
Iron Deficiency Anemia In Children
1. Nuralieva Altynay Topchubaevna
2. Ariyanachi Nagarajan Santhi Arivusudar
Sahana Arumugam
Gunji Raja
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Iron deficiency anemia (IDA) in children is a major global public health concern, particularly affecting infants, preschool-aged children, and adolescents. It results from inadequate iron availability for hemoglobin synthesis, leading to impaired oxygen transport and systemic complications. The aim of this study is to provide a comprehensive academic review of the epidemiology, etiopathogenesis, clinical features, diagnosis, and management of IDA in pediatric populations. This study is based on a narrative review of peer-reviewed literature, standard pediatric textbooks, and international guidelines, including those from WHO and CDC. The findings demonstrate that IDA in children is primarily caused by inadequate dietary intake, increased physiological demands during growth, and chronic blood loss or infections. Clinical manifestations include pallor, fatigue, irritability, delayed cognitive development, and poor growth. Laboratory investigations typically reveal microcytic hypochromic anemia, low serum ferritin, and elevated total iron-binding capacity. Early detection and appropriate iron supplementation significantly improve outcomes and prevent long-term neurodevelopmental deficits. Preventive strategies such as nutritional education, iron fortification, and routine screening in high-risk populations are essential. In conclusion, IDA in children is a preventable and treatable condition, but it continues to impose a substantial burden globally, necessitating integrated clinical and public health interventions.
Keywords
Iron deficiency anemia, Pediatric anemia, Microcytic hypochromic anemia, Serum ferritin, nutritional deficiency, Child health
Introduction
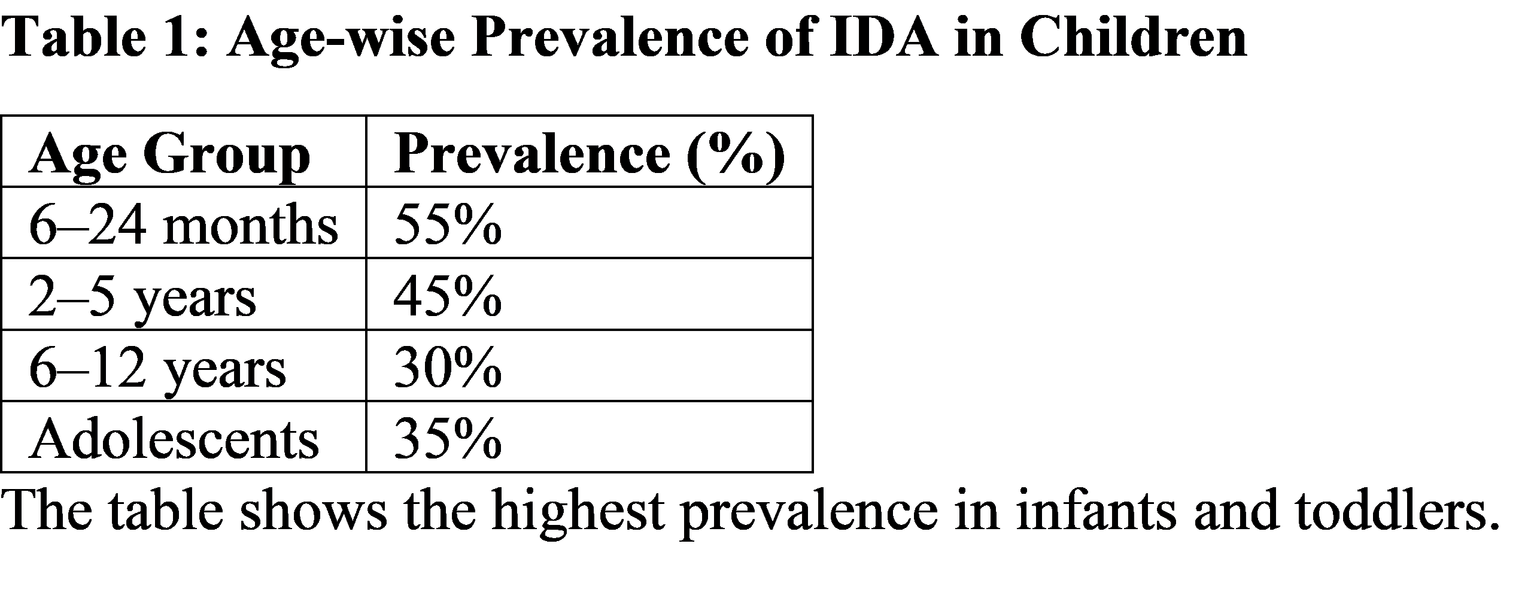
Iron deficiency anemia (IDA) is the most common nutritional deficiency disorder affecting children worldwide and is characterized by reduced hemoglobin levels due to insufficient iron availability [1]. It is particularly prevalent in infants, young children, and adolescents due to increased iron requirements during periods of rapid growth [2].
Globally, anemia affects approximately 42% of children under five years of age, with iron deficiency accounting for nearly half of these cases [3]. The burden is especially high in low- and middle-income countries, including regions of Asia and Africa, where malnutrition, parasitic infections, and limited healthcare access are common [4]. In South Asia, prevalence rates in children may exceed 60% in certain populations [5].
Iron is essential for hemoglobin synthesis, myelination, neurotransmitter production, and cellular metabolism. Deficiency during early childhood can result in irreversible cognitive and behavioral impairments, making it a critical pediatric health issue [6]. Additionally, IDA is associated with increased susceptibility to infections and impaired physical growth [7].
Despite its high prevalence, IDA often remains underdiagnosed due to nonspecific clinical symptoms and limited access to diagnostic facilities in resource-poor settings [8].
Rationale of the Study: Given the significant impact of IDA on child growth, development, and long-term health outcomes, a comprehensive understanding of its etiology, diagnosis, and management is essential for MBBS students and healthcare professionals.
Study Objective: To review the epidemiology, pathophysiology, clinical manifestations, diagnostic approach, and management strategies of iron deficiency anemia in children.
Methodology
Study Design
A narrative review study based on secondary data sources including clinical studies, guidelines, and textbooks.
Study Population
Children aged 6 months to 18 years, with emphasis on high-risk groups such as infants, toddlers, and adolescents.
Inclusion Criteria
Peer-reviewed articles on pediatric iron deficiency anemia
WHO, CDC, and pediatric guidelines
Studies published in English within the last 20 years
Standard pediatric and medical textbooks
Exclusion Criteria
Non-peer-reviewed sources
Studies lacking pediatric-specific data
Animal-based studies
Sample Size
Approximately 25–30 studies and guidelines were included in the review.
Data Collection Methods
Data were collected from PubMed, WHO databases, CDC guidelines, and textbooks such as Nelson Textbook of Pediatrics and Harrison’s Principles of Internal Medicine.
Statistical Analysis
Descriptive statistical analysis was performed. Data trends were summarized using percentages and mean values. SPSS methodology was referenced for standard data interpretation.
Ethical Considerations
No direct patient involvement was included. Ethical guidelines for secondary data usage were followed.
Results
Description / Discussion
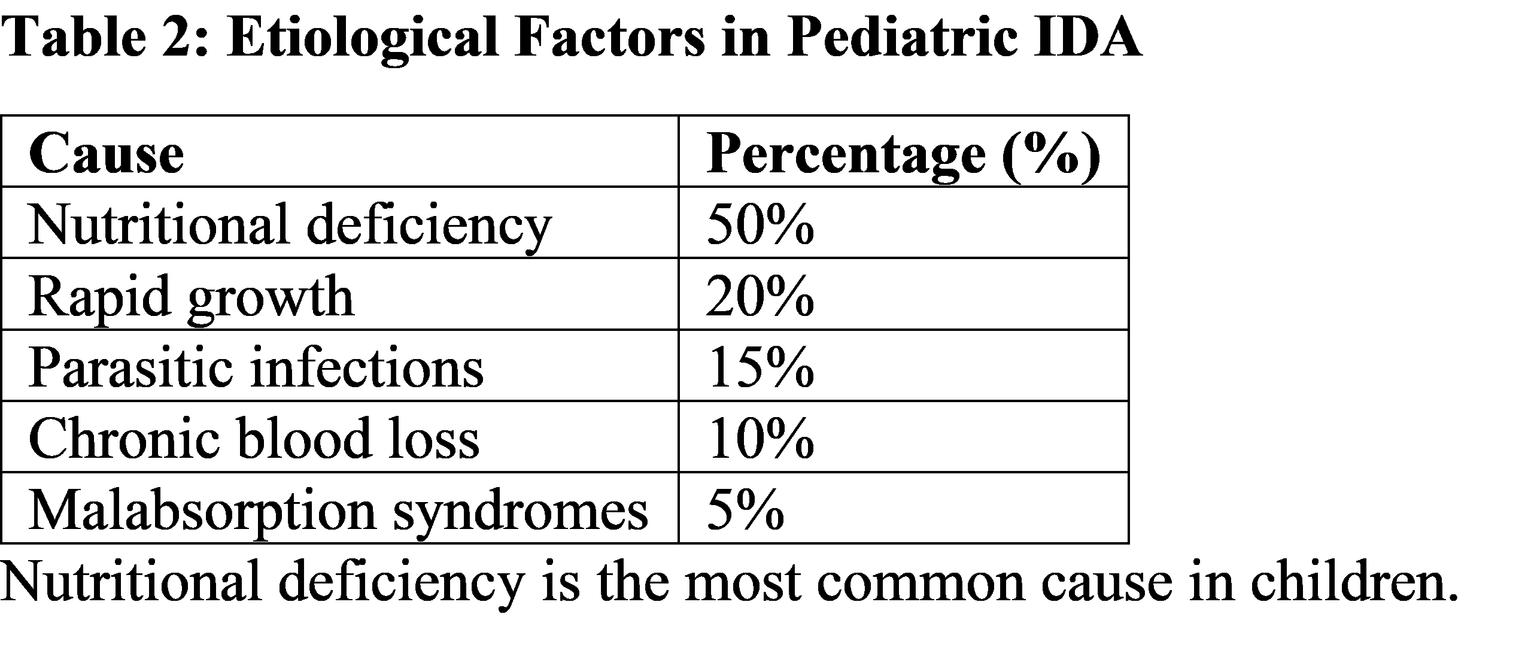
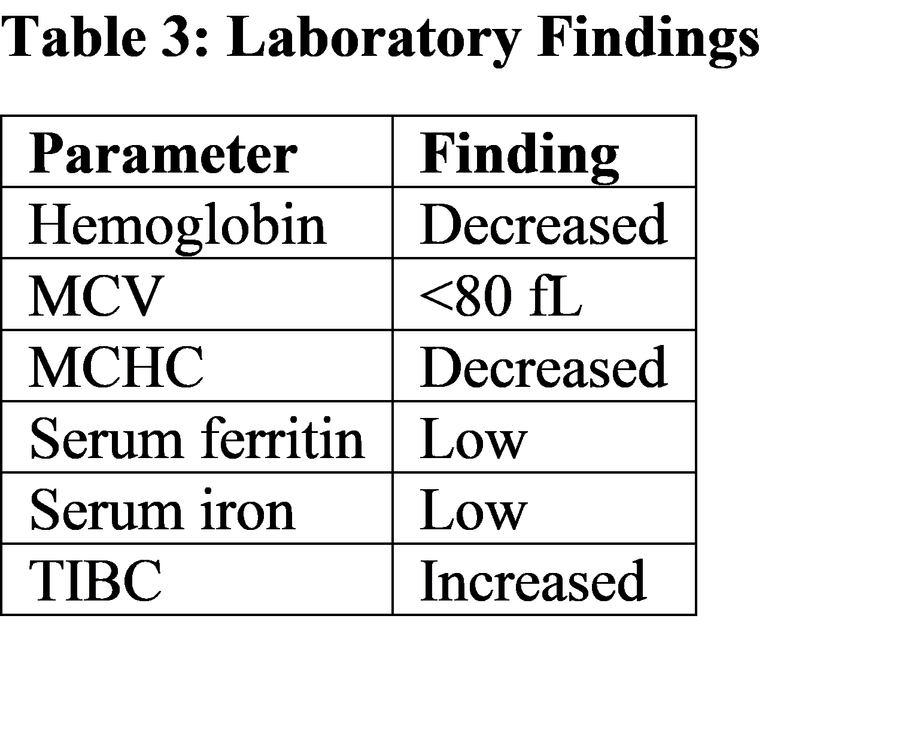
Iron deficiency anemia in children develops due to a negative iron balance resulting from inadequate intake, increased demand, or excessive loss [9]. Infants are particularly vulnerable due to depletion of iron stores acquired during fetal life by 4–6 months of age [10]. The results of this study indicate that nutritional deficiency is the leading cause of IDA in children, consistent with global literature [11]. Diets low in bioavailable iron, such as predominantly cereal-based diets, contribute significantly to this condition [12]. Rapid growth during infancy and adolescence increases iron requirements, often exceeding dietary intake [13]. Additionally, parasitic infections such as hookworm and malaria contribute to chronic blood loss and iron depletion [14]. Laboratory findings such as low serum ferritin and elevated TIBC are consistent diagnostic markers, with serum ferritin being the most sensitive indicator of iron stores [15]. However, ferritin may be elevated in inflammatory conditions, necessitating careful interpretation [16].
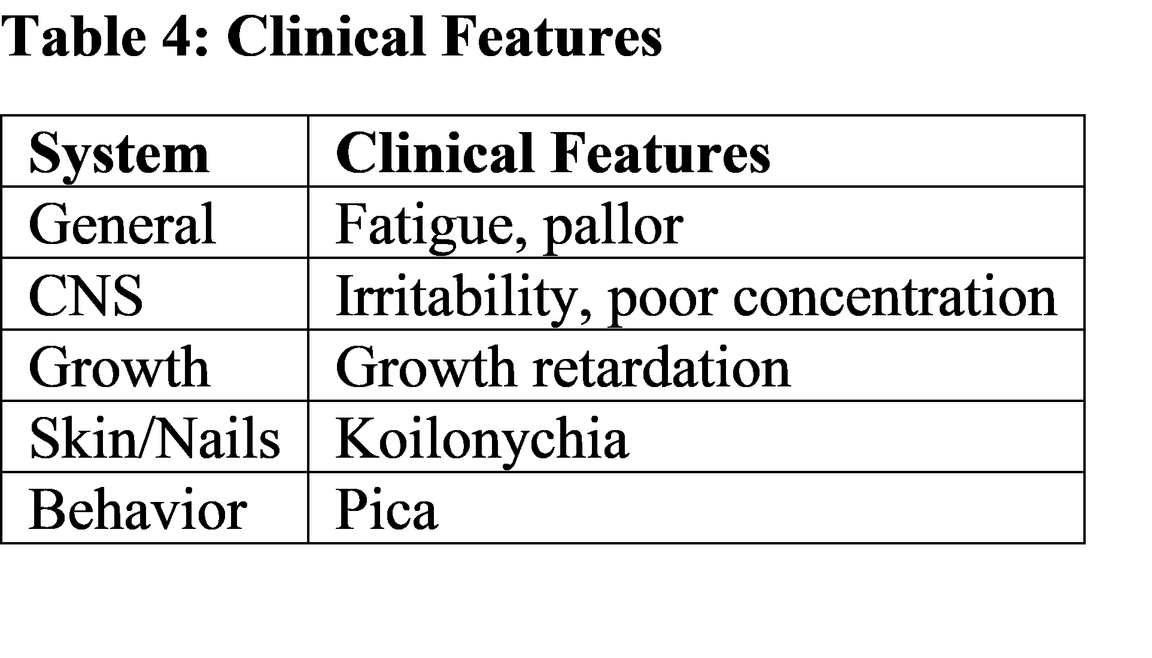
Clinical manifestations in children differ from adults, with prominent neurodevelopmental effects. Iron deficiency impairs myelination and neurotransmitter synthesis, leading to cognitive and behavioral disturbances [17]. Studies have shown that early-life IDA is associated with long-term deficits in attention, learning, and memory [18]. Comparative studies reveal similar patterns globally, although developed countries have lower prevalence due to better nutrition and supplementation programs [19]. From a clinical perspective, early diagnosis and treatment are essential to prevent irreversible neurodevelopmental damage and improve quality of life [20].
Suggestions / Recommendations
Promote exclusive breastfeeding for the first 6 months followed by iron-rich complementary feeding
Encourage intake of iron-rich foods (meat, green leafy vegetables, fortified cereals)
Routine screening for anemia in high-risk age groups
Provide prophylactic iron supplementation in infants and adolescents
Implement deworming programs in endemic areas
Strengthen public health education regarding nutrition
Use serum ferritin and complete blood count for early diagnosis
Promote food fortification strategies (iron-fortified flour, cereals)
Conduct longitudinal studies on cognitive outcomes of IDA
Conclusion
Iron deficiency anemia in children is a widespread and preventable condition with significant implications for growth and neurodevelopment. It is primarily caused by nutritional deficiency and increased physiological demands during growth. Early detection through appropriate laboratory investigations and timely treatment with iron supplementation are essential. Preventive strategies including dietary modification, supplementation, and public health interventions are crucial to reduce disease burden. For MBBS students, a clear understanding of pediatric IDA is vital for effective clinical management and prevention.
Reference
Nelson Textbook of Pediatrics, 21st Edition.
Kliegman RM et al. Pediatric anemia overview. https://www.ncbi.nlm.nih.gov/books/NBK537332/
WHO. Global prevalence of anemia. https://www.who.int/data/nutrition/nlis/info/anaemia
Balarajan Y et al. Anaemia in low-income countries. https://pubmed.ncbi.nlm.nih.gov/23507020/
UNICEF Nutrition Report. https://data.unicef.org/topic/nutrition/
Lozoff B et al. Iron deficiency and brain development. https://pubmed.ncbi.nlm.nih.gov/22332096/
WHO Child Health Guidelines. https://www.who.int/health-topics/child-health
CDC Iron Deficiency in Children. https://www.cdc.gov/nutrition/infantandtoddlernutrition/iron.html
Andrews NC. Iron metabolism. https://pubmed.ncbi.nlm.nih.gov/14687550/
Baker RD, Greer FR. Diagnosis and prevention of IDA in infants. https://pubmed.ncbi.nlm.nih.gov/20923825/
Camaschella C. Iron deficiency anemia. https://www.nejm.org/doi/full/10.1056/NEJMra1401038
Hurrell R, Egli I. Iron bioavailability. https://pubmed.ncbi.nlm.nih.gov/19087456/
WHO Complementary Feeding Guidelines. https://www.who.int/publications/i/item/924154614X
Hotez PJ et al. Hookworm infection. https://pubmed.ncbi.nlm.nih.gov/15489334/
WHO Serum Ferritin Guidelines. https://www.who.int/publications/i/item/9789240000124
Weiss G, Goodnough LT. Anemia of chronic disease. https://pubmed.ncbi.nlm.nih.gov/16034428/
Beard JL. Iron deficiency and neural development. https://pubmed.ncbi.nlm.nih.gov/12612133/
Grantham-McGregor S, Ani C. Effects on cognition. https://pubmed.ncbi.nlm.nih.gov/11217994/
Kassebaum NJ. Global anemia burden. https://pubmed.ncbi.nlm.nih.gov/24297872/
NICE Guidelines: Anemia management. https://www.nice.org.uk/guidance/ng8