
Immunodeficiency in Children: A Comprehensive Review
1. Endysh Kyzy Gulsara
2. Karan Karve
Kaveri Batwal
Anisha Chougale
Abhijeet Gaike
Krushna Jagtap
(1. Teacher, International Medical Faculty, Osh State University, Kyrgyzstan)
(2. Students, International Medical Faculty, Osh State University, Kyrgyzstan)
Abstract
The introduction of T-cell receptor excision circle (TREC) analysis for severe combined immunodeficiency screening in newborns has brought about significant improvements in early identification methods together with improvements in genetic testing methods and gene therapy approaches and hematopoietic stem cell transplantation which have developed into new treatment approaches. The article presents evidence-based research which establishes a systematic process for doctors to detect and assess and treat children who show signs of immunodeficiency while highlighting how early identification of this condition safeguards against illness and death.
Keywords: Primary immunodeficiency, inborn errors of immunity, severe combined immunodeficiency, pediatric immunology, newborn screening, immunoglobulin replacement, hematopoietic stem cell transplantation.
Introduction
The immune system functions as the body’s main protection system which defends against numerous microbial pathogens through its advanced defense system which includes physical barriers and innate cellular components and adaptive immunological memory. The system needs to establish its immunological competence because children face new environmental antigen exposures which require them to protect themselves. The body experiences an immunodeficiency state when its complex defense system breaks down because this leads to increased infection vulnerability.
The scientific understanding of immunodeficiency has progressed through many changes during the last 30 years. The medical community now considers what were once uncommon and obscure disorders to be important factors which cause pediatric patients to experience both illness and death across the globe. The International Union of Immunological Societies (IUIS) now classifies these disorders as “inborn errors of immunity” (IEI), acknowledging that they encompass not only infection susceptibility but also autoimmune manifestations, autoinflammatory syndromes, allergy, and malignancy. The new viewpoint shows that immune system disorders create more health problems than only stopping the body from fighting infections.
The present research has established new epidemiological benchmarks for primary immunodeficiency disorders (PIDD) because current studies present fresh evidence. The established rare disease status which affects 1 in 10,000 to 1 in 50,000 people has been reevaluated according to current research that shows approximately 1 in 1,200 live births face the condition. The current situation shows better diagnostic methods and increased disease recognition plus inclusion of less severe symptoms which together explain the present situation. The world experiences a higher prevalence of secondary immunodeficiency diseases which occur primarily through HIV infection and immunosuppressive drug use and malnutrition and these conditions need analysis during differential diagnosis assessment. The medical field needs to recognize the vital importance of detecting health issues at their earliest stage. Pediatric immunodeficiency results show that diagnostic delay represents the primary treatable element which determines patient results. The medical condition becomes worse for patients when health professionals diagnose them too late because prenatal infections keep accumulating and cause permanent damage to their bodies which includes bronchiectasis and hearing loss and growth failure. The medical field needs to detect health issues early because this practice allows doctors to provide critical treatments that include immunoglobulin replacement and antimicrobial preventive measures and stem cell transplantation and gene therapy.
The review presents evidence-based research about immunodeficiency states which affect children by describing classification systems and clinical symptoms and diagnostic procedures and modern treatment methods. The article uses present scientific research and clinical guidelines as its base to help medical professionals learn how to identify affected children and manage their complicated treatment path.
Methods
The researchers evaluated pediatric immunodeficiency states through a complete examination of peer- reviewed literature and recognized clinical standards. The researchers used a narrative synthesis method to combine results from multiple sources which included original research articles and systematic re- views and clinical practice guidelines and textbook chapters because the topic required a broad research approach.
Search Strategy
The primary literature search was conducted using PubMed/MEDLINE, focusing on publications from 2010 to 2025. The search included terms which combined “primary immunodeficiency” with “inborn errors of immunity” and “severe combined immunodeficiency” and “pediatric” and “children” and “diagnosis” and “treatment” and “immunoglobulin replacement” and “hematopoietic stem cell transplantation.” The search strategy used MeSH terms and Boolean operators to achieve maximum search sensitivity and specificity. Researchers conducted a focused systematic review search by using the PubMed systematic review filter to find high-level evidence.
Inclusion Criteria
The researchers selected sources according to five requirements which they established as their inclusion criteria.
(1) The first requirement required sources to demonstrate they studied pediatric populations who be- longed to the age range of 0 through 18 years.
(2) The second requirement mandated sources to achieve publication through peer-reviewed journals or recognized health organizations.
(3) The third requirement demanded sources to provide information in the English language.
(4) The fourth requirement restricted publication to sources created within the past 15 years except for works which established foundational historical knowledge.
(5) The fifth requirement demanded sources to demonstrate direct connection with clinical diagnosis and treatment.
The researchers prioritized systematic reviews and meta-analyses and multicenter studies and evidence- based clinical guidelines.
Data Sources
The research team combined primary literature with data from multiple respected sources which included the following materials:
• The Centers for Disease Control and Prevention (CDC) guidelines on primary immunodeficiency
• Australian National Blood Authority criteria for immunoglobulin therapy
• MSD Manual Professional Edition clinical approaches
• Journal of Pediatric Pulmonology editorial content
• Recent gene therapy trial publications
• Epidemiological studies from developing world contexts
• Royal Australian College of General Practitioners clinical guidance
Data Extraction and Synthesis
The team extracted essential details about classification systems and clinical warning signs and diagnostic testing methods and treatment criteria and outcome data. The study used available quantitative data from epidemiological studies to create tables which showed how different immunodeficiency categories occurred and spread throughout the population. The clinical recommendations developed through evidence-based guidelines which the team used to verify consistency across various sources.
Limitations
This review is narrative rather than systematic in nature, and therefore does not employ formal quality assessment tools or meta-analytic techniques. The different research methods and participant groups used in the studies make it impossible to combine their results through quantitative analysis. The ongoing developments in genetic diagnosis and targeted therapies require that certain recommendations will need updating when new evidence becomes available.
Results
Classification of Immunodeficiency States
Immunodeficiency states in children are broadly categorized into primary (genetically determined) and secondary (acquired) forms. The initial distinction of these two categories affects three critical aspects which include diagnosis and treatment methods as well as clinical outcome prediction.
Primary Immunodeficiency (Inborn Errors of Immunity)
The IUIS expert committee has established a phenotypic classification system that complements genotypic characterization. The system currently includes 485 different genetic disorders which experts have categorized into ten primary disease groups according to the 2022 update. The current classification system displays its existing framework through Table 1 which includes example cases for demonstration.
Secondary Immunodeficiency
Acquired immunodeficiency significantly outnumber primary forms in clinical practice. The most recognized cause globally remains HIV infection, though in resource-rich settings, iatrogenic immunosuppression represents the predominant etiology. Table 2 summarizes major causes of secondary immunodeficiency in children.
Epidemiology and Demographic Patterns
Current epidemiological studies demonstrate essential patterns which show how pediatric immunodeficiency disorders spread and how they clinically manifest. Researchers at the University of Child Health Sciences conducted a study from 2021 to 2023 in which they tested 81 children who showed symptoms of primary immunodeficiency according to Jeffrey Modell Foundation warning signs. The patients had their first symptoms at an age which reached a median point of 4 months while their median age at presentation was 17 months with a range of 2 to 156 months. The differences between these two groups resulted in a diagnostic delay which reached a median value of 10.5 months because medical professionals throughout the world face difficulties which prevent them from diagnosing patients within the appropriate timeframe.
The study found that males represented 60 percent of participants while females made up 40 percent of the total population. This pattern of male predominance appears because several common disorders including X-linked agammaglobulinemia and Wiskott-Aldrich syndrome follow X-linked inheritance pat- terns. Consanguinity appeared as a major risk element because it affected 80.8 percent of the children who suffered from the condition while 53.8 percent of families showed positive genetic links and 37.2 percent reported sibling fatalities. Egyptian research reported consanguinity rates at 55.5 percent while
46.9 percent of participants showed family history of genetic disorders.
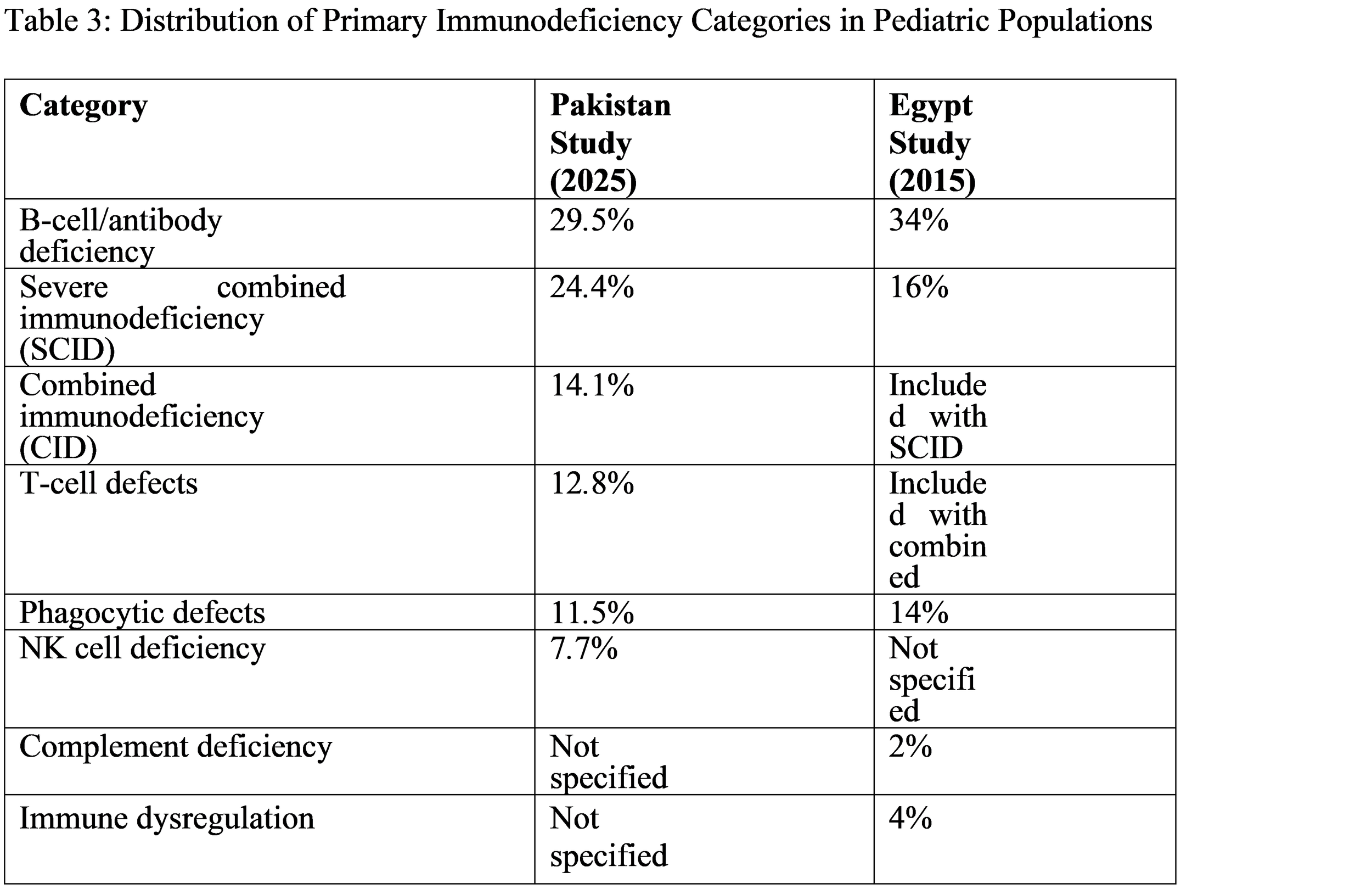
Various populations show different patterns of immunodeficiency category distribution yet there exists a constant trend which shows antibody deficiencies as the most common type of immunodeficiency. The researchers present their findings from two recent studies in Table 3 for comparison purposes.
Clinical Manifestations and Warning Signs
Immunodeficiency shows wide clinical presentation because patients can show either no symptoms or extreme severe life-threatening infectious diseases. The main characteristic of the condition exists as increased risk for infections, but the specific types of infections which occur through the condition reveal essential information about the person’s immune system impairment.
People develop different types of infections according to which parts of their immune system become active to fight against specific kinds of pathogens. Table 4 summarizes these relationships.
The Jeffrey Modell Foundation Warning Signs
The Jeffrey Modell Foundation created 10 warning signs which help medical professionals to identify primary immunodeficiency at its first stages. The signs continue to function as screening instruments which medical professionals use in primary care environments. Researchers studied a Pakistani group to determine which warning signs appeared among patients with confirmed PIDD diagnosis.
• Need for intravenous antibiotics to clear infections: 88.5%
• Two or more pneumonias within 12 months: 76%
• Failure to thrive or growth retardation: common but not quantified
• Family history of PIDD: 53.8%
• Recurrent deep skin or organ abscesses: 10.3%
• Two or more deep-seated infections including septicemia: 5.1%
• Two or more sinus infections within 12 months: 11.5%
• Persistent oral or skin fungal infections: 51.3% (thrush)
• Infection requiring prolonged antibiotics: universal in severe cases
Physical Examination Findings
Beyond infection patterns, physical examination may reveal characteristic findings that point toward specific diagnoses. The Pakistani study documented the frequency of various physical findings in confirmed PIDD patients:
Oral thrush affects 51.3 percent of patients.
• Hepatomegaly occurs in 16.7 percent of cases.
• Lymphadenopathy appears in 6.4 percent of patients.
• The presence of clubbing indicates chronic suppurative lung disease in 11.5 percent of cases.
• Skin manifestations which include pyoderma and eczema and seborrhea occur in 10 to 28 percent of cases.
• The rate of silvery hair or occult-cutaneous albinism occurs at 5 to 8 percent of the population according to specific syndromes.
• The rate of delayed umbilical cord separation which exceeds three weeks happens in 3.8 percent of cases which indicates leukocyte adhesion deficiency.
Diagnostic Approach
The diagnostic evaluation of suspected immunodeficiency follows a stepwise approach which begins with clinical suspicion and progresses through screening tests before reaching definitive diagnostic studies.
Initial Screening Investigations
The initial laboratory evaluation should be accessible and inexpensive while its abilities to identify common immunodeficiency patterns must succeed. Essential screening tests include:
1. Complete Blood Count with Manual Differential: This fundamental test can reveal:
• Lymphopenia (absolute lymphocyte count <2,000/mcL at birth, <4,500/mcL at 9 months, or
<1,000/mcL in older children), suggesting T-cell deficiency
• Neutropenia (absolute neutrophil count <1,200/mcL), suggesting congenital or cyclic neutropenia
• Thrombocytopenia, suggesting Wiskott-Aldrich syndrome in males
• Persistent leukocytosis, suggesting leukocyte adhesion deficiency
• Howell-Jolly bodies on peripheral smear, suggesting asplenia
2. Quantitative Immunoglobulin Levels: Measurement of IgG, IgA, and IgM requires interpretation against age-matched normal values, as levels are physiologically lower in infancy. An IgG level <200 mg/dL (<2 g/L) indicates significant antibody deficiency, though levels must be interpreted in context.
3. Specific Antibody Responses: Assessment of functional antibody responses through pre- and post-vaccination titers (tetanus, diphtheria, H. influenzae type b, pneumococcal polysaccharides) can identify specific antibody deficiency even when total immunoglobulin levels are normal.
4. Delayed-Type Hypersensitivity Testing: Skin testing with Candida antigen assesses T-cell function, though results may be negative in unexposed infants.
Newborn Screening for SCID
The implementation of newborn screening for severe combined immunodeficiency using T-cell receptor excision circle (TREC) analysis represents a major public health advance. TRECs are circular DNA fragments generated during T-cell receptor rearrangement in the thymus; their absence on dried blood spot screening indicates failed T-cell production. All 50 US states now include SCID screening in their newborn panels, enabling presymptomatic diagnosis and treatment before life-threatening infections develop.
Advanced Diagnostic Testing
When screening tests suggest immunodeficiency or clinical suspicion remains high despite normal screening, specialized testing is indicated:
• Flow cytometry for lymphocyte phenotyping enables researchers to measure T-cell quantities through CD3 detection and T-cell subtypes through CD4 and CD8 and B-cell quantities through CD19 detection and NK cell quantities through CD56 detection. The test results play a crucial role in diagnosing combined immunodeficiency disorders and agammaglobulinemia.
• Lymphocyte proliferation assays evaluate T-cell activity through their response to the mitogen phytohemagglutinin and the mitogen concanavalin A and the antigens used in the test.
• Neutrophil Function Tests (Dihydrorhodamine flow cytometry) enable assessment of respiratory burst activity which helps diagnose chronic granulomatous disease.
• Complement testing (CH50 and AH50) evaluate the functionality of the classical and alter- native complement pathways.
• Genetic testing uses targeted gene sequencing and gene panels and whole exome sequencing to establish permanent molecular diagnoses which now include 485 genes associated with immune dysregulation disorders.
The European Society for Immunodeficiencies (ESID) has established diagnostic criteria for common disorders through their establishment of diagnostic standards for specific disorders. The diagnosis of common variable immunodeficiency (CVID) in children older than 2 years requires the following three criteria to be satisfied:
1. The patient needs to demonstrate a significant decline in IgG levels together with a significant decline in IgA levels which may or may not include a decrease in IgM levels.
2. The test results need to show that the patient failed to develop antibodies after receiving vaccines.
3. The patient needs to be diagnosed with hypogammaglobulinemia which results from a specific medical condition that has been recognized and documented.
4. The patient experiences either heightened infection risk or exhibits autoimmune symptoms together with either granulomatous disease or lymphoproliferation or both conditions.
Management Strategies
The management of pediatric immunodeficiency requires three connected methods which include infection prevention together with supportive care and missing immune components replacement and ultimate restoration of the basic immune system defect.
Infection Prevention
All children with immunodeficiency require comprehensive infection prevention strategies:
• Hand hygiene and avoidance of sick contacts
• Antimicrobial prophylaxis: Trimethoprim-sulfamethoxazole for PJP prevention in T-cell defects; itraconazole for fungal prophylaxis in chronic granulomatous disease
• Vaccination considerations: Live vaccines (MMR, varicella, rotavirus, intranasal influenza, oral polio) are contraindicated in most T-cell deficiencies and severe combined immunodeficiency. Killed vaccines are generally safe but may be ineffective in antibody-deficient patients.
• Immunoglobulin monitoring: Live vaccines should be avoided in household contacts of severely immunocompromised patients when possible.
Immunoglobulin Replacement Therapy
For antibody deficiencies, immunoglobulin (IG) replacement represents the cornerstone of management. The two available formulations, subcutaneous (SCIG) and intravenous (IVIG), provide equivalent treatment effectiveness. The Australian National Blood Authority has established specific qualifying criteria for IG therapy:
For CVID meeting ESID criteria:
• Patient >2 years of age
• Marked decrease of IgG and IgA on two occasions
• Documented vaccine failure OR IgG <2 g/L with significant infection risk OR absent isohemagglutinins OR low switched memory B-cells
• Increased infection susceptibility OR autoimmune manifestations/lymphoproliferation/family his- tory
For transient hypogammaglobulinemia of infancy (children <4 years):
• Therapy considered only if recurrent suppurative infections threaten organ function
• Cessation should be attempted after 24 months or when IgA and IgM normalize
• Some patients require only seasonal therapy during winter months.
Hematopoietic Stem Cell Transplantation
The procedure of hematopoietic stem cell transplantation (HSCT) provides a permanent cure for patients with severe combined immunodeficiency, Wiskott-Aldrich syndrome, chronic granulomatous disease and other serious medical conditions. Transplantation produces optimal results when it occurs during early stages of treatment before the patient develops major infectious complications. Newborn screening pro- grams aim to facilitate presymptomatic transplantation in SCID.
Gene Therapy
The development of new gene therapy techniques has created better treatment results for particular medical conditions. The New England Journal of Medicine published a landmark study which tracked the long-term results of autologous hematopoietic stem cell treatment for 62 children with adenosine deaminase-deficient SCID (ADA-SCID) who received lentiviral vector-based ADA gene therapy. The results proved that:
• The procedure achieved successful immune system restoration in 59 out of 62 patients achieving a success rate of 95 percent
• The patients maintained their immune system function for a decade after receiving treatment
• The procedure did not result in any complications that would restrict treatment options
• The procedure achieved success through the use of frozen cells which provided treatment access to patients throughout the world.
The research team leader Dr. Donald Kohn from UCLA said that “These results are what we hoped for when we first began developing this approach. The durability of immune function, the consistency over time and the continued safety profile are all incredibly encouraging”. The study represents the longest research on ADA-SCID gene therapy which spans 474 patient-years and includes 474 patient-years of follow-up data and researchers expect to receive FDA approval within 2 to 3 years.
Supportive Care and Monitoring
Long-term management requires multidisciplinary care including:
• The medical team needs to monitor patients growth and development throughout their treatment period.
• Patients undergo pulmonary function testing and imaging to track bronchiectasis progression.
• The team conducts audiologic assessment to detect hearing loss caused by infections.
• Patients receive nutritional assistance.
• The team provides psychological assistance to both patients and their families.
• Genetic counseling services are offered to families who have members with genetic disorders.
Outcomes and Prognosis
The prognosis for children with immunodeficiency has improved dramatically over recent decades, though it remains highly variable depending on the specific diagnosis, severity, and timeliness of intervention.
Historical mortality rates reached their highest points because severe combined immunodeficiency caused death within the first two years of life in all untreated patients. The current outcomes show marked enhancement from previous results. The Egyptian study reported 28.4% mortality among diagnosed PIDD patients, primarily from infectious complications. The combination of earlier diagnosis together with expanded access to definitive treatment methods results in decreased mortality rates.
Morbidity
Chronic complications remain significant even among treated patients. Recurrent infections can lead to:
• Bronchiectasis and chronic lung disease
• Hearing loss which results from repeated otitis media infections
• Sinusitis together with chronic sinus disease
• Growth failure together with developmental delay
• Autoimmune complications which affect people with immune dysregulation disorders
• Increased malignancy risk which affects especially lymphoma
Factors which affect results
The main factors which determine prognosis results are:
• Age at diagnosis: Earlier diagnosis consistently predicts better outcomes
• Specific diagnosis: Some disorders (e.g. complete DiGeorge syndrome) carry worse prognoses than others
• Access to definitive therapy: HSCT and gene therapy availability dramatically alter outcomes
• Infection history prior to treatment: Established organ damage is irreversible
• Adherence to supportive care: Prophylaxis and immunoglobulin replacement reduce infectious complications
Discussion
The present understanding of pediatric immunodeficiency has developed through two major stages since people used to think of these disorders as uncommon conditions that always resulted in death. Current evidence positions inborn errors of immunity as significant contributors to childhood morbidity, with prevalence estimates approaching 1 in 1,200 live births. The new paradigm change creates deep effects which affect both medical work and public health policies and scientific research funding decisions.
The Challenge of Diagnostic Delay
Diagnostic delay continues to be the primary factor which doctors and researchers can change to improve patient outcomes in their work. A recent Pakistani cohort study found a median delay of 10.5 months which matches the Egyptian study results showing patients received their diagnosis at an average age of
27.4 months. The period of the delay functions as a vital time frame because it leads to permanent organ damage through infectious agents which develop into an unhealable state that makes the body unable to function normally.
The process of diagnosing a condition experiences delays because multiple reasons exist. The physiologic state of healthy infants creates difficulty for doctors to identify which respiratory infections represent actual medical conditions because healthy infants experience up to 10 respiratory infections every year. The Jeffrey Modell Foundation warning signs provide helpful information but they do not accurately identify all milder phenotypes and unusual cases. The majority of low- and middle-income countries face major obstacles which prevent their citizens from accessing specialized immunological testing as they deal with high rates of undiagnosed immunodeficiency.
The observation that consanguinity was present in 80.8% of affected children in Pakistan and 55.5% in Egypt highlights the importance of autosomal recessive inheritance patterns in populations with high rates of consanguineous marriage. The results indicate that direct population screening together with genetic testing efforts will provide substantial benefits for these communities and their members.
The Spectrum of Disease
Recent studies have examined how different immunodeficiency categories distribute through various immunodeficiency categories to deliver key research findings. The historical pattern shows that approximately 30% of cases involve antibody deficiencies while the Pakistani cohort shows an exceptional 24.4% SCID rate which exceeds normal estimates. The distribution of severely sick infants to tertiary hospitals creates a possibility of referral bias while the actual population distribution in the disease exists.
The isolated NK defects found in 7.7% of patients with NK cell deficiency represent a significant finding because these defects were previously regarded as uncommon. The current finding demonstrates better diagnostic capabilities which use flow cytometric immunophenotyping as routine practice because these disorders remain underdiagnosed despite their actual presence in patients.
Advances in Diagnosis and Treatment
The public health system experiences a complete transformation through the implementation of newborn screening for SCID which uses TREC analysis. The screening programs enable presymptomatic diagnosis which helps doctors to start treatment before patients develop life-threatening infections that lead to severe medical problems. The United States uses this method as the standard practice which other countries should follow when they develop their screening programs.
Genetic testing has revolutionized diagnostic precision, with 485 distinct genetic defects now recognized. The expanding genetic architecture shows extreme genetic diversity because different gene mutations create distinct phenotypes while two different genes produce identical clinical symptoms. The IUIS classification system continues to evolve to accommodate this complexity, incorporating both phenotypic and genotypic information.
The most impressive medical treatment development brings gene therapy research from its initial testing stage to its current complete implementation. The recently disclosed long-term results of lentiviral gene therapy treatment for ADA-SCID show that patients achieve permanent immune system restoration which maintains high safety standards throughout treatment. The successful application of frozen cells eliminates operational challenges which hinder worldwide adoption thus making this life-saving treatment available to more people. The development of gene editing methods will result in new treatment options for all monogenic immune system disorders which are currently available.
Clinical Implications
The review presents multiple essential principles which medical practitioners should follow. The first point establishes that all children who experience severe or rare infections with accompanying weight loss symptoms and family history of immune system disorders and parents from related backgrounds should receive evaluation for immunodeficiency. The particular infection patterns which patients present to doctors help physicians discover which immune system functions require assessment. Medical professionals should use screening tests which include CBC with differential and quantitative immunoglobulins because these tests exist in all medical facilities and should be used whenever testing becomes necessary. When patients show abnormal screening results or when there is clinical suspicion about their health, medical professionals need to contact clinical immunologists immediately.
The treatment of affected children needs doctors, immunologists, infectious disease specialists, pulmonologists, nutritionists and social workers to work together as a qualified team. The process of long-term follow-up needs to continue because it helps track complications while it evaluates treatment success and offers suitable developmental assistance for each age group.
Research Priorities
Researchers have achieved major advancements yet they still encounter multiple knowledge deficiencies. Scientists have not yet identified the genetic factors responsible for various immunodeficiency disorders which exist in non-European populations that need more research. Researchers need to investigate which antimicrobial prophylaxis methods provide the best protection and which timeframes show optimal results. Scientists need to study how newborn screening programs identify immunodeficiency diseases that exist beyond SCID. Medical professionals must track the long-term health of gene therapy patients to monitor their potential development of cancer and autoimmune disorders. Research on implementation science needs to create methods which help people find correct medical diagnoses and access treatment in areas with limited resources.
Limitations
This review has several limitations. The narrative methodology, while appropriate for synthesizing diverse information, does not employ systematic review techniques or formal quality assessment. The included studies show such diverse characteristics that researchers cannot perform quantitative meta-analysis. The epidemiological research uses data from single-center studies which may introduce referral bias. The fast development of this research area will lead to new genetic and treatment information which will replace existing knowledge.
Conclusion
Children with immunodeficiency states develop multiple disorders which all share the same problem with their ability to defend against infections. The medical community has experienced a major shift in understanding that occurs when they now treat these diseases as common pediatric diseases instead of uncommon medical conditions. Clinicians who treat children need to recognize inborn errors of immunity as a critical issue because scientists have discovered more than 485 genetic defects which affect this condition and current research indicates that 1 in 1,200 live births results in this disorder.
Immunodeficiency shows its clinical symptoms through the occurrence of multiple severe infections which happen at unusual times but doctors can detect the underlying immune defect through the specific types of infections which the patient experiences. Children who have antibody deficiencies will start to show symptoms after they reach six months of age because they will develop sinopulmonary infections from bacteria that have protective capsules. The first signs of T-cell deficiencies appear through infections which occur from viral, fungal, and opportunistic pathogens. Phagocyte defects cause patients to develop deep abscesses that take a long time to heal. People who have complement deficiencies develop two medical problems which include autoimmune disorders and infections from encapsulated bacteria. The warning signs from the Jeffrey Modell Foundation serve as an effective screening tool yet doctors need to use their professional expertise when evaluating patients.
Diagnostic evaluation begins with clinical suspicion which then leads to screening tests before reaching definitive studies. A complete blood count with differential together with quantitative immunoglobulins and specific antibody responses serves as the first laboratory assessment. The patient needs more advanced testing when test results become abnormal or when doctors continue to suspect a medical problem because of their clinical findings. The development of TREC analysis for newborn screening of severe combined immunodeficiency has enabled new testing methods.
You accumulate knowledge from your training until the month of October in the year 2023. The process of management includes three essential parts which involve preventing infections and restoring lost immune system elements and fixing the main health problem. The primary treatment for anti- body deficiencies requires immunoglobulin replacement therapy which has established guidelines for both treatment and patient assessment. The treatment of severe combined immunodeficiency and other critical medical conditions can be achieved through hematopoietic stem cell transplantation which produces the best results when performed at an early stage of treatment. The new gene therapy method has brought about significant progress in treating particular diseases because research from ADA-SCID studies shows that patients maintain their immune system recovery while their safety remains intact.
Children without diagnosis exists because it enables between two outcomes, which include a lifetime of preventable morbidity and the opportunity for definitive intervention. Our shared duty as clinicians and educators and researchers demands that we create systems which prevent any child from losing this essential period of growth.
References
[1] Booth C, Masiuk K, Kohn DB, et al. Long-Term Safety and Efficacy of Gene Therapy for Adenosine Deaminase Deficiency. New England Journal of Medicine. 2025. doi:10.1056/nejmoa2502754
[2] Centers for Disease Control and Prevention. About Primary Immunodeficiency (PI). December 5, 2024. https://www.cdc.gov/primary-immunodeficiency/about/index.html
[3] Fernandez J. Approach to the Patient With Suspected Immunodeficiency. MSD Manual Professional Edition. October 2024. https://www.msdmanuals.com/ professional/immunology-allergic-disorders/immunodeficiency-disorders/
approach-to-the-patient-with-suspected-immunodeficiency
[4] Galal AA, Heiba DAE, Abdelkader HAA. Study of suspected cases of primary immunodeficiency disease attending Alexandria University children’s hospital; a one year study. Alexandria Journal of Pediatrics. 2015;29(1):29-37
[5] National Blood Authority Australia. Inborn errors of immunity (IEI) (primary immunodeficiency diseases) with antibody deficiency. April 14, 2025. https://criteria.blood.gov.au/ MedicalCondition/View/2721
[6] O’Sullivan M, McLean-Tooke A, Loh R. Evaluating for immunodeficiency in children with recurrent infection. Australian Family Physician. 2014;43(9):602-608
[7] Sarath Balaji B. Primary Immunodeficiency in Children: An Overview. Journal of Pediatric Pulmonology. 2024;3(2):33-34. doi:10.4103/jopp.jopp_25_24
[8] Shahzad F, Saleem A, Ali T, et al. Spectrum of different categories of Primary Immunodeficiency Disorders diagnosed at Children Hospital. Pakistan Journal of Medical Sciences. 2025;41(2):569-574. doi:10.12669/pjms.41.2.9511
[9] Zenodo. Risk Factors and Early Markers of Primary Immunodeficiencies in Pediatric Practice. November 1, 2025. https://zenodo.org/records/17471773