
Gallstones Disease
1. Kayipov Abdumazhit
2. Muskan Kumawat
3. Krushna Theng
4. Deepak Yadav
(1. Teacher, Surgery Dept., International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
3. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
4. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
ABSTRACT
One of the most prevalent hepatobiliary system illnesses is gallstone disease, which is defined by the development of solid concretions inside the biliary ducts or gallbladder. Gallstones are generally divided into three categories: cholesterol, pigment, and mixed stones. They are mostly caused by supersaturation of cholesterol, decreased gallbladder motility, and changes in bilirubin metabolism. Clinical manifestations include severe inflammatory consequences, biliary colic, and asymptomatic forms. A variety of hepatobiliary, gastrointestinal, renal, and cardiac disorders are included in differential diagnosis because of overlapping symptoms, especially discomfort in the right upper quadrant. When a stone blocks the cystic duct, it causes acute calculous cholecystitis, which can result in inflammatory changes that might lead to infection, empyema, gangrene, or perforation. Choledocholithiasis, obstructive jaundice, acute cholangitis, gallstone pancreatitis, and, in rare cases, gallstone ileus are further consequences of gallstone disease.
Keywords: hepatobiliary, choledocholithiasis, cholangitis, pancreatitis, empyema, gangrene, cholecystitis, calculous
INTRODUCTION
One of the most common digestive diseases in the world, gallstone disease (cholelithiasis) affects up to 15% of individuals in affluent nations. Gallbladder hypomotility, infection, and biochemical abnormalities in bile composition are the causes. Gallstones can result in considerable morbidity from inflammatory and obstructive problems or biliary discomfort, even though many individuals do not experience any symptoms. Ultrasonography's broad availability has improved detection, but treatment choices are still mostly based on symptoms and potential risks. To maximize patient results, it is crucial to comprehend the mechanics underlying gallstone development, clinical symptoms, and contemporary therapy alternatives. No large population-based ultrasonographic survey for gallstone prevalence has been published from Kyrgyzstan in major indexed journals as of current searchable data the total incidence of gallstone disease, cholecystitis, and cholangitis was almost 586.5 cases per 100,000 people in 2019, according to national health reporting statistics. Due to such scarce data we are using global estimates. As per data seen in many articles we have seen that ten to twenty percent of people in Europe have gallbladder stones. Many gallstones are quiet, but in over 40% of individuals over 40, symptoms and serious problems develop, requiring laparoscopic cholecystectomy. According to a recent study, women between the ages of 70 and 79 had the greatest prevalence rate of gallstones: 57% of them had either a history of cholecystectomy or present sonographic evidence of gallstones. The majority of Central and South American Hispanic communities, as well as American Hispanics of Native American heritage, have an even greater frequency of cholelithiasis. The populations of Native Americans in North and South America are the most vulnerable in the world.
Mechanism of gallstones formation:
Gallstones are categorized as pigment and cholesterol stones. The gallbladder is the site of formation for about 90% of gallstones, which are mostly composed of cholesterol. The principal cause of cholesterol stones is when bile contains more cholesterol than the combined micelles of bile salts and phosphatidylcholine (lecithin) can dissolve. Cholesterol microcrystals can be maintained and develop into macroscopic gallstones due to other variables such biliary mucus and decreased gallbladder movement. Gallstones normally forms when one of these process happens in body-
1. Supersaturation of Bile with Cholesterol: When the liver secretes bile that contains more cholesterol than phospholipids and bile salts can dissolve, the most frequent kind of cholesterol stones occur. The following are some of the factors causing this imbalance: Fatigue and metabolic disorders
Excessive intake of calories or cholesterol Hormonal factors (estrogen treatment, oral contraceptives, pregnancy)
Excessive weight loss or extended fasting
2. Elevated Excretion of Bilirubin: When bile contains too much unconjugated bilirubin, pigment stones develop. This might happen in: Hemolytic diseases that persist Cirrhosis of the liver
Infections of the biliary system Disorders that affect the circulation of bile acid
3. Hypomotility of the Gallbladder: Gallbladder stasis encourages crystal agglomeration and the consequent development of stones. Hypomotility is linked to: Diabetes Complete parenteral nourishment Damage to the spinal cord Extended periods of immobility
Types of Gallstones:
Cholesterol Stone- these we discussed above as these are the most common type of gallstones.
Black pigment stone- these stones make up a relatively little percentage of gallbladder stones (2%). Their main component is polymerized calcium bilirubinate, which progressively polymerizes in biliary sludge and precipitates if the ion product of calcium and unconjugated bilirubin surpasses its solubility product. The most evident causes of elevated unconjugated bilirubin are hemolytic anemias. Bile salt leakage into the colon due to ileal illness or resection is another possible mechanism. This leads to increased enterohepatic cycling and biliary production of bilirubin, as well as the solubilization and absorption of unconjugated bilirubin. The increased occurrence of gallstones in Crohn's disease and cystic fibrosis may be caused by this mechanism. The Gilbert syndrome-associated UGT1A1 promoter variation raises the risk of pigment stone development in individuals with hemolytic anemias and cystic fibrosis.
Brown pigment stone- secondary bile duct stones, or cholesterol stones that originate from the gallbladder and have a pigment shell, make up a large number of bile duct stones. Stasis and infection within the bile ducts cause brown pigment stones, also known as primary bile duct stones. Bilirubin precipitates as calcium salts of long-chain fatty acids as a result of bacterial β-glucuronidase converting soluble conjugated bilirubin back to the insoluble unconjugated state. As a result, this sort of stone is linked to parasites, biliary strictures, or duodenal diverticula.
Clinical signs:
Silent stones and serious consequences are only two of the symptoms of gallstone disease.
1. Asymptomatic Gallstones:
The majority of people don't exhibit any symptoms. Usually, these stones are found by chance. Unless difficulties occur, current recommendations advise against therapy.
2. Biliary colic:
Biliary colic is the primary sign of gallstone disease.
This is what makes it unique:
Abrupt onset of persistent, severe discomfort
Placement in the epigastrium or upper right quadrant
Radiating to the right shoulder, scapula, or back
30 minutes to many hours
The temporary blockage of the cystic duct by a stone causes the discomfort.
3. Chronic Calculous Cholecystitis:
Chronic inflammation, fibrosis, and thickening of the gallbladder wall are caused by repeated bouts of ductal blockage.
These are some of the symptoms:
Recurrent discomfort in the right upper quadrant after eating
Sensitivity to some foods, especially fatty ones
Bloating and dyspepsia
The differential diagnosis of this disease includes several diseases as the signs of gallstones resemble those of many different diseases.
Gastrointestinal conditions
· Acute pancreatitis
· Gastric or duodenal ulcer
· Gastroesophageal reflux
· Hepatitis
· Appendicitis (especially high retrocecal)
Cardiopulmonary conditions
· Myocardial ischemia
· Right-sided pneumonia
· Pleuritic chest pain
Renal conditions
· Renal colic
· Pyelonephritis
Ultrasound is the first-line test that separates gallstone disease from other gastrointestinal or cardiopulmonary conditions such as peptic ulcer, GERD, MI, pneumonia, or renal colic.
Research Data:
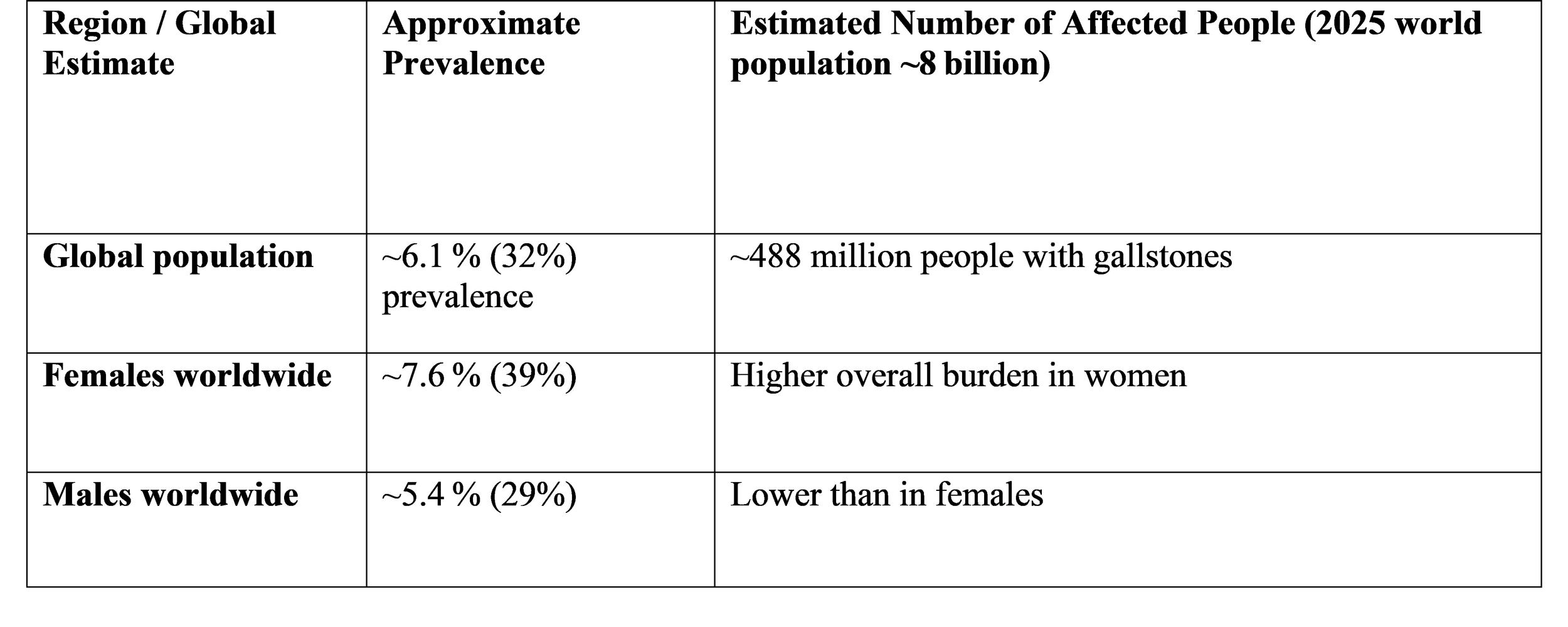
In this we will see the global burden of gallstones diseases. Worldwide prevalence: as per the data collected from pubmed approximately 6.1% of people worldwide suffer from gallstone disease. Accordingly, gallstones affect around 1 in 16 persons globally at any given moment.
Estimated Number of People Affected Worldwide:
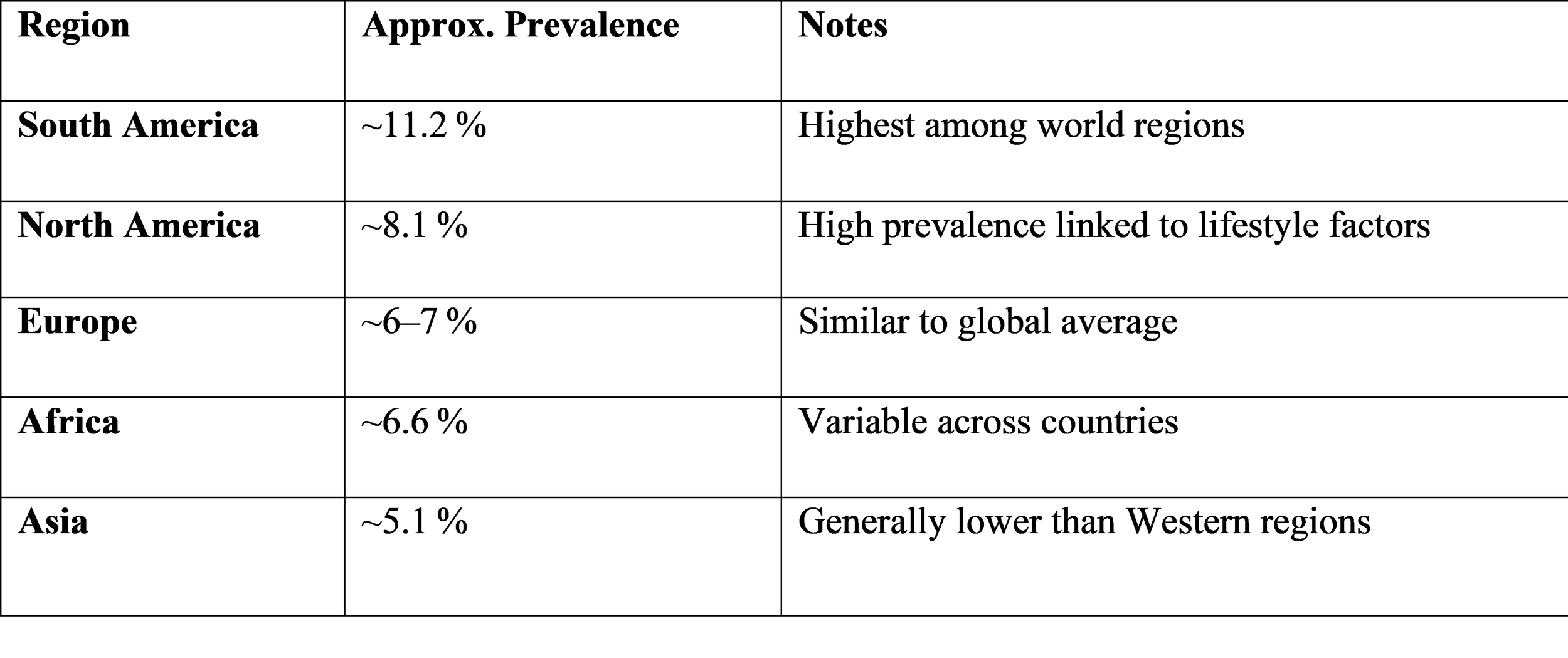
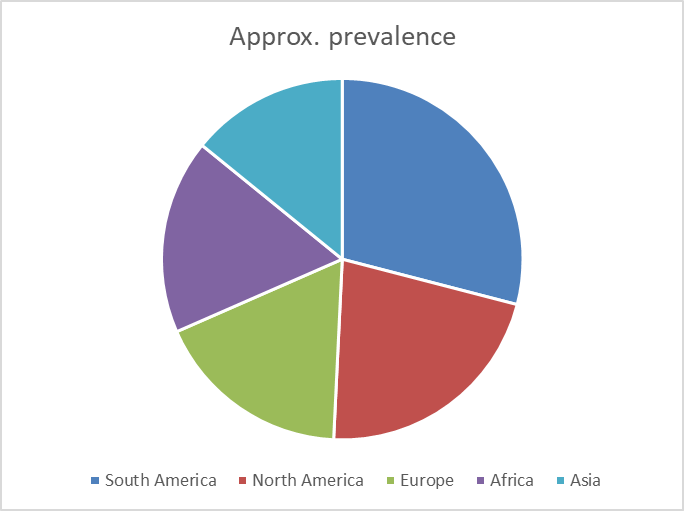
Regional Patterns in Gallstone Prevalence:
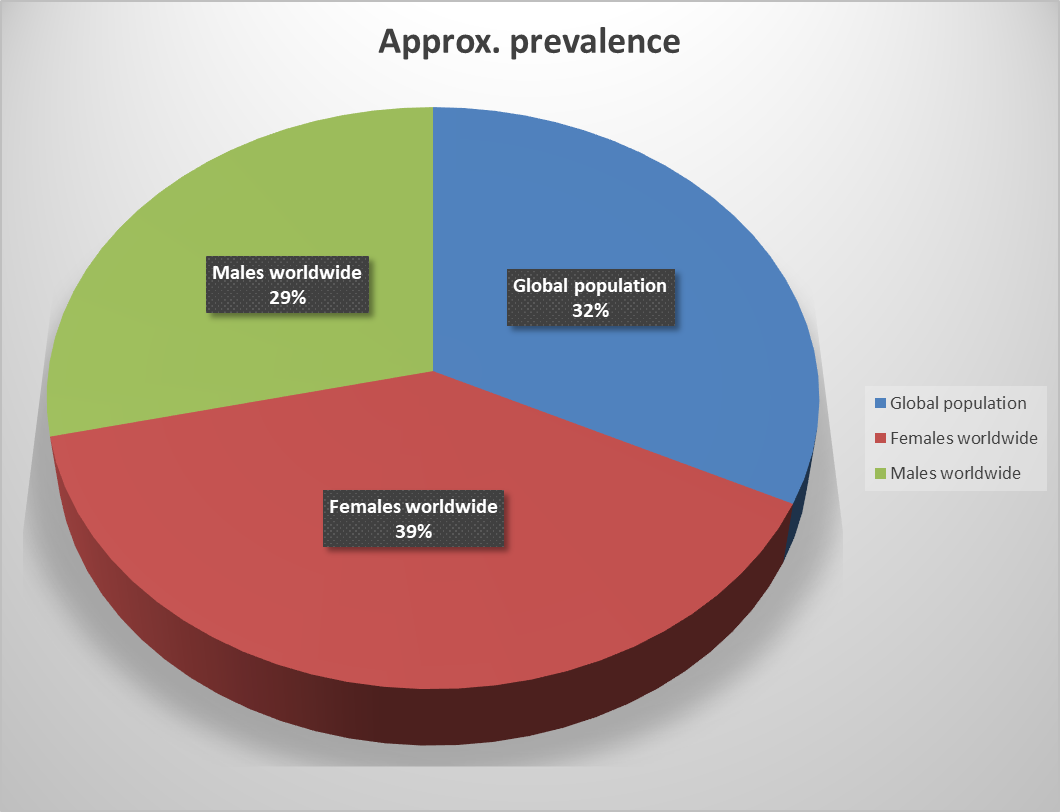
Pie chart to show estimated Number of People Affected Worldwide showing that females
To estimate the absolute number of people affected this table is what we are using, data is from pubmed,
This is giving us the approximate prevalence of gallstones disease worldwide.
To understand it better we will use piechart or any other form of expressive information chart. These figures are approximate global estimates; actual numbers vary by region, age group, and diagnostic methods.
The data presented in the tables highlight the significant global burden of gallstone disease. Worldwide, an estimated 6.1 % of the population, or roughly 488 million people, are affected. This underscores the importance of recognizing gallstones not only as a common gastrointestinal disorder but also as a potential contributor to severe complications such as acute cholecystitis, choledocholithiasis, and gallstone pancreatitis.
Why Regional Differences Exist in Prevalence-
These worldwide disparities can be attributed to many factors:
1. Lifestyle and Nutrition: Western diets that are heavy in calories and fat are associated with higher bile cholesterol saturation, which increases the risk of stone formation. Higher rates are a result of sedentary lifestyles and obesity, which are more prevalent in industrialized nations.
2. Sex and Age: As people age, gallstones grow increasingly prevalent, particularly beyond the age of 40.
Because estrogen stimulates the production of cholesterol into bile, women are more likely than males to suffer this condition.
3. Healthcare and Socioeconomic Aspects: more asymptomatic stones may be found in areas with easier access to imaging. Variations in risk factor distribution and genetic background also have an impact.
Risk Factors:
Gallstone risk factors can include:
Having a family history of gallstones, and Having been pregnant, possessing a gene variant that considerably raises the risk of gallstones, Taking oral contraceptives, Being sedentary, Undergoing high-dose estrogen therapy, Recently losing a significant amount of weight, Consuming a lot of dietary fat, being older than 60, and Being Native American, Having diabetes and using statins, which are medications that decrease cholesterol Gallstones are more common in women than in males.
Furthermore, males who purposefully dropped weight quickly and then put it back on may be more susceptible to gallstones in the future. Additionally, research has linked hormone replacement therapy for women during menopause to a higher risk of gallbladder problems. A study found that HRT administered by skin patches or gels poses a little risk than HRT taken orally.
Diagnosis:
Gallbladder stones
With a sensitivity of 97% and a specificity of 95%, transabdominal ultrasonography is the most popular and reliable technique for identifying gallbladder stones that are less than 5 mm. Additionally, ultrasonography may be used to measure gallbladder volume and motility (normal ejection fraction >60%) and is a highly helpful diagnostic technique for acute cholecystitis. Transabdominal ultrasonography, on the other hand, is less sensitive to microlithiasis (stone size 1–5 mm), which can lead to recurrent biliary colic and consequences like "acalculous" cholecystitis or recurrent pancreatitis. In 70–90% of instances, microlithiasis may be detected with greater sensitivity and specificity using endoscopic ultrasonography and/or microscopic analysis of bile.
Bile duct stones-
Since endoscopic retrograde cholangiography (ERC) provides treatment alternatives, it is the recommended diagnostic technique for patients with a strong suspicion of bile duct stones. If the bile duct is dilated (>7 mm) and bilirubin, γ-glutamyl transferase (GT), and/or alanine aminotransferase (ALT) are raised, or if gallbladder stones and biliary colic are present at the same time, the likelihood of bile duct stones is significant.
Notably, individuals with symptomatic bile duct stones in which acute (bile acid-mediated) hepatocellular damage predominates but γ-GT and alkaline phosphatase are not yet triggered may have increased ALT, including those without dilated ducts on transabdominal ultrasonography.
Patients with an intermediate risk of gallstones should have endoscopic ultrasonography and magnetic resonance cholangiography (MRC) due to the serious consequences that might arise with ERC. According to a recent meta-analysis of five RCTs with 301 patients, MRC and endoscopic ultrasonography show comparable
Bile duct stone detection sensitivity (93 vs. 85%) and specificity (96 vs. 93%). Although intraoperative cholangiography may be used to view the architecture and/or bile duct stones in patients undergoing cholecystectomy, current recommendations do not support its non-selective usage because less than 4% of individuals had unexplained stones. MRC and abdominal ultrasonography are the primary diagnostic methods for intrahepatic stones.
PREVENTION:
Although randomised controlled trials (RCTs) have not yet been conducted, lifestyle modifications, particularly cutting back on overall calorie consumption, may help reduce the production of cholesterol gallstones. Gallstone development can be effectively averted by UDCA (at least 500 mg per day) or early enteral feeding, respectively, in certain situations that are linked to an elevated risk of gallstones, such as fast weight loss (>1.5 kg/week) or whole parenteral nutrition. The latter situation may also benefit from the administration of motilin agonists such erythromycin or clarithromycin (500–600 mg) or cholecystokinin (50 ng/kg/day i.v.).
An exciting new concept in the prevention of gallstone formation is the stimulation of nuclear receptors that regulate metabolism and secretion of biliary lipids, as shown by the efficient prevention with synthetic agonists of the central bile salt sensor FXR in mouse models.
Dietary and/or lifestyle adjustments can lower the incidence of symptomatic gallstone disease or the rate of cholecystectomy. Recreational physical exercise is linked to a lower risk of cholecystectomy, while a sedentary lifestyle is linked to a greater risk. It has been suggested that regular use of coffee and nuts, together with modest amounts of alcohol, might lower the risk of gallstone disease symptoms. In order to lower the conversion rate from the asymptomatic to the symptomatic condition, it makes sense to encourage gallstone carriers who do not exhibit any symptoms to adhere to at least some of these guidelines.
If the patient is not complying with these methods of preventions there is a definitive management involving surgery.
MANAGEMENT:
-Asymptomatic Gallstones
• No medical intervention is necessary.
• Just observation
• Cholecystectomy as a preventative measure only in cases of high risk:The gallbladder made of porcelainGallbladder polyp more than 1 cmHemolytic anemia
• Big stones (more than 2-3 cm)
• Those in need of bariatric or transplant surgery
-Gallstones with symptoms (Biliary Colic)
• Analgesics, preferably NSAIDs
• Antiemetics
• Cholecystectomy via elective laparoscopy (final therapy)
- Acute Calculous Cholecystitis
• Admission to the hospital
• Nonprofit
IV fluidsIV antibiotics with a broad range of action
• Pain relief
• Cholecystectomy by laparoscopy as soon as possible (within 72 hours)
• No medical intervention is necessary
.• Just observation
• Cholecystectomy as a preventative measure only in cases of high risk:The gallbladder made of porcelainGallbladder polyp more than 1 cmHemolytic anemia
• Big stones (more than 2-3 cm)
• Those in need of bariatric or transplant surgery
Gallstones with symptoms (Biliary Colic)
• Analgesics, preferably NSAIDs
• Antiemetics
CONCLUSION
A frequent hepatobiliary condition called gallstone disease (cholelithiasis) is brought on by abnormalities in the composition of bile and gallbladder motility. When bile becomes supersaturated—usually with cholesterol—along with poor gallbladder emptying and crystal nucleation, gallstones develop. The main reasons include biliary stasis, illness, reduced bile acids, and increased cholesterol secretion (as shown in obesity, pregnancy, and estrogen medication). Risk factors are traditionally summed up as the "four F's": forty, female, fat, and fertile. There are three types of gallstones: pigment stones (black stones linked to cirrhosis and hemolysis, and brown stones linked to biliary infection), cholesterol stones (the most common type, usually yellow and radiolucent), and mixed stones, which contain different amounts of calcium salts, bilirubin, and cholesterol.
In terms of clinical presentation, gallstone disease can be asymptomatic or manifest as biliary colic, which is defined by discomfort in the right upper quadrant that radiates to the right shoulder or scapula, frequently following fatty meals. Peptic ulcer illness, acute pancreatitis, hepatitis, appendicitis, right lower lobe pneumonia, renal colic, and myocardial ischemia are among the differential diagnoses that require thorough clinical evaluation and imaging, particularly ultrasound. Acute calculous cholecystitis is caused by a stone blocking the cystic duct, which results in fever, leukocytosis, a positive Murphy's sign, and persistent discomfort in the right upper quadrant that lasts longer than six hours. Gallstone pancreatitis, gallstone ileus (intestinal blockage brought on by a migrated stone), ascending cholangitis, obstructive jaundice, and choledocholithiasis (stones in the common bile duct) are among the major consequences that gallstone disease can cause if left untreated.
Although laparoscopic cholecystectomy is still the gold standard surgical procedure, care is contingent on symptoms and complications. Open surgery may be necessary in complex situations, and endoscopic retrograde cholangiopancreatography (ERCP) is utilized in certain circumstances to remove bile duct stones. Morbidity is greatly decreased and potentially fatal complications are avoided with early diagnosis and prompt surgical surgery.
REFERENCE
o Bailey & Love’s Short Practice of Surgery– Chapter on gallbladder and biliary tract disease.
o Sabiston Textbook of Surgery– Section: Liver, Biliary Tract, and Pancreas.
o Schwartz’s Principles of Surgery– Chapter on biliary tract disorders.
o Harrison’s Principles of Internal Medicine– Chapter on diseases of the gallbladder and bile ducts.
o World Society of Emergency Surgery Guidelines – WSES Guidelines for Acute Calculous Cholecystitis.
o Tokyo Guidelines (TG18/TG23)– Management of acute cholangitis and cholecystitis.
o American College of Gastroenterology Guidelines– Management of gallstones and choledocholithiasis.
o Society of American Gastrointestinal and Endoscopic Surgeons Guidelines– Clinical application of laparoscopic biliary surgery.
o National Institute for Health and Care Excellence (NICE) clinical guideline on gallstone disease https://www.ncbi.nlm.nih.gov/books/NBK327527/ — Gallstone disease diagnosis and management from NICE CG188 (covers cholelithiasis, cholecystitis, choledocholithiasis)
o NICE official recommendation page for gallstone disease https://www.nice.org.uk/guidance/cg188/chapter/1-recommendations — Recommendations on investigations and timing of surgery in gallstone disease.
o AAFP overview on management of gallstones and complications https://www.aafp.org/pubs/afp/issues/2000/0315/p1673.html — Discusses surgical timing, ERCP, and cholecystectomy strategies
o BMJ summary of NICE guidance on gallstone management https://www.bmj.com/content/349/bmj.g6241 — Summary article of evidence-based management from NICE