
Pediatric Infective Endocarditis: Evolving Epidemiology, Diagnostic Challenges, and Contemporary Management Strategies
1. Endysh Kyzy Gulsara
2. Kavita Choudhary
Aniket Mahajan
Advait Makode
Arslan Latif
Shehroz Tariq
(1. Teacher, International Medical Faculty, Osh State University, Kyrgyzstan)
(2. Students, International Medical Faculty, Osh State University, Kyrgyzstan)
Abstract
Infective endocarditis (IE) in children, once considered a rare occurrence, has emerged as a significant cause of morbidity and mortality in the pediatric population. This comprehensive review examines the evolving landscape of pediatric IE, focusing on epidemiological shifts, diagnostic modalities, treatment strategies, and outcomes. The rising number of IE cases occurs together with enhanced survival rates among children who suffer from congenital heart disease (CHD) and the expanded use of intracardiac prostheses and the in- creasing number of children who need central venous catheters. Recent multicenter studies show that Gram-positive bacteria especially Staphylococcus aureus continue to dominate as pathogens however there has been a concerning rise of non-HACEK Gram-negative bacteria and multidrug-resistant organisms. The process of diagnosing patients remains difficult because of the existing problems with culture-negative cases and the need to differentiate infective endocarditis (IE) from other febrile conditions that affect vulnerable patients. The management process needs multiple specialists to examine two key aspects which include deciding when to start medical treatments and performing surgeries while assessing how these choices will influence results that extend into the future. This review synthesizes current evidence from major pediatric cardiac centers and provides practical recommendations for clinicians caring for children with suspected or confirmed IE.
Keywords: infective endocarditis, congenital heart disease, pediatric cardiology, Staphylococcus aureus, vegetation, multidrug resistance, cardiac surgery
INTRODUCTION
The medical condition infective endocarditis occurs when bacteria infect the endocardial surface of the heart which leads to the development of vegetations that contain microorganisms and platelets and fibrin thrombi. The vegetations develop the ability to destroy endocardial tissue and cause valve failure and create blood clots that travel through the body and harm vital organs. The disease IE which was believed to affect only adults who had rheumatic heart disease as their main precursor has experienced major changes in its epidemiological patterns among children during the past 50 years (Dixon and Christov 257).
The annual incidence of IE in children estimates between 0.43 and 0.69 cases per 100000 population which represents a lower rate compared to the 3 to 7 cases per 100000 that occurs in adults (Essa and Said 30). Multiple factors which all connect with each other because this increase in incidence. The outstanding progress in survival rates for children who have congenital heart disease represents the main factor that contributes to this situation because these children now receive complex palliative and corrective treatment which medical professionals could not perform before the previous generation. The rising number of CHD survivors who have implanted prosthetic devices and surgical shunts and transcatheter-implanted devices creates a new group of individuals who face increased risk (Marín-Cruz et al. 3906). The development of pediatric critical care medicine has produced new populations that experience increased susceptibility to infective endocarditis. The risk of infective endocarditis increases for three groups of people which include premature infants who need central venous access for more than 30 days and immunocompromised patients who receive intensive chemotherapy or stem cell transplants and patients who depend on indwelling catheters for their chronic illnesses (Abdel-Haq et al. 1742). The introduction of these two groups of people results in complete changes to the microbiological patterns which determine how children with infective endocarditis will display their symptoms and what results they will achieve.
The study of pediatric infective endocarditis shows less research activity than studies that focus on adult populations even though there have been major changes to its epidemiological patterns. The clinical practice guidelines which medical professionals use today mostly come from studies on adult patients because there is insufficient evidence from studies that focus on pediatric patients. This review presents existing knowledge about pediatric infectious endo- carditis through its epidemiological patterns and diagnostic methods and treatment approaches which include recent multicenter research about this particular dangerous disease.
METHODS
The narrative review collected evidence from scientific studies which appeared in peer-reviewed journals between 2017 and 2025. The research team performed a systematic search through PubMed and MEDLINE and Scopus databases which used various combinations of these search terms “pediatric infective endocarditis” “congenital heart disease” “Staphylococcus aureus” “multidrug resistance” “vegetation” and “cardiac surgery.” The researchers included original research articles and multicenter studies and retrospective cohort analyses and clinical guidelines which studied children who had definite or possible IE. The researchers selected studies from the last five years as their primary focus but they also included essential studies and guideline documents from the years 2015 to 2017 to provide historical context and enable comparative analysis. The research team conducted manual searches through the reference lists of retrieved articles to find additional publications which might be relevant to their study.
RESULTS
Epidemiology and Risk Factors
The epidemiological profile of pediatric IE has undergone substantial evolution over the past two decades. Current multicenter research studies provide researchers with essential information about present-day research patterns. The 19-year research study at Children’s Hospital of Michigan showed that the hospital experienced a twofold increase of IE cases between 2012 and 2020 when compared to the period between 2002 and 2011. The Spanish reference center study of 32 IE episodes between 2012-2021 showed a pattern that European centers confirmed. The study found that 87.5% of patients who had CHD received their diagnosis at a median age of 9.1 months (Marín-Cruz et al. 3907).
CHD serves as the primary risk factor because more children with complex medical conditions survive and doctors increasingly utilize prosthetic materials to treat their surgical needs. Borrelli and his team found that prior cardiac surgery or percutaneous intervention together with prosthetic materials and serious valvular heart diseases represented the primary risk factors for endocarditis in their research which covered 41 CHD patients across multiple medical centers throughout the United States (Borrelli et al. 2). The presence of prosthetic material causes fundamental changes to both the microbiological aspects and the clinical development of infective endocarditis which uses foreign body surfaces as sites for bacteria to attach and create biofilm that combat conventional antimicrobial treatment.
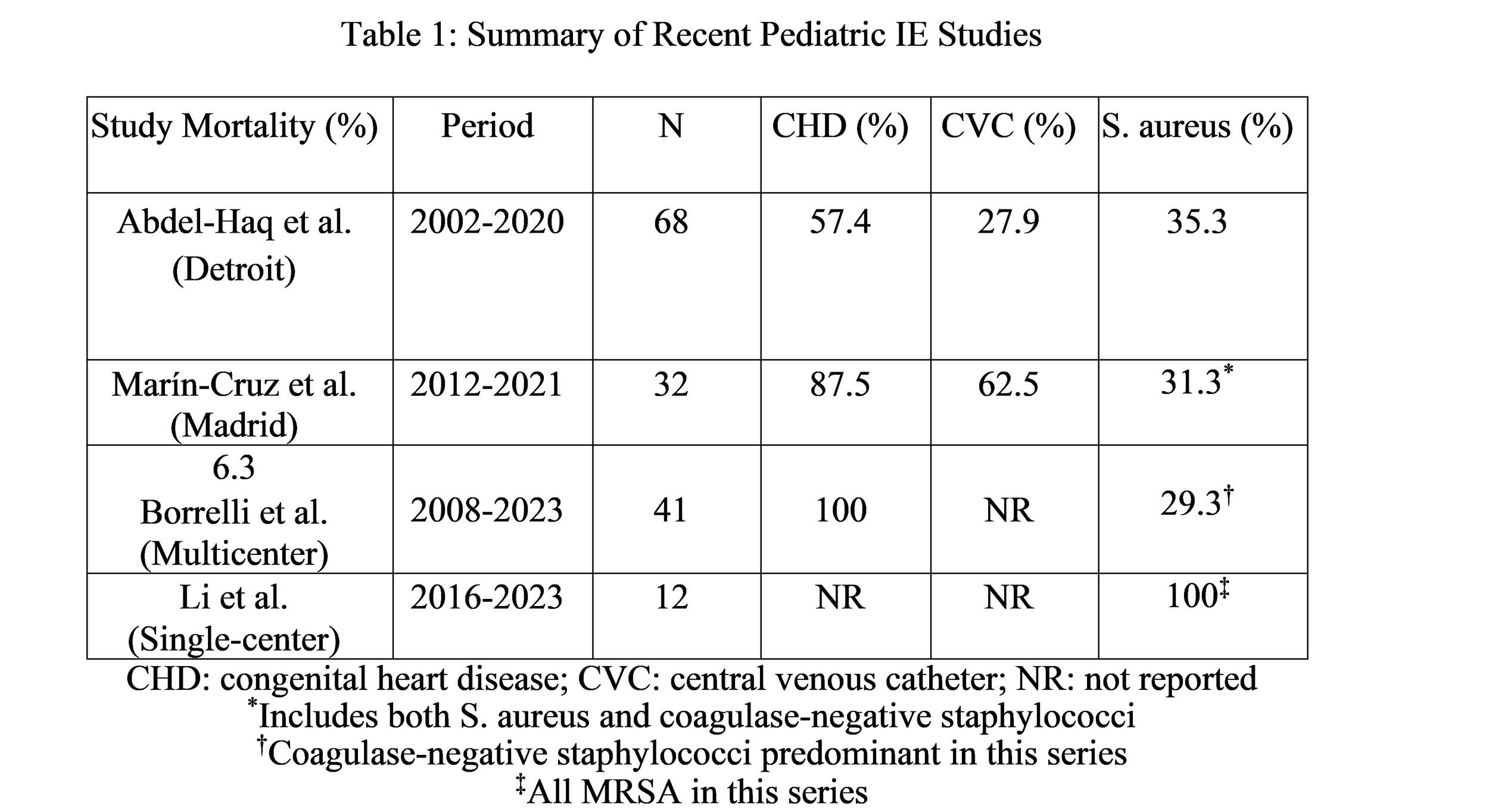
The use of central venous catheters creates the second major danger which affects most infants and young children. The Spanish study found that children with indwelling CVCs experienced 62.5% of all IE episodes while preterm infants and immunocompromised children together with patients who had chronic medical conditions developed CVC-related IE more often than patients who had isolated CHD (Marín-Cruz et al. 3908). CVC-related bacteremia typically involves staphylococci and Gram-negative organisms which show different resistance patterns thus establishing important requirements for choosing antibiotics through empirical methods.
Microbiology: Shifting Patterns and Emerging Threats
The majority of pediatric cases of infective endocarditis involves Staphylococcus aureus as the primary pathogen because it appears in 35.3% of Michigan cases and European studies show its high occurrence (Abdel-Haq et al. 1744; Marín-Cruz et al. 3908). The virulence of S. aureus stems from its collection of adhesion proteins together with tissue-damaging enzymes and its ability to create infections at distant sites. The bacterium methicillin-resistant S. aureus (MRSA) presents.
The present study investigates Streptococci which used to be the primary pathogens causing infective endocarditis during the period before antibiotics became available but now their prevalence has decreased to 22 percent of cases while viridians group streptococci continue to act as significant pathogens for children who suffer from valvular defects according to Abdel-Haq et al. 1744. The healthcare system has experienced a rise in infections which has resulted in decreased cases of streptococcal infective endocarditis. The emergence of Gram-negative organisms and multidrug-resistant bacteria as pathogens in infective endocarditis represents the most alarming development in this field. The Spanish series documented an unexpectedly high proportion of non-HACEK Gram-negative bacteria which accounted for 27.8 percent of all microbiological isolates according to Marín-Cruz et al. 3909. The study presents new evidence which contradicts established ideas about the microbiological causes of infective endocarditis while it establishes critical requirements that need to be fulfilled during the selection process of antibiotics used for treatment. The HACEK group (Hemophilus species, Aggregatibacter species, Cardio bacterium hominis, Eike Nella corrodes, and Kinsella species), traditionally emphasized in IE teaching, accounted for only 2.8% of isolates, suggesting that contemporary pediatric IE epidemiology diverges substantially from classic descriptions. The relationship between multidrug-resistant bacterial colonization and subsequent infectious endocarditis development represents a pressing concern for healthcare providers. The Spanish series found that 30 percent of colonized patients developed infective endocarditis which resulted from the same multidrug-resistant bacterial strain according to the statistical analysis which con- firmed this relationship (p = 0.007) (Marín-Cruz et al. 3910). The research demonstrates that high-risk groups require surveillance cultures for monitoring purposes while empirical antibiotic treatment must include coverage for all bacteria present in colonized patients.
Fungal IE is an uncommon disease which affects 11.1% of isolates from the Spanish series but produces severe health risks for patients who need extreme medical support and who suffer from prolonged central venous catheter use or who are extremely premature or who have severe immunodeficiency (Marín-Cruz et al. 3908). The most common species found in this study are Candida species whereas Aspergillus and other molds exist in patients who have the most extreme immunosuppression.
Clinical Presentation and Diagnostic Challenges
The clinical presentation of pediatric IE shows major differences which depend on a patient’s age and medical history and the microorganism that causes the infective endocarditis. Fever represents the most consistent finding, present in 84.4% of patients in the Spanish series (Marín- Cruz et al. 3907). Physicians must maintain a strong suspicion about infective endocarditis when they treat children who belong to high-risk groups because fever shows no specific patterns in this age group.
The Spanish patient group showed shock symptoms at their first examination, with 50% of the patients displaying this condition because current pathogens present high virulence levels and doctors take too long to identify childhood illnesses (Marín-Cruz et al. 3907). The study found 43.8% of patients developed vascular complications which included septic emboli, with lung embolism being the most common type found in patients with right-sided infections. Surgical decisions about timing rely on cerebral embolization, which occurs less frequently but leads to major health problems.
The modified Duke criteria stand as the established diagnostic method for pediatric infectious endocarditis because it combines three types of evidence which are microbiological results and echocardiographic results and clinical assessment (Essa and Said 32). The criteria establish acceptable sensitivity which keeps their identification capability intact because they enable correct identification of cases that the criteria define for children. The Spanish series showed that 87.5% of episodes reached the criteria for probable IE which confirms that these criteria function effectively in present-day clinical practice (Marín-Cruz et al. 3907).
Echocardiography functions as an essential diagnostic method which uses transthoracic echocardiography (TTE) as its primary testing method for pediatric patients. TTE generally provides excellent image quality in pediatric patients because of their acoustic window advantages yet transesophageal echocardiography (TEE) helps detect prosthetic valve issues and annular abscesses and vegetations in one-third of cases that involve older children or those with damaged acoustic windows (Essa and Said 33). Three-dimensional echocardiography provides extra anatomical information which assists in creating surgical operation strategies.
Vegetation size serves as an essential factor that determines patient outcomes. Borrelli and his team found that embolic events show a strong connection with vegetation size because larger vegetations create a greater risk of experiencing embolic events (Borrelli et al. 3). This discovery matches findings from adult research which shows that doctors should consider performing early surgical procedures on patients who have large vegetations and experienced embolic events before. The diagnostic process becomes difficult for medical professionals when they encounter culture-negative endocarditis because it exists in 40 percent of documented cases according to research conducted by Essa and Said. The three main causes of this condition include previous antibiotic treatment and the presence of difficult-to-cultivate microorganisms and non-bacterial infectious agents. The HACEK group together with Coxiella burnetii (Q fever) and Bartonella species and fungi require both special culture methods and serological testing for their identification. The identification of pathogens in culture-negative cases requires extended incubation periods together with molecular diagnostic techniques that use 16S rRNA gene sequencing.
Management Strategies
Antimicrobial Therapy
Medical professionals use appropriate antimicrobial treatment as the fundamental method to treat infective endocarditis (IE). The empirical treatment plan requires medical professionals to identify the most probable pathogens through clinical assessment and examination of patient risk factors and regional resistance patterns. The therapy for stable patients who have negative blood cultures can be postponed until culture results arrive while unstable patients require immediate treatment.
The treatment of community-acquired infective endocarditis in children with congenital heart disease requires a combination of ampicillin and an aminoglycoside because these drugs will effectively treat both streptococci and enterococci and the treatment need to include anti-staphylococcal coverage through nacillin or vancomycin depending on the actual MRSA risk in the specific medical situation. Healthcare-associated IE needs to use vancomycin for MRSA along with additional Gram-negative organism coverage that matches local susceptibility patterns be- cause patients with CVCs have higher risk of the disease (Essa and Said 34).
Clinicians determine definitive therapy based on the pathogens that they identify and their antimicrobial resistance patterns. The Chinese series showed that linezolid and vancomycin and the combination of cephalosporin with enzyme inhibitors dominated clinical practice because doctors needed to treat patients who showed high rates of MRSA and required broad-spectrum medication for complex cases (Li et al. 1591). The study found that only 25 percent of cases involved therapeutic drug monitoring for vancomycin which demonstrates a major opportunity to improve quality because vancomycin pharmacokinetics differ significantly between children and subtherapeutic levels lead to treatment failure while excessive levels result in nephrotoxicity. The standard treatment duration for most medical conditions lasts between 4 and 6 weeks however some cases of uncomplicated right-sided infective endocarditis which involve highly susceptible organisms can be treated with shorter drug treatment periods. Patients with prosthetic valve infective endocarditis and fungal infective endocarditis and those with infections caused by highly resistant organisms need to undergo lengthy treatment periods that extend from 6 to more than 8 weeks. Parenteral antimicrobial therapy can be completed by outpatient treatment in patients who meet specific criteria because they have stable medical conditions and sufficient social support and will receive regular medical follow-up.
Surgical Intervention
Surgical management plays an essential role in approximately 20-30% of pediatric IE cases with Michigan patients undergoing valve replacement or valvuloplasty at a rate of 22.1% (Abdel-Haq et al. 1745). The medical field recognizes multiple indications for surgery which include heart failure that does not respond to treatment and ongoing sepsis that persists despite receiving appropriate antimicrobial treatment and multiple embolic events that continue to occur even after proper treatment and large vegetations that exceed 10 mm in size and pose an embolic threat and perivalvular extension with abscess development and dysfunctional prosthetic valves and infections that result from highly resistant organisms which medical treatment cannot eliminate. The surgical procedure needs to be planned at a specific moment which requires assessment of different risks that can affect patient outcomes. The process of waiting to perform surgery on patients who need it leads to their hemodynamic status becoming worse and their heart muscle experiencing permanent harm and their risk of experiencing more embolic incidents increasing. The procedure requires more technical expertise because of active infections and that situation creates a higher possibility to experience prosthetic reinfection. The medical standard for operating on patients who have stable conditions requires doctors to eliminate all bloodstream infections before beginning their surgical procedures. Most patients in the Michigan series required surgical intervention within seven days after their initial diagnosis while half of the patients needed surgery within three days because of myocardial dysfunction or staphylococcal infection (Essa and Said 35).
The surgical procedure requires complete removal of all infected tissues together with col- lection of abscess materials and construction of new valves or restoration of existing valves. The medical field considers pediatric patients to require valve repair as their preferred option whenever it proves feasible because this method maintains their original heart structure while allowing their body to develop and it eliminates the need for blood-thinning medication and possible problems that come with artificial heart valves. Successful repair success depends on two factors which include infection that affects only the leaflet tissue and does not cause major damages to the structure.
Special Populations: Device-Related Endocarditis
The growing application of transcatheter-implanted devices for treating congenital heart dis- ease has established new patient groups which now face the danger of developing device-related endocarditis. The Melody valve (Medtronic) functions as a bovine jugular vein valve which doctors implant through the skin into the pulmonary position yet the device has shown high incidence rates of infective endocarditis which range between 3 and 14 percent. The exact causes behind this tendency remain unidentified although they may connect to the natural characteristics of bovine jugular vein tissue and blood flow conditions and the partial development of new endothelial tissue after the device went into use.
The Melody valve implant procedure results in about 84.9% of patients remaining free from infective endocarditis after 5 years which equals the success rate of surgically implanted Contegra bovine jugular vein conduits yet surpasses other surgical conduit methods (Essa and Said 36). Melody valve endocarditis presents with uncommon clinical features in which patients display fewer echocardiographic findings than anticipated and show different pathogens which cause their condition when compared to native valve infective endocarditis. The condition of acute right ventricular outflow tract obstruction stands as an uncommon yet dangerous medical emergency which needs immediate medical treatment.
The same issues which affect transcatheter devices also apply to septal occludes and percutaneous pulmonary valves which other companies produce. The process of treating device related infective endocarditis typically necessitates device removal to achieve treatment success yet doctors may use long-term antibiotics to manage patients who cannot undergo surgery. The prevention methods require doctors to use strict aseptic procedures during the installation process and to provide proper antibiotic treatment when patients undergo future medical procedures which have a chance of causing bacteremia.
Multidisciplinary Approach
Modern IE management demands a multidisciplinary team that combines the knowledge from pediatric cardiology and infectious diseases and cardiac surgery and intensive care to solve the problem. The “endocarditis team” concept, endorsed by both American Heart Association and European Society of Cardiology guidelines, facilitates timely decision-making, optimizes medical- surgical coordination, and improves outcomes (Dixon and Christov 258). The team examines all IE cases through their review process which enables them to make systematic decisions about when to perform surgery and what type of treatment to use and how to track patient progress after treatment.
Outcomes and Prognosis
Pediatric IE remains a serious health threat because new methods for diagnosing and treating the condition fail to reduce its high rate of life-threatening complications and deaths. In-hospital mortality in contemporary series ranges from 6-10% with the Michigan series documenting 10.3% mortality (Abdel-Haq et al. 1745) and the Spanish series reporting 6.3% (Marín-Cruz et al. 3910). The data show an alarming situation but the current mortality rates show an improvement compared to historical mortality rates which exceeded 25% for native valve endocarditis.
The risk of death from a disease depends on two main factors, which include the individual characteristics of the patient and the specific pathogen. The outlook for S aureus IE presents a serious danger because MRSA infection led to the death of one patient from Michigan de- spite the medical staff’s best efforts to treat the patient (Abdel-Haq et al. 1745). The CHD patient group and the CVC user group both experience higher mortality risk, in addition to immunocompromised people and patients with fungal IE.
The study found that 30 percent of pediatric cases of infective endocarditis developed com- plications which most often took the form of septic embolism according to Abdel-Haq and his colleagues on page 1745. The process of embolic events develops through two primary pathways which include pulmonary circulation and systemic arterial beds and cerebral circulation. Cerebral embolization leads to high levels of morbidity which can result in permanent neurological sequelae. The medical condition produces three main complications which include heart failure that results from valvular destruction and perivalvular abscess with conduction abnormalities and metastatic infection to distant sites of the body.
The successful treatment of infective endocarditis establishes long-term results which de- pend on three main factors that include valvular damage assessment and remaining prosthetic materials and existing heart conditions. The patients need to undergo extended monitoring sessions which help to assess their valvular performance and find any upcoming issues and enforce all protective protocols. Current guidelines should be used to review and reinstate antibiotic prophylaxis for dental work and invasive treatments.
DISCUSSION
The pediatric infective endocarditis patterns which show continuous changes create two main effects on doctors who work with children having higher infection threats. The rising incidence of IE, documented across multiple centers and geographic regions, reflects the success of modern pediatric cardiology in extending survival of children with complex CHD while simultaneously creating new populations vulnerable to infection. The epidemiological shifts require staff members to study them because they need to maintain their ability to identify diseases and choose their treatment methods and verify long-term success.
The field of microbiology now faces different research needs because of its new discoveries about infectious diseases and their medical treatments. The present-day pediatric infectious endocarditis microbiological profile shows significant differences from the traditional medical descriptions of the disease. The medical establishment must update its diagnostic methods and treatment procedures for infectious endocarditis because non-HACEK Gram-negative bacteria and multidrug-resistant pathogens have become important infectious endocarditis pathogens which continue to exist. Healthcare professionals need to understand that infectious endocarditis can develop from uncommon pathogens which particularly affect patients who enter medical facilities and who use multiple medical devices. The relationship between MDRB colonization and its subsequent development into IE infection with identical strains creates critical effects for both infection control measures and initial treatment decisions according to (Marín-Cruz et al. 3910). The process of surveillance cultures which targets high-risk patients enables the discovery of specific organisms that will likely lead to invasive infections. The approach allows medical staff to optimize their antibiotic treatment plans when doctors suspect an infection of infectious endocarditis. Intensive care units particularly benefit from this approach because they frequently see multidrug-resistant bacterial colonization and doctors face serious consequences when they choose improper initial treatment methods.
The predominance of MRSA in some series (Li et al. 1590) highlights geographic variation in resistance patterns and the importance of local epidemiology in guiding empiric therapy. Medical facilities that experience high MRSA rates must use their initial treatment methods to guarantee patients receive proper treatment which requires the use of vancomycin or linezolid drugs. The study found that Chinese hospitals used therapeutic drug monitoring for vancomycin at a low rate which creates a chance to enhance healthcare standards because advanced monitoring will help achieve better patient results and decrease adverse effects.
Diagnostic Challenges and Opportunities
The diagnosis of pediatric IE remains difficult for medical professionals because patients with this condition present no visible symptoms that doctors usually rely on for assessment. The modified Duke criteria create a valuable framework for diagnosing patients but need changes to suit the requirements of pediatric patients. The study results show that half of Spanish patients with shock (50% in the Spanish series) present at hospitals with advanced medical conditions (Marín-Cruz et al. 3907). The medical community uses three main strategies to detect diseases earlier which include maintaining high suspicion in at-risk populations and using echocardiography for all febrile patients with risk factors and conducting microbiological tests without delay.
Advanced imaging technologies enable better accuracy in diagnostic procedures which helps medical professionals decide on treatment options. Medical professionals use echocardiography as the main imaging technique but they also use cross-sectional imaging methods (CT and MRI) to find complications outside the heart which helps them detect embolic events that determine when surgery should occur (Essa and Said 33). Medical professionals use FDG-PET/CT as a useful diagnostic tool in specific adult patient groups who require detection of prosthetic valve infection and hidden metastatic infection; however, its application in pediatric patients remains underexplored.
Controversies and Unresolved Questions
The management of pediatric infectious endocarditis still lacks resolution for multiple critical questions which need answers. The best time when surgical treatment should start for children who have large vegetations needs further research because they do not meet requirements for other surgical procedures. The research shows that adults should undergo surgery right away when they have large vegetations which cause them to suffer from embolic events but scientists do not know whether this applies to children (Borrelli et al. 3). Pediatric-specific risk stratification tools which include vegetation size and causative organism and patient characteristics will help surgeons make better surgical decisions. The medical community does not yet understand how oral antibiotics work for treating pediatric infectious endocarditis. Adults who receive intravenous therapy can switch to partial oral treatment after their first intravenous session. The medical community needs to investigate the effectiveness of oral step-down therapy for pediatric patients who need long-term intravenous access because intravenous treatment causes problems for children and raises their need for hospital time. Medical professionals need to know how long patients with prosthetic valve infective endo- carditis need treatment especially when dealing with transcatheter valves. The existing guidelines use adult surgical valve research to create their guidelines which need to change because percutaneous valves behave differently than adult surgical valves and they interact with body tissues in unique ways. The collection of long-term registry data will provide crucial information which healthcare providers need to develop management guidelines for these devices which have become more frequently used.
Future Directions
The solution requires multiple domains to work together to solve the challenges that exist in treating pediatric IE. Multicenter prospective registries are essential because they help drive research by providing enough case data for researchers to perform subgroup analyses and discover factors that lead to positive outcomes. The registries must collect extensive data about patient attributes together with microbiological results and treatment methods and their long-term results to create prediction models and treatment pathways specifically for pediatric patients.
Research priorities include investigation of host-pathogen interactions in the setting of prosthetic materials, development of biofilm-resistant materials for intracardiac devices, and evaluation of novel antimicrobial and antibiofilm strategies. The high incidence of IE in bovine jugular vein conduits (Essa and Said 36) indicates that material properties determine infection risk, and research into these connections will help develop infection-proof prosthetic devices.
The development of prevention strategies requires additional focus. The 2007 AHA guide- lines decreased antibiotic prophylaxis recommendations, which created major restrictions, but multiple studies show increasing rates of IE that have occurred since that time (Abdel-Haq et al. 1743) which raises questions about the effect of these alterations. The actual increase results from several elements which include growing numbers of at-risk individuals, and researchers must explore the role of decreased prophylaxis in driving this pattern according to their judgment.
CONCLUSION
The rare occurrence of infective endocarditis in children has become an increasing problem which results in health complications and deaths among vulnerable children. The increasing rate of congenital heart disease cases occurs because more children with this condition survive and doctors now use intracardiac prostheses and more children develop complications from central venous catheters. Proper understanding of these epidemiological changes helps medical professionals maintain their needs for diagnostic testing while they carry out their patient treatment process.
The current microbial landscape of pediatric infective endocarditis shows Staphylococcus aureus as the most common pathogen while non-HACEK Gram-negative bacteria have appeared and multidrug-resistant organisms have become increasingly important. The observed microbiological patterns create critical effects which influence choice of initial antibiotics and demonstrate the necessity for continuous monitoring of regional resistance trends. The link between multiple drug-resistant bacteria colonization and subsequent endocarditis caused by the identical strain demonstrates the importance of high-risk patient surveillance cultures.
The diagnostic process needs medical experts to maintain strong clinical suspicion while using echocardiography together with microbiological testing. The modified Duke criteria function as an effective diagnostic tool although they show limitations when applied to specific pediatric patient groups. The diagnosis of culture-negative endocarditis presents difficulties which need advanced testing methods that include molecular diagnostic techniques. Management requires medical professionals to work together who have specialized knowledge in pediatric cardiology and infectious diseases and cardiac surgery and intensive care. Doctors need to use targeted pathogen treatments whenever feasible because they must monitor patient medication dosages and treatment periods. Surgical procedures become necessary for patients who experience heart failure combined with persistent sepsis and recurrent embolization and large vegetations and perivalvular extension and prosthetic infection. Medical professionals should choose valve repair as the primary treatment method for children.
Pediatric patients with infective endocarditis continue to experience severe health complications and high death rates despite improvements in medical treatment. The current series shows an in-hospital mortality rate between 6 and 10 percent which represents better outcomes than past studies but still remains excessively high. About 30 percent of patients experience complications which make septic embolism the most common and serious medical problem.
The future development process needs research from multiple centers to create pediatric- specific guidelines and examine prosthetic materials that resist infection and reinforce existing prevention methods. The ultimate goal remains reducing the burden of this serious infection through improved prevention, earlier diagnosis, and more effective treatment. The parents and children who experience infective endocarditis need medical advances to reach them as soon as possible.
References
[1] Abdel-Haq, Nahed, et al. “Infective Endocarditis at a Referral Children’s Hospital During 19-Year Period: Trends and Outcomes.” Pediatric Cardiology, vol. 45, no. 8, 2024, pp. 1741- 1749.
[2] Borrelli, Nunzia, et al. “Infective Endocarditis in Pediatric Patients with Congenital Heart Disease: Results from a National Multicenter Study.” Pediatric Cardiology, 2025. Epub ahead of print.
[3] Dixon, Garth, and Georgia Christov. “Infective Endocarditis in Children: An Update.” Cur- rent Opinion in Infectious Diseases, vol. 30, no. 3, 2017, pp. 257-267.
[4] Essa, Yasin, and Sameh M. Said. “Diagnostic Work-up and Current Management Strategies for Infective Endocarditis in the Pediatric Population.” Indian Journal of Thoracic and Cardiovascular Surgery, vol. 40, no. Suppl 1, 2024, pp. 29-39.
[5] Li, Sanni, et al. “Drug Treatment Analysis of Infective Endocarditis in Children—A Retro- spective, Single-Centre Study.” Cardiology in the Young, vol. 35, no. 8, 2025, pp. 1589-1594.
[6] Marín-Cruz, Inés, et al. “Infective Endocarditis in Pediatric Patients: A Decade of Insights from a Leading Spanish Heart Surgery Reference Center.” European Journal of Pediatrics, vol. 183, no. 9, 2024, pp. 3905-3913.