for monogenic diabetes, with appropriate counseling and therapy modification when mutations are identified, represents a precision medicine opportunity particularly relevant given the treatability of some neonatal diabetes forms with sulfonylureas. The gradual reduction in costs of continuous glucose monitoring and the potential for indigenous manufacturing of diabetes technologies may eventually democratize access to these tools. The incorporation of diabetes care into national health insurance schemes and public health programs, building on models such as Kerala's Mittayi Scheme, could address the catastrophic financial burden currently borne by families. Finally, the growing recognition of T1DM as a condition warranting disability support and educational accommodation, while still incomplete, suggests gradual normalization of the condition in policy discourse.
Conclusion
Diabetes mellitus in children represents a significant and growing challenge for Indian healthcare, demanding coordinated responses across clinical, public health, and policy domains. The diversity of diabetes forms encountered in pediatric practice—from autoimmune T1DM through obesity-related T2DM to monogenic variants—requires diagnostic sophistication and individualized therapeutic approaches. The socioeconomic and cultural contexts that shape diabetes experience in India necessitate adaptation of international guidelines to local realities, with particular attention to the affordability of care, the cultural acceptability of dietary recommendations, and the family structures that support (or sometimes impede) treatment adherence.
The human dimensions of pediatric diabetes must remain central to clinical and research agendas. Behind every statistic on glycemic control or complication rates lies a child navigating school friendships while managing blood glucose fluctuations, a mother waking at midnight to check her toddler's sugar, a family making impossible choices between insulin purchases and other essential expenses. The goal of diabetes care extends beyond biochemical normalization to encompass the full flourishing of the child—academic achievement, social participation, psychological resilience, and the capacity to imagine a future unbounded by chronic disease.
India's response to the pediatric diabetes epidemic will serve as a test case for global health, demonstrating whether effective chronic disease management can be achieved at scale in resource-constrained settings. The foundations for success exist: dedicated healthcare professionals, growing scientific expertise, increasing policy attention, and resilient families determined to secure healthy futures for their children. Realizing the promise of these foundations will require sustained investment, equitable resource distribution, and unwavering commitment to the principle that every child with diabetes, regardless of geography or economic circumstance, deserves the opportunity to thrive.
References
Goyal S, Gupta S, Gupta N, Kalaivani M, Nongkynrih B, Guleria R, et al. Prevalence and associated clinical features of type 1 diabetes mellitus in children: A hospital-based study from North India. Indian Pediatr. 2024;61(1):28-33.
Choukem SP, Kanthem C, Neupane S, Sharma A, Bhattarai S, Sharma S, et al. Type 1 diabetes in India: Overall insights. World J Diabetes. 2024;15(4):462-478.
Pendsey EP. Incidence trends for childhood type 1 diabetes in India. Indian J Endocrinol Metab. 2012;16(Suppl 2):S334-S335.
Sahoo J, Sahoo B, Sahu S, Chakraverty A, Agrawal U. Diabetes in adolescents without obesity in India: An emerging concern. Indian J Endocrinol Metab. 2024;28(3):389-394.
Wolfsdorf JI, Allgrove J, Craig ME, Edge J, Glaser N, Jain V, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes. 2022;23(8):1310-1336.
Gokulakrishnan K, Amutha A, Priya M, Anjana RM, Ranjit U, Anbalagan VP, et al. Current recommendations for management of paediatric diabetic ketoacidosis. Indian J Endocrinol Metab. 2015;19(Suppl 1):S56-S64.
Dabla V. Prevalence of diabetic retinopathy in India: The global burden of diabetic retinopathy study. Indian J Ophthalmol. 2017;65(6):524-530.
Grover S, Bhadada S, Kate N, Sharma S, Bhansali A, Singh OP. Psychosocial morbidity among children with type-1 diabetes mellitus: A cross-sectional study from North India. J Pediatr Endocrinol Metab. 2017;30(6):643-648.
Kanthimathi S, Liju VB, Anjana RM, Mohan V, Radha V. Molecular diagnosis of maturity onset diabetes of the young in India. Indian J Med Res. 2015;142(4):393-401.
Sahoo J, Sahoo B, Mohanty S, Das S. Development and design of the first structured clinic-based program in lower resource settings to transition emerging adults with type 1 diabetes from pediatric to adult care: The PATHWAY study. Contemp Clin Trials Commun. 2024;42:101229.
Sood A, Kapoor M, Singh A. Using digital tools to improve diabetes care in India. J Diabetes Sci Technol. 2023;17(4):1015-1022.
Mohan V, Shah SN, Joshi SR, Seshiah V, Sahay BK, Banerjee S, et al. Current status of diabetes management in India: The National Diabetes Management Survey (NDMS) 2021. Diabetes Ther. 2023;14(5):891-903.
Dabadghao P, Bhatia V, Bhatia E, Singh R. The prevalence of type 1 diabetes mellitus and its association with autoimmunity in North India. Diabetes Res Clin Pract. 2011;91(1):94-99.
Vellanki P, Umpierrez GE. Diabetic ketoacidosis: Current diagnosis and management. Indian J Endocrinol Metab. 2012;16(Suppl 2):S163-S170.
Bhattarai S, Sharma A, Neupane S, Choukem SP. Ambulatory Flash Glucose Monitoring Device Detects Nocturnal Hypoglycemia in Children with Type 1 Diabetes Mellitus. J Nepal Paediatr Soc. 2024;44(2):e236.
Mohan V, Radha V. Neonatal and Maturity onset of youth registry india. Indian J Med Res. 2016;143(3):271-273.
Kanthimathi S, Anjana RM, Mohan V. Monogenic diabetes in children: An underdiagnosed and poorly managed clinical dilemma. Indian J Endocrinol Metab. 2015;19(Suppl 1):S45-S50.
International Diabetes Federation. IDF Diabetes Atlas (10th Edition). Brussels: International Diabetes Federation; 2023.
Indian Council of Medical Research. ICMR Guidelines for Management of Type 1 Diabetes in India. New Delhi: ICMR; 2017.
Unnikrishnan AG, Bhatia E, Bhatia V, Bhadada S, Sahay RK, Kannan A, et al. Type 1 diabetes: The Indian experience. Indian J Endocrinol Metab. 2011;15(Suppl 1):S13-S17.
Diabetic Child Society. Home [Internet]. Visakhapatnam: Diabetic Child Society; [cited 2026 Mar 18]. Available from: http://www.diabeticchildsociety.org.
Herold KC, Bundy BN, Long SA, Bluestone JA, DiMeglio LA, Dufort MJ, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Screening, Staging, and Strategies to Preserve Beta-Cell Function in Type 1 Diabetes. Pediatr Diabetes. 2024;25(8):1456-1472.
Joshi SR, Parikh RM, Joshi AA. 'Old Is Gold': How Traditional Indian Dietary Practices Support Diabetes Management. J Assoc Physicians India. 2023;71(3):11-13.
Zeitler P, Arslanian S, Fu J, Pinhas-Hamiel O, Reinehr T, Tandon N, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Type 2 Diabetes in Children and Adolescents. Pediatr Diabetes. 2024;25(8):1473-1490.
Maahs DM, Daniels SR, de Ferranti SD, Dichek HL, Flynn J, Golden SH, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Cardiovascular Risk Factors in Youth With Diabetes. Pediatr Diabetes. 2024;25(8):1491-1505.
Sherr JL, Tauschmann M, de Beaufort C, de Bock M, Frohnert BI, Haller MJ, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Diabetes Technologies - Insulin Delivery. Pediatr Diabetes. 2024;25(8):1506-1521.
Tauschmann M, Sherr JL, de Beaufort C, de Bock M, Frohnert BI, Haller MJ, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Diabetes Technologies - Continuous Glucose Monitoring. Pediatr Diabetes. 2024;25(8):1522-1542.
World Health Organization. A diabetes information kit: India. New Delhi: WHO Regional Office for South-East Asia; 2016.
Adolfsson P, Parkin CG, Thomas SM, Hinnen DA, Hartnell S, DePorte J, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Automated Insulin Delivery. Pediatr Diabetes. 2024;25(8):1543-1560.
Kapoor M, Sood A, Singh A. Making Indian schools type 1 diabetes friendly: Policy initiatives and implementation challenges. Indian J Pediatr. 2024;91(5):512-518.
Agarwal S, Yadav A, Gutch M, Kumar S, Jain N, Razi SM. Prevalence of celiac disease in type 1 diabetes mellitus in North India. J Gastroenterol Hepatol. 2011;26(4):718-722.