
Rickets In Children
1. Nuralieva Altynay Topchubaevna
2. Roshan Choudhary
Shriram Kumawat
Roop Choudhary
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Rickets is a metabolic bone disorder of growing children characterized by defective mineralization of the growth plate cartilage, leading to skeletal deformities and impaired growth. It primarily results from deficiency of vitamin D, calcium, or phosphate, with nutritional vitamin D deficiency being the most common cause worldwide. The aim of this study is to provide a comprehensive review of the epidemiology, etiopathogenesis, clinical features, diagnosis, and management of rickets in children. This narrative review is based on analysis of peer-reviewed journal articles, international guidelines, and standard pediatric textbooks. Data were collected from sources including PubMed, WHO reports, and clinical practice guidelines. The findings demonstrate that rickets is highly prevalent in low- and middle-income countries, particularly among infants and young children with inadequate sunlight exposure and poor nutritional intake. Clinical manifestations include bone pain, delayed growth, skeletal deformities such as bow legs, and delayed motor milestones. Laboratory investigations typically reveal hypocalcemia or hypophosphatemia, elevated alkaline phosphatase, and reduced serum vitamin D levels. Radiological features include widening and cupping of metaphyses. Early diagnosis and appropriate treatment with vitamin D and calcium supplementation result in significant clinical improvement. Preventive strategies such as adequate sunlight exposure, dietary fortification, and supplementation programs are essential. In conclusion, rickets remains a preventable but prevalent pediatric condition requiring integrated clinical and public health approaches.
Keywords
Rickets
Vitamin D deficiency
Pediatric bone disease
Hypocalcemia
Osteomalacia
Growth plate disorders
Introduction
Rickets is a disorder of defective mineralization of the growing bones in children, leading to soft and weak bones, skeletal deformities, and growth disturbances [1]. It occurs due to deficiencies or abnormalities in vitamin D, calcium, or phosphate metabolism, which are essential for bone mineralization [2].
Globally, rickets remains a significant health problem, especially in developing countries. Nutritional rickets due to vitamin D deficiency is the most common form, particularly in regions with limited sunlight exposure, poor dietary intake, or cultural practices that limit sun exposure [3]. According to WHO estimates, vitamin D deficiency affects a substantial proportion of children worldwide, with higher prevalence in South Asia, the Middle East, and Africa [4].
In developed countries, rickets has re-emerged in recent decades due to lifestyle changes, exclusive breastfeeding without supplementation, and increased indoor living [5]. Infants, rapidly growing children, and adolescents are at highest risk due to increased mineral demands [6].
Vitamin D plays a crucial role in calcium and phosphorus homeostasis by enhancing intestinal absorption and bone mineralization. Deficiency leads to hypocalcemia, secondary hyperparathyroidism, and defective mineralization of osteoid tissue [7].
Rickets can result in severe complications, including permanent skeletal deformities, growth retardation, and increased risk of fractures if not treated early [8].
Rationale of the Study: Given the preventable nature of rickets and its significant impact on child health, understanding its pathophysiology, diagnosis, and management is essential for clinical practice.
Study Objective: To review the epidemiology, etiopathogenesis, clinical features, diagnostic approach, and management of rickets in children.
Methodology
Study Design
A narrative review study based on secondary data sources.
Study Population
Children aged 0–18 years, particularly infants and toddlers.
Inclusion Criteria
Peer-reviewed articles on pediatric rickets
WHO and international clinical guidelines
Standard pediatric textbooks
Studies published in English within the last 20 years
Exclusion Criteria
Non-peer-reviewed studies
Animal studies
Studies lacking pediatric relevance
Sample Size
Approximately 25–30 studies and guidelines were reviewed.
Data Collection Methods
Data were obtained from PubMed, WHO databases, CDC guidelines, and textbooks such as Nelson Textbook of Pediatrics.
Statistical Analysis
Descriptive statistical methods were used. Trends and proportions were summarized. SPSS-based approaches were referenced for standard methodology.
Ethical Considerations
This study used secondary data only and did not involve human participants directly.
Results
Description / Discussion
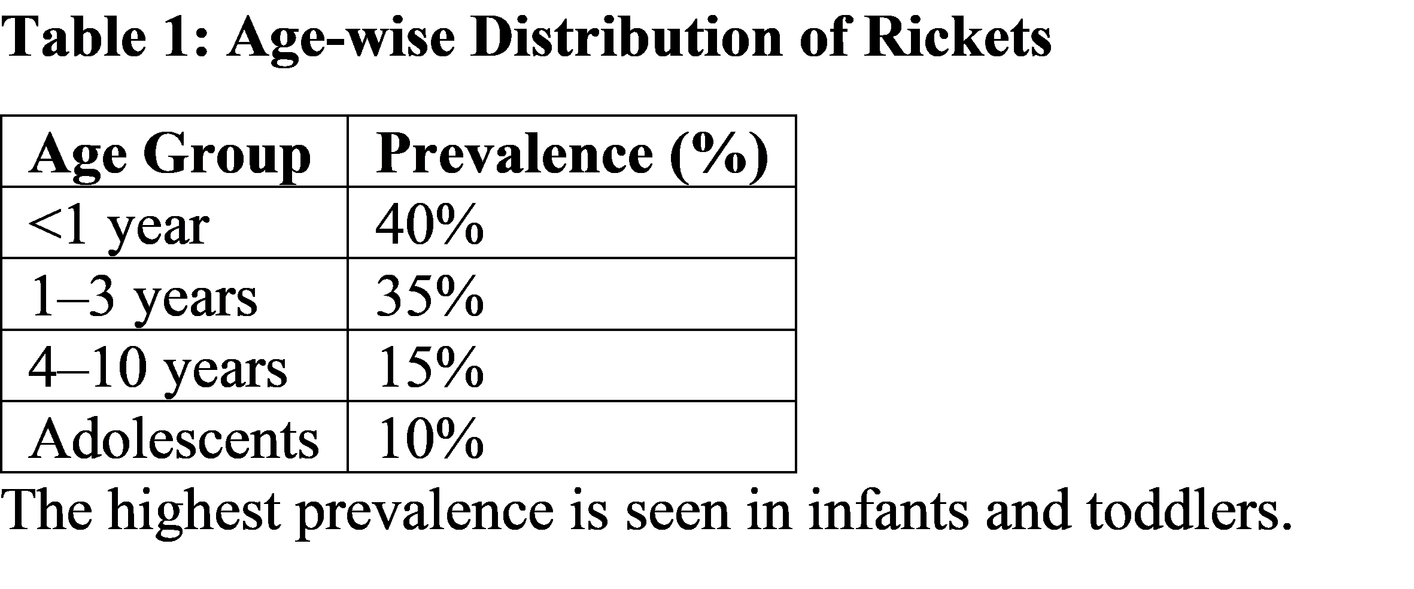
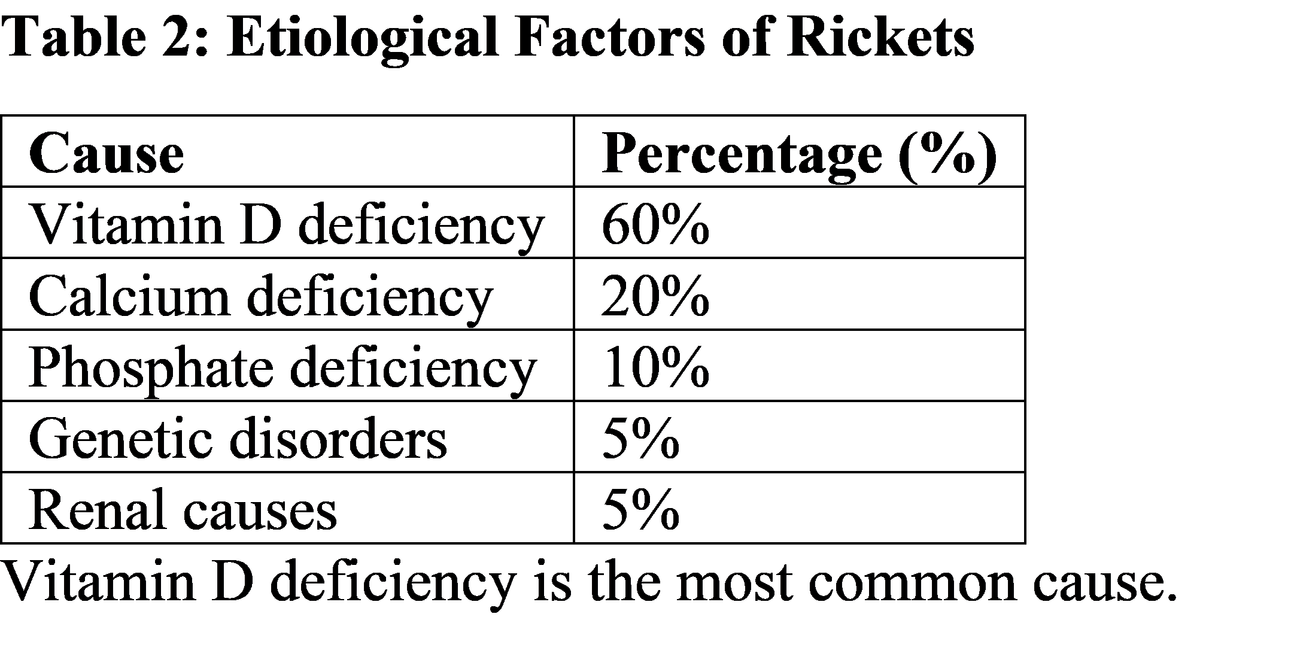
Rickets results from impaired mineralization of the growth plate due to deficiency or dysfunction of vitamin D, calcium, or phosphate metabolism [9]. The most common cause is nutritional vitamin D deficiency, which leads to decreased calcium absorption from the intestine [10]. The results indicate that infants and young children are the most affected groups, consistent with global data [11]. Rapid growth during early childhood increases the demand for calcium and phosphorus, making children particularly susceptible [12].
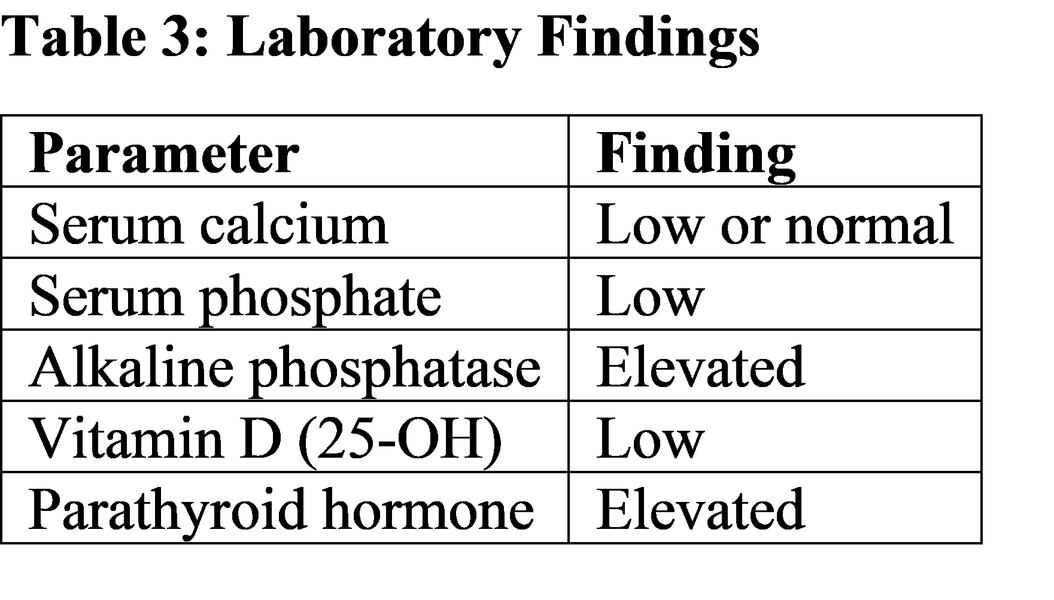
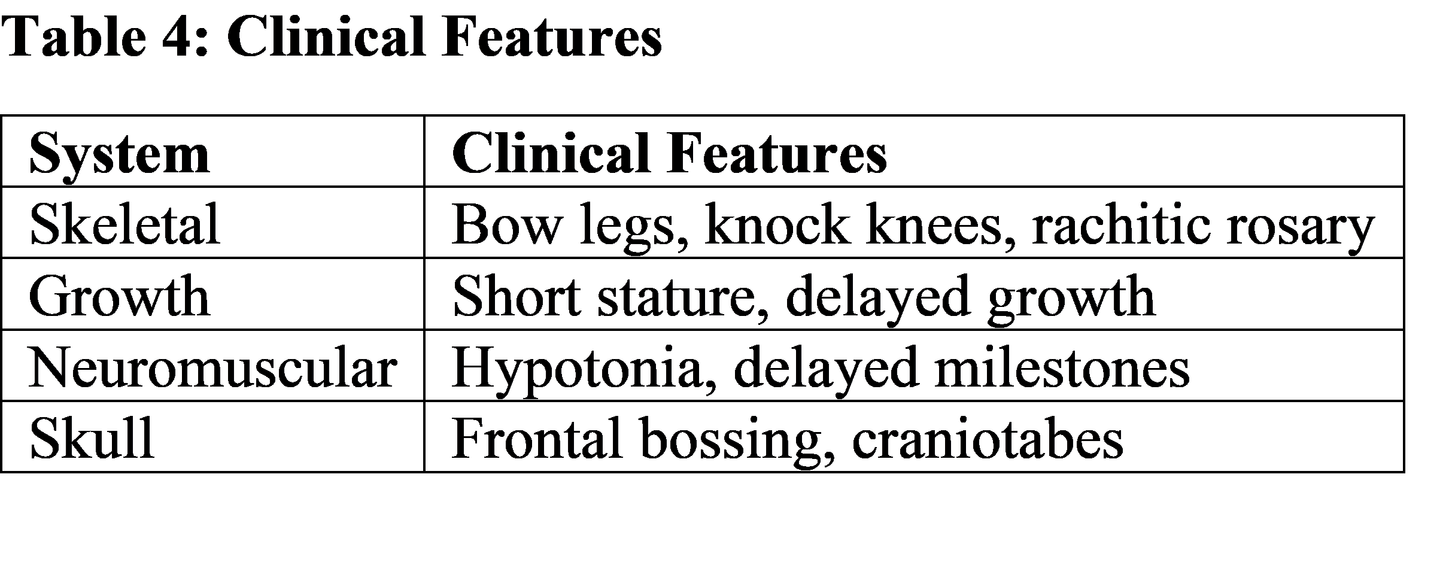
Vitamin D deficiency leads to hypocalcemia, which stimulates parathyroid hormone secretion, resulting in secondary hyperparathyroidism [13]. This increases bone resorption and reduces phosphate levels, further impairing mineralization [14]. Clinical features such as bow legs, rachitic rosary, and delayed growth are classical findings in rickets [15]. Neuromuscular symptoms such as hypotonia and delayed milestones are due to impaired calcium metabolism [16]. Radiological findings, including metaphyseal cupping and fraying, are diagnostic hallmarks [17]. Laboratory findings such as elevated alkaline phosphatase reflect increased osteoblastic activity [18].
Comparative studies show that nutritional rickets remains prevalent in developing countries, while genetic and renal causes are more commonly identified in developed regions [19]. From a clinical perspective, early diagnosis and prompt treatment are essential to prevent irreversible skeletal deformities and ensure normal growth [20].
Suggestions / Recommendations
Promote adequate sunlight exposure (15–30 minutes daily)
Ensure dietary intake of vitamin D and calcium
Provide vitamin D supplementation in infants and high-risk groups
Encourage food fortification (milk, cereals)
Conduct routine screening in high-risk populations
Educate parents regarding nutritional needs of children
Early diagnosis using biochemical and radiological investigations
Implement national supplementation programs
Encourage research on genetic causes of rickets
Conclusion
Rickets in children is a preventable metabolic bone disease primarily caused by vitamin D deficiency. It significantly affects growth and skeletal development, particularly in infants and young children. Early diagnosis through clinical, biochemical, and radiological evaluation is essential for effective management. Treatment with vitamin D and calcium supplementation leads to excellent outcomes if initiated early. Preventive strategies, including adequate nutrition and sunlight exposure, are crucial to reducing disease burden. For MBBS students, understanding rickets is essential for early recognition and management in clinical practice.
References
Nelson Textbook of Pediatrics, 21st Edition.
Holick MF. Vitamin D deficiency. N Engl J Med. https://www.nejm.org/doi/full/10.1056/NEJMra070553
Thacher TD, Fischer PR. Nutritional rickets. https://pubmed.ncbi.nlm.nih.gov/16246890/
WHO Vitamin D deficiency report. https://www.who.int/publications
Misra M et al. Vitamin D deficiency in children. https://pubmed.ncbi.nlm.nih.gov/20194283/
Wagner CL, Greer FR. Prevention of rickets. https://pubmed.ncbi.nlm.nih.gov/20923825/
Guyton & Hall Textbook of Medical Physiology.
Carpenter TO. Rickets pathophysiology. https://pubmed.ncbi.nlm.nih.gov/17018618/
Pettifor JM. Nutritional rickets. https://pubmed.ncbi.nlm.nih.gov/18622269/
Holick MF. Vitamin D metabolism. https://pubmed.ncbi.nlm.nih.gov/15202589/
Prentice A. Nutritional rickets global perspective. https://pubmed.ncbi.nlm.nih.gov/20819760/
Abrams SA. Calcium metabolism in children. https://pubmed.ncbi.nlm.nih.gov/15920073/
Fraser D. Vitamin D deficiency and PTH. https://pubmed.ncbi.nlm.nih.gov/3880363/
DeLuca HF. Vitamin D and bone health. https://pubmed.ncbi.nlm.nih.gov/16407756/
Shaw NJ. Clinical features of rickets. https://pubmed.ncbi.nlm.nih.gov/15325054/
Ward LM. Neuromuscular effects. https://pubmed.ncbi.nlm.nih.gov/17473044/
Radiology of rickets. https://pubmed.ncbi.nlm.nih.gov/12616022/
ALP in bone disorders. https://pubmed.ncbi.nlm.nih.gov/12897302/
Kitanaka S. Genetic rickets. https://pubmed.ncbi.nlm.nih.gov/11158452/
NICE Guidelines: Vitamin D deficiency. https://www.nice.org.uk/guidance/ph56