
Physiology of Adrenal Glands and Adrenaline
1. Alimbekova Aiperi Alimbekovna
2. Velladurai Kaushik
(1. Lecturer, International Medical Faculty, Osh State University, Kyrgyz Republic.
2. Student, International Medical Faculty, Osh State University, Kyrgyz Republic.)
ABSTRACT
The adrenal glands are a pair of tiny but important endocrine organs situated above the kidneys; they help regulate homeostasis and respond to stress in the body. This paper provides insight into the physiology and pathology associated with the production of adrenal hormones. The adrenal glands include a cortex that forms the outer shell of the organ and a medulla forming the core. The cortex generates corticosteroid hormones like cortisol, aldosterone, and androgens, whereas the medulla releases catecholamine hormones, primarily adrenaline and noradrenaline.A detailed description of hormone synthesis and secretion, as well as the mode of action of each of them, is provided. Adrenaline is especially important since it quickly prepares the body for "fight-or-flight" via increased heart rate and energy. Conversely, cortisol and aldosterone are responsible for long-term regulation of metabolism and immune response. Further, information about the pathway of corticosteroid hormones through the bloodstream and further processing and elimination of the hormones is provided.Addison's disease, Cushing syndrome, and hyperaldosteronism, which indicate adrenal malfunction, are considered examples of major diseases associated with the endocrine glands. In conclusion, it is clear that adrenal hormones play an essential role in homeostasis.
INTRODUCTION:
The adrenal glands are important endocrine organs that sit above the kidneys. They are very small, but they are very important for controlling metabolism, fluid balance, and how the body reacts to stress. Adrenaline is one of the most important hormones they make. It gets the body ready to respond quickly to emergencies by activating the "fight-or-flight" response.
ANATOMY OF ADRENAL GLAND:
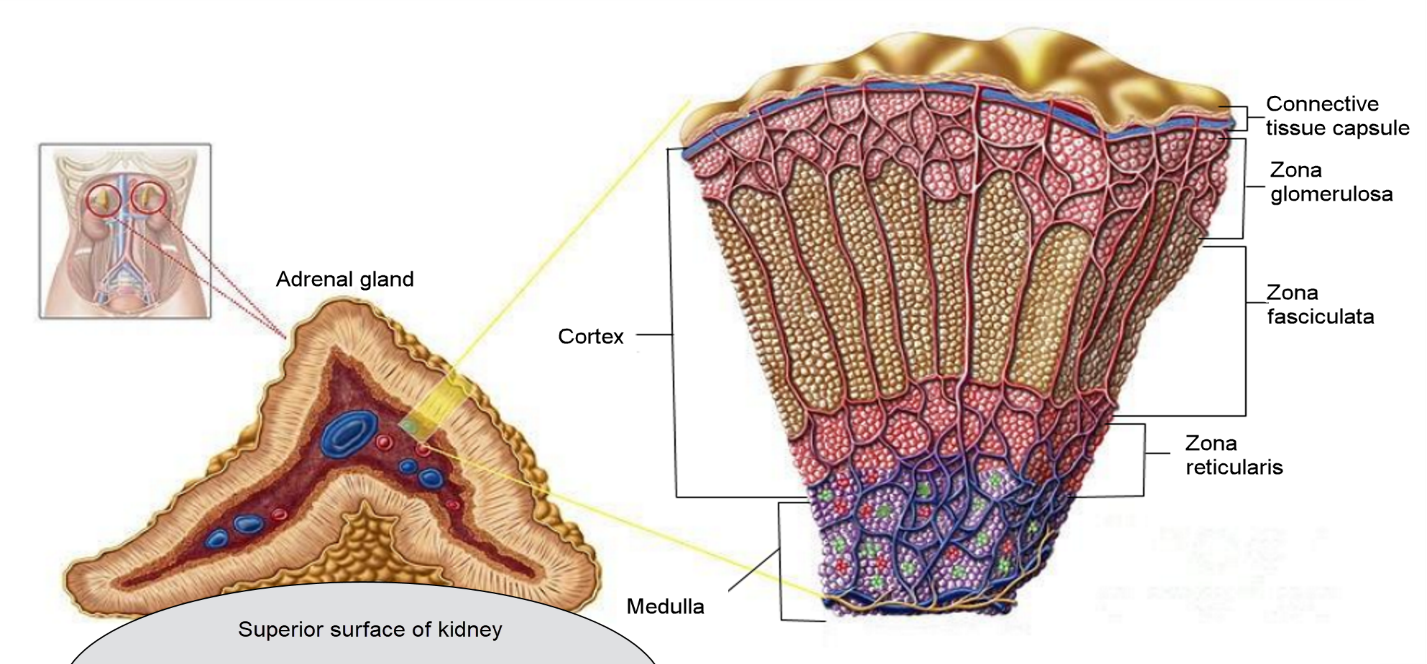
The adrenal glands, also known as suprarenal glands, are paired endocrine organs located at the upper poles of the kidneys. Each gland is situated above a kidney and in front of the diaphragm. They are surrounded by fatty tissue and enclosed within the perirenal fascia, with a septum separating them from the kidneys. The right adrenal gland is triangular or pyramidal in shape, whereas the left is semilunar. Each gland measures about 5 cm in height and weighs approximately 5 grams.
Structurally, each adrenal gland consists of two distinct parts: the outer cortex and the inner medulla. The cortex forms the major portion and is divided into three zones. The outer zona glomerulosa produces mineralocorticoids that regulate salt and water balance. The middle zona fasciculata secretes glucocorticoids involved in metabolism and stress response. The inner zona reticularis produces small amounts of sex hormones.
The inner medulla, which develops from neural crest cells, contains chromaffin cells that secrete catecholamines, mainly adrenaline and noradrenaline. These hormones are released in response to stimulation by the sympathetic nervous system and are responsible for the rapid “fight-or-flight” response. (Fig:1)
SYNTHESIS AND SECRETION OF ADRENALINE:
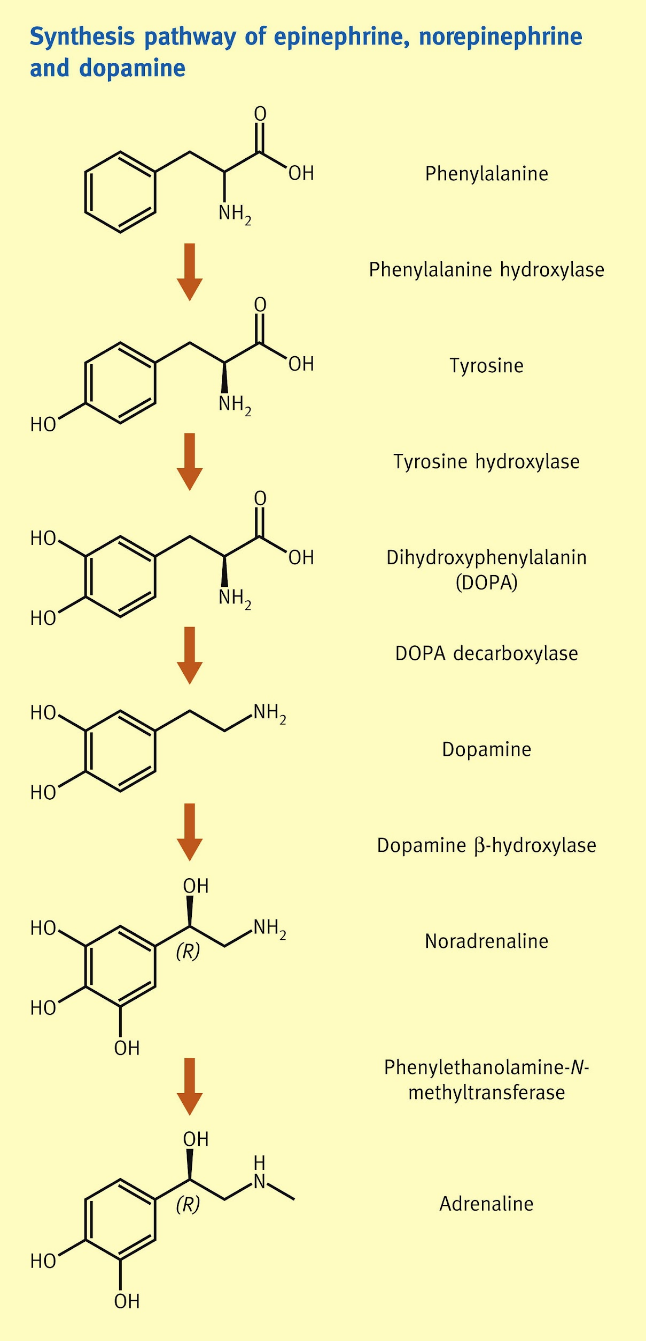
Norepinephrine (NE) is the primary neurotransmitter released by postganglionic sympathetic nerves, and its synthesis begins with the amino acid tyrosine. Tyrosine is actively transported into the nerve terminal, where it undergoes a sequence of enzymatic conversions. First, it is converted into L-DOPA by the enzyme tyrosine hydroxylase, which represents the rate-limiting step in the pathway. L-DOPA is then converted into dopamine by DOPA decarboxylase. The dopamine formed in the cytoplasm is transported into synaptic vesicles, where it is further converted into norepinephrine by dopamine β-hydroxylase. Once synthesized, norepinephrine is stored within these vesicles until it is needed for release.
The secretion of norepinephrine occurs in response to an action potential traveling down the sympathetic nerve fiber. When the electrical impulse reaches the nerve terminal, it causes depolarization of the membrane, leading to the opening of voltage-gated calcium channels. The influx of calcium ions into the neuron is the key trigger for neurotransmitter release. Increased intracellular calcium promotes the movement of vesicles toward the presynaptic membrane, where they fuse and release norepinephrine into the synaptic cleft through exocytosis. In addition to norepinephrine, other substances such as dopamine β-hydroxylase and co-transmitters like ATP may also be released. The released norepinephrine then binds to adrenergic receptors on the target tissue, initiating the appropriate physiological response.
Epinephrine (Epi), in contrast, is primarily synthesized in the adrenal medulla and functions as a hormone. Its synthesis follows the same initial steps as norepinephrine formation, beginning with tyrosine and progressing through L-DOPA and dopamine to form norepinephrine. However, norepinephrine undergoes an additional enzymatic modification in chromaffin cells, where it is converted into epinephrine by phenylethanolamine-N-methyltransferase. The epinephrine produced is then transported back into storage vesicles. Upon stimulation by preganglionic sympathetic nerves, chromaffin cells depolarize, allowing calcium to enter the cells and trigger vesicle fusion with the cell membrane. This results in the release of epinephrine directly into the bloodstream, enabling it to act on distant organs. Approximately 80% of the catecholamines released from the adrenal medulla is epinephrine, while the remaining 20% is norepinephrine, reflecting their complementary roles in the body’s response to stress. (Fig:2)
METABOLISM OF ACTION:
Catecholamines such as epinephrine and norepinephrine exert their physiological effects by binding to specific adrenergic receptors, which are broadly classified into α (alpha) and β (beta) types. The β receptors are further divided into β₁, β₂, and β₃ subtypes, while the α receptors include α₁ and α₂, each of which has additional subtypes. Although both epinephrine and norepinephrine can act on all adrenergic receptors, they show relative selectivity in their actions: epinephrine tends to have a stronger effect on β receptors, whereas norepinephrine predominantly acts on α receptors. Structurally, β₁, β₂, and α₂ receptors share similarities, which is reflected in some overlap in their signaling behavior.
The intracellular effects of catecholamines depend on the type of receptor they activate. β₁, β₂, and β₃ receptors are coupled to stimulatory G proteins that activate adenylyl cyclase, leading to an increase in cyclic AMP (cAMP) levels within the cell. This rise in cAMP acts as a second messenger, triggering a cascade of cellular responses. In contrast, α₂ receptors are coupled to inhibitory G proteins, which suppress adenylyl cyclase activity and reduce intracellular cAMP levels. On the other hand, α₁ receptors operate through a different signaling pathway involving phosphatidylinositol. Activation of these receptors leads to the formation of second messengers diacylglycerol (DAG) and inositol triphosphate (IP₃), which promote calcium release from intracellular stores and mediate the cellular response.
Steroid hormones such as cortisol act through a fundamentally different mechanism that involves regulation of gene expression. Because cortisol is lipid-soluble, it diffuses easily across the cell membrane and binds to glucocorticoid receptors located in the cytoplasm. In its inactive state, the receptor is bound to a heat shock protein complex, which is displaced upon cortisol binding. This interaction alters the receptor’s configuration and leads to its activation through hyperphosphorylation. The hormone–receptor complex then translocates into the nucleus, where it binds to specific DNA sequences known as glucocorticoid regulatory elements. This binding initiates the transcription of messenger RNA, ultimately resulting in the synthesis of proteins that modify cellular function. Due to this genomic mechanism, the effects of cortisol typically take hours to days to become apparent.
Aldosterone, another steroid hormone, also acts primarily through intracellular receptors and gene regulation. After diffusing into the cell, aldosterone binds to cytoplasmic receptors, and the resulting hormone–receptor complex moves into the nucleus to promote transcription of specific genes. One of the key genes activated is the serum and glucocorticoid-regulated kinase (SGK) gene, which plays a critical role in increasing the activity of epithelial sodium channels (ENaC). Aldosterone enhances the synthesis of ENaC subunits, promotes their insertion into the cell membrane, and increases their functional activity, leading to greater sodium reabsorption
PHYSIOLOGY EFFORTS OF ADRENALINE:
Adrenaline, also known as epinephrine, is a powerful hormone released mainly from the adrenal medulla. It plays a crucial role in helping the body respond to stress and sudden demands. In fact, the adrenal medulla produces more than 90% of the adrenaline found in the bloodstream, while only very small amounts are present in other tissues. When the adrenal glands are removed, adrenaline levels in the blood become almost undetectable, showing how important this gland is as its primary source.
Adrenaline works by acting on adrenergic receptors, which are divided into alpha (α₁, α₂) and beta (β₁, β₂, β₃) types. Although both adrenaline and norepinephrine can activate these receptors, adrenaline has a stronger effect on beta receptors, especially β₂ receptors. Through these receptors, adrenaline influences many body systems at once, including the heart, lungs, and metabolism.
One of the most important roles of adrenaline is in the body’s “fight-or-flight” response, a concept first described by Walter Bradford Cannon. During stressful or threatening situations, adrenaline is rapidly released into the bloodstream. This prepares the body for immediate action by increasing heart rate, improving blood flow to vital organs, and releasing stored energy. Interestingly, even though adrenaline plays a major role in this response, the body can still survive without the adrenal medulla, as other systems help compensate when needed.
Exercise is one of the strongest natural triggers for adrenaline release. As physical activity increases, especially when it becomes intense, adrenaline levels rise significantly. This helps the body meet higher energy demands by improving circulation and oxygen delivery. At the same time, adrenaline relaxes the airways, making breathing easier and more efficient. This effect is mainly due to stimulation of β₂ receptors and occurs even without direct nerve supply to the lungs.
Adrenaline is also closely linked to emotional responses, especially fear. When adrenaline levels rise, people often experience physical changes such as a faster heartbeat, trembling, and increased alertness. These changes can make emotions feel more intense. Research shows that higher levels of adrenaline are associated with stronger feelings of fear and more vivid emotional experiences, even if the actual situation is not extremely threatening.
Another important effect of adrenaline is its role in memory. It helps strengthen the storage of memories, particularly those linked to emotional or stressful events. This means that experiences associated with high adrenaline levels are more likely to be remembered clearly. Although adrenaline does not easily enter the brain, it still influences memory through signals involving β receptors outside the brain. Blocking these receptors has been shown to reduce the memory-enhancing effects of adrenaline.
FLIGHT OR FIGHT RESPONSE:
The fight-or-flight response is the body’s natural reaction to a perceived threat or stressful situation. It prepares an individual to either confront danger (“fight”) or escape from it (“flight”). This response is driven by the release of catecholamine hormones such as adrenaline and norepinephrine, which trigger rapid physical and emotional changes in the body.
When activated, the body undergoes several immediate physiological adjustments to enhance survival. Blood flow is redirected toward the muscles and brain, improving strength, alertness, and reaction speed, while reducing activity in less urgent systems like digestion. Heart rate and blood pressure increase to deliver more oxygen and nutrients to tissues. At the same time, the liver releases glucose and fats into the bloodstream to provide quick energy. Breathing becomes faster to meet the body’s increased oxygen demand, and pupils dilate to improve vision. Muscles become tense, preparing for action, which may sometimes cause trembling.
Additionally, blood clotting ability increases to minimize potential blood loss in case of injury. Alongside these physical changes, emotional responses also play an important role. The intensity of fear or stress influences how a person reacts, whether by staying calm, becoming anxious, or acting aggressively. Emotional regulation helps control these reactions, allowing individuals to respond more effectively to threats. People with better emotional control are generally able to manage stress more efficiently, while those with higher emotional reactivity may experience stronger anxiety or defensive behaviors.
ROLE IN METABOLISM:
The adrenal glands produce a variety of hormones that are essential for maintaining balance in the body, especially during stress. These hormones can be broadly divided into two groups: steroid hormones from the adrenal cortex and catecholamines from the adrenal medulla. Together, they regulate metabolism, blood pressure, electrolyte balance, and the body’s response to stress.
One of the most important hormones is cortisol, a glucocorticoid that plays a key role in metabolism. It helps the body use fats, proteins, and carbohydrates efficiently, ensuring a steady supply of energy. Cortisol also reduces inflammation, supports normal blood pressure, and increases blood sugar levels when needed. In addition, it helps regulate the sleep–wake cycle. During stressful situations, cortisol is released in higher amounts to help the body cope by providing extra energy and maintaining stability.
Another vital hormone is aldosterone, a mineralocorticoid that primarily controls blood pressure and electrolyte balance. It regulates the levels of sodium and potassium in the blood, which in turn influences fluid balance and blood volume. By controlling these electrolytes, aldosterone also helps maintain the body’s pH within a normal range. This function is crucial for proper functioning of cells and organs.
The adrenal glands also produce small amounts of DHEA and other androgenic steroids. These are considered weak male hormones, but they serve as precursors for stronger sex hormones. In females, they can be converted into estrogens in the ovaries, while in males, they contribute to androgen production in the testes. Although their direct effects are limited, they play a supportive role in the development of secondary sexual characteristics and overall hormonal balance.
In contrast, the adrenal medulla produces catecholamines, mainly adrenaline (epinephrine) and noradrenaline (norepinephrine). These are often called “fight-or-flight” hormones because they prepare the body to respond quickly to stress or danger. They increase heart rate and the force of heart contractions, improve blood flow to the brain and muscles, and promote the release of glucose for immediate energy. They also cause constriction of blood vessels, helping to maintain blood pressure during stressful situations. These hormones act rapidly, allowing the body to react within seconds.
Overall, adrenal hormones work together to ensure that the body can respond effectively to both everyday demands and sudden stress. While steroid hormones provide long-term regulation of metabolism, immunity, and fluid balance, catecholamines enable quick, short-term responses. This coordinated action is essential for maintaining health, stability, and survival.
FATE OF CORTICOSTEROIDS:
Corticosteroids, including glucocorticoids like cortisol and mineralocorticoids like aldosterone, are essential hormones produced by the adrenal cortex. After being released into the bloodstream, they undergo a series of processes involving transport, metabolism, and excretion, which together determine their overall effects in the body.
Once secreted, most corticosteroids circulate in the blood bound to plasma proteins. Cortisol, for example, is largely transported by a specific carrier protein called corticosteroid-binding globulin (CBG), while a smaller portion remains free and biologically active. Only the free form of the hormone can enter cells and exert its effects. This binding also acts as a reservoir, helping to maintain stable hormone levels in circulation.
Corticosteroids are primarily metabolized in the liver. Here, they are converted into inactive forms through enzymatic reactions such as reduction and conjugation. These processes make the hormones more water-soluble, allowing them to be more easily eliminated from the body. Some metabolism also occurs in the kidneys and other tissues, but the liver remains the main site.
After metabolism, the inactive metabolites are excreted mainly through the kidneys in urine. A smaller amount may also be eliminated through bile into the feces. The rate at which corticosteroids are cleared from the body depends on their half-life, which varies among different hormones. For example, cortisol has a moderate half-life, allowing it to exert sustained effects, while aldosterone is cleared more rapidly, reflecting its role in short-term regulation of electrolyte balance.
The regulation of corticosteroid levels is closely controlled by feedback mechanisms. Cortisol secretion is regulated by the hypothalamus–pituitary–adrenal (HPA) axis, where increased cortisol levels inhibit further release of ACTH, thereby maintaining hormonal balance. Aldosterone, on the other hand, is mainly regulated by electrolyte levels and the renin–angiotensin system rather than direct hormonal feedback.
Overall, the fate of corticosteroids involves a carefully balanced cycle of circulation, action, metabolism, and excretion. This ensures that their powerful effects on metabolism, fluid balance, and stress response are precisely controlled and do not become excessive or prolonged.
DISORDERS: SIGNS & SYMPTOMS:
The adrenal glands play a vital role in maintaining hormonal balance in the body. When these glands produce too much or too little of certain hormones, it can lead to a range of disorders affecting metabolism, blood pressure, stress response, and overall health. These conditions may arise from tumors, genetic defects, autoimmune diseases, or long-term medication use.
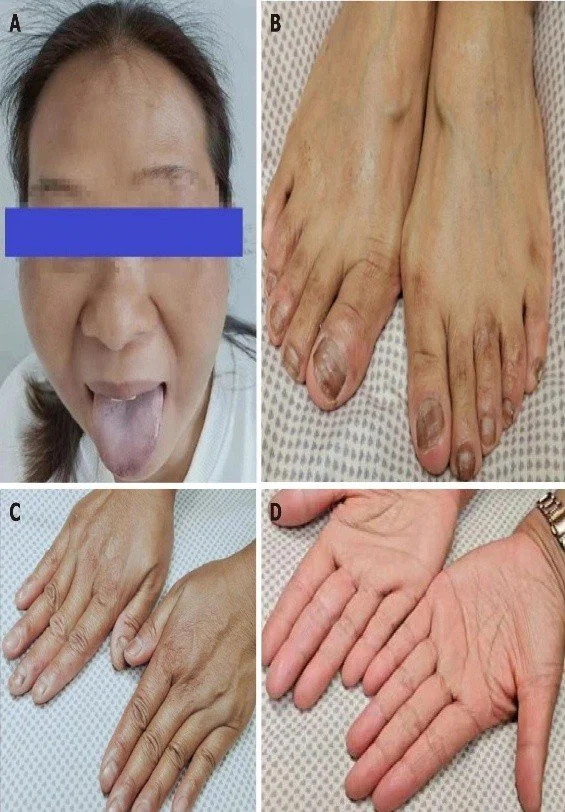
One of the most important disorders is Addison’s disease, also known as adrenal insufficiency. In this condition, the adrenal cortex fails to produce enough cortisol and aldosterone. As a result, individuals often experience chronic fatigue, muscle weakness, low blood pressure, dehydration, and weight loss. A characteristic feature is darkening of the skin (hyperpigmentation), caused by increased ACTH levels. Patients may also have nausea, vomiting, and a reduced ability to handle stress. In severe cases, an adrenal crisis can occur, leading to sudden collapse and requiring immediate medical attention.(fig:3)
In contrast, Cushing syndrome results from excessive production of cortisol. This may be due to tumors of the adrenal gland, excessive ACTH secretion, or prolonged use of steroid medications. The condition is characterized by abnormal fat distribution, leading to features such as a rounded “moon face,” fat accumulation in the abdomen (pot belly), and a “buffalo hump” on the back of the neck. Other common symptoms include thinning of the skin, purple stretch marks, muscle weakness, osteoporosis, high blood pressure, and increased blood glucose levels. Patients are also more prone to infections and show delayed wound healing due to suppressed immune function.(Fig:4)
Another important disorder is hyperaldosteronism, in which excess aldosterone is produced. This condition causes increased retention of sodium and water, leading to high blood pressure. At the same time, excessive loss of potassium results in symptoms such as muscle weakness, fatigue, and irregular heart rhythms. In severe cases, metabolic alkalosis may develop due to increased loss of hydrogen ions.
Adrenogenital syndrome occurs when the adrenal glands produce excessive androgens. In females, this leads to masculinization, including deepening of the voice, increased body hair, and enlargement of the clitoris. Men may show signs of feminization if there is abnormal estrogen production, such as breast enlargement and reduced sexual function. These changes reflect the imbalance in sex hormone production.
Congenital adrenal hyperplasia (CAH) is a genetic disorder in which enzyme deficiencies impair cortisol production. This leads to increased ACTH stimulation and enlargement of the adrenal glands. As a result, excess androgens are produced, causing early sexual development in boys and masculinization in girls. In some cases, affected individuals may appear normal at birth but develop symptoms later in childhood.
In addition to adrenal disorders, diabetes mellitus is another major endocrine condition that may be related to hormonal imbalance. It is characterized by high blood glucose levels due to problems with insulin production or action. Common symptoms include excessive urination (polyuria), increased thirst (polydipsia), increased hunger (polyphagia), fatigue, and weight loss. Severe cases may lead to complications such as ketoacidosis, dehydration, and even coma. Long-term complications include damage to blood vessels, nerves, kidneys, and eyes.
Overall, adrenal and endocrine disorders can significantly affect multiple systems in the body. Early recognition of symptoms such as fatigue, abnormal weight changes, blood pressure abnormalities, and metabolic disturbances is essential for timely diagnosis and treatment. Proper management can help prevent complications and improve quality of life.

DIAGNOSIS AND TREATMENT:
Endocrine disorders such as diabetes mellitus, Cushins syndrome, and Addison’s disease require careful diagnosis and targeted treatment, as they involve complex hormonal imbalances that affect multiple body systems. Early identification through appropriate tests, followed by proper management, plays a key role in preventing complications and improving quality of life.
Diabetes mellitus is diagnosed mainly by evaluating blood glucose levels. This includes measuring fasting blood glucose, postprandial blood glucose, and performing a glucose tolerance test to assess how the body processes sugar. Another important test is glycated hemoglobin (HbA1c), which provides an overview of long-term blood glucose control and is especially useful for monitoring patients over time. Abnormal results, such as elevated fasting glucose or reduced glucose tolerance, may indicate early stages like pre-diabetes.
The treatment of diabetes depends on its type. In Type I diabetes, where the body is unable to produce insulin, treatment involves regular administration of insulin through injections, as it cannot be taken orally due to digestion in the gastrointestinal tract. In Type II diabetes, treatment typically begins with lifestyle modifications and oral medications. These drugs may work by stimulating insulin secretion, improving the body’s response to insulin, or slowing down carbohydrate absorption in the intestine. In more severe or long-standing cases, insulin therapy may be added to achieve better control of blood glucose levels.
Cushing syndrome is usually identified through a combination of clinical features and laboratory findings. Physical signs such as abnormal fat distribution often raise suspicion, which is then confirmed by measuring cortisol levels in the blood and analyzing urine for steroid metabolites. Treatment depends on the underlying cause and may include medications to reduce cortisol production, surgical removal of tumors in the adrenal or pituitary glands, or radiation therapy. In some cases, a condition known as Nelson syndrome may develop after removal of the adrenal glands, where a pituitary tumor produces excess ACTH, leading to symptoms like headaches and visual disturbances. This condition is managed through surgery or radiation therapy.
Addison’s disease, on the other hand, is diagnosed by detecting low levels of cortisol and aldosterone in the blood, along with reduced steroid excretion in urine. These findings confirm adrenal insufficiency and help guide further treatment, which typically involves hormone replacement therapy to restore normal physiological function.
In summary, the diagnosis of endocrine disorders relies on a combination of clinical evaluation and laboratory testing, particularly hormone level assessment. Treatment approaches are tailored to the specific disorder and aim to restore hormonal balance, whether through medication, hormone replacement, or surgical intervention. With timely diagnosis and appropriate care, most of these conditions can be effectively managed.
CONCLUSION:
The adrenal glands may be tiny, but they play an essential part in keeping the body balanced and resilient. They have the ability to coordinate various hormones secreted by the cortex and medulla to ensure proper functioning of the metabolism rate, electrolyte levels, blood pressure, and reaction to various types of stressful stimuli.The article explains how the various hormones work within our bodies. It shows how these hormones are synthesized, their activities, as well as how they get metabolized. The production and removal of hormones from the body need to be controlled in order to avoid any kind of malfunction.Adrenal disorders include Addison's Disease, Cushing Syndrome, and Hyperaldosteronism. Knowledge about these kinds of disorders helps us appreciate why we need the correct hormone regulation within our bodies. Imbalances within our bodies can affect many systems and result in many adverse effects.
In summary, the adrenal glands play a crucial part in ensuring survival and resilience in people's lives. We need to understand the importance of these glands to ensure we keep our bodies healthy and strong.
REFERENCE:
1)Medical Physiology Sixth Edition K Sembulingam
2)Guyton and Hall Textbook of Medical Physiology 14 TH EDITION
3) GK PAL Comprehensive Textbook of Medical Physiology volume 1
4) CV Pharmacology | Norepinephrine, Epinephrine and Acetylcholine - Synthesis, Release and Metabolism https://share.google/s1YpHV2uKFbQ0rVOx
5)Fight-or-flight response - Wikipedia https://share.google/qC7WqsBSeCuDgZVQ1
6)Adrenaline - Wikipedia https://share.google/ktRBMnlMwooPQ822u
7)Adrenal Gland: What It Is, Function, Symptoms & Disorders https://share.google/U5YxQoFNSLQwQQaj2