
Bronchitis and Bronchiolitis in Children
1. Nuralieva Altynay Topchubaevna
2. Shravan Sarvesh Jaiswal
Rohit Tanwar
Rakibul Hossain Sarkar
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Bronchitis and bronchiolitis are common respiratory tract infections in children, contributing significantly to pediatric morbidity worldwide. Bronchitis primarily involves inflammation of the larger airways, whereas bronchiolitis affects the smaller bronchioles and is most commonly seen in infants. The aim of this study is to provide a comprehensive review of the epidemiology, etiopathogenesis, clinical features, diagnosis, and management of bronchitis and bronchiolitis in children. This narrative review is based on analysis of peer-reviewed articles, pediatric textbooks, and international guidelines, including those from WHO and CDC. The findings indicate that viral infections, particularly respiratory syncytial virus (RSV), are the leading cause of bronchiolitis, while bronchitis may be caused by both viral and bacterial agents. Clinical manifestations include cough, wheezing, respiratory distress, and feeding difficulties in infants. Laboratory findings are often nonspecific, and diagnosis is primarily clinical. Management is largely supportive, including oxygen therapy, hydration, and monitoring, with limited roles for pharmacological interventions. Preventive strategies such as vaccination, breastfeeding, and infection control measures are crucial in reducing disease burden. In conclusion, bronchitis and bronchiolitis remain significant pediatric health concerns, especially in infants, requiring early recognition and appropriate management to prevent complications and hospitalization.
Keywords
Bronchiolitis
Bronchitis
Respiratory syncytial virus
Pediatric respiratory infections
Wheezing
Lower respiratory tract infection
Introduction
Bronchitis and bronchiolitis are inflammatory conditions of the lower respiratory tract commonly affecting children. Bronchitis refers to inflammation of the bronchial tubes, while bronchiolitis involves inflammation of the smaller airways (bronchioles), predominantly affecting infants under two years of age [1].
Globally, bronchiolitis is one of the leading causes of hospitalization in infants, especially during the winter season. It is estimated that nearly all children are infected with respiratory syncytial virus (RSV) by the age of two years, with a subset developing severe bronchiolitis [2]. According to WHO, acute lower respiratory infections, including bronchiolitis, account for a significant proportion of child mortality, particularly in developing countries [3].
Bronchitis in children is often viral in origin but may occasionally be bacterial. It presents as part of a spectrum of respiratory infections and is commonly associated with upper respiratory tract infections [4].
Risk factors for severe disease include prematurity, low birth weight, malnutrition, lack of breastfeeding, and exposure to environmental pollutants such as tobacco smoke [5].
The pathophysiology involves airway inflammation, mucosal edema, increased mucus production, and airway obstruction, leading to impaired ventilation and gas exchange [6].
Rationale of the Study: Given the high prevalence and potential complications of bronchitis and bronchiolitis in children, a detailed understanding is essential for effective diagnosis and management.
Study Objective: To review the epidemiology, etiopathogenesis, clinical features, diagnostic approach, and management of bronchitis and bronchiolitis in children.
Methodology
Study Design
A narrative review study based on secondary data sources.
Study Population
Children aged 0–18 years, with emphasis on infants and young children.
Inclusion Criteria
Peer-reviewed articles on pediatric bronchitis and bronchiolitis
WHO, CDC, and NICE guidelines
Standard pediatric textbooks
Studies published in English within the last 20 years
Exclusion Criteria
Non-peer-reviewed sources
Studies lacking pediatric-specific data
Animal-based studies
Sample Size
Approximately 25–30 studies and guidelines were reviewed.
Data Collection Methods
Data were collected from PubMed, WHO databases, CDC guidelines, and textbooks such as Nelson Textbook of Pediatrics.
Statistical Analysis
Descriptive statistical analysis was performed. Trends and proportions were summarized. SPSS methodology was referenced for standard analysis.
Ethical Considerations
No direct patient involvement; ethical standards for secondary data usage were followed.
Results
Description / Discussion
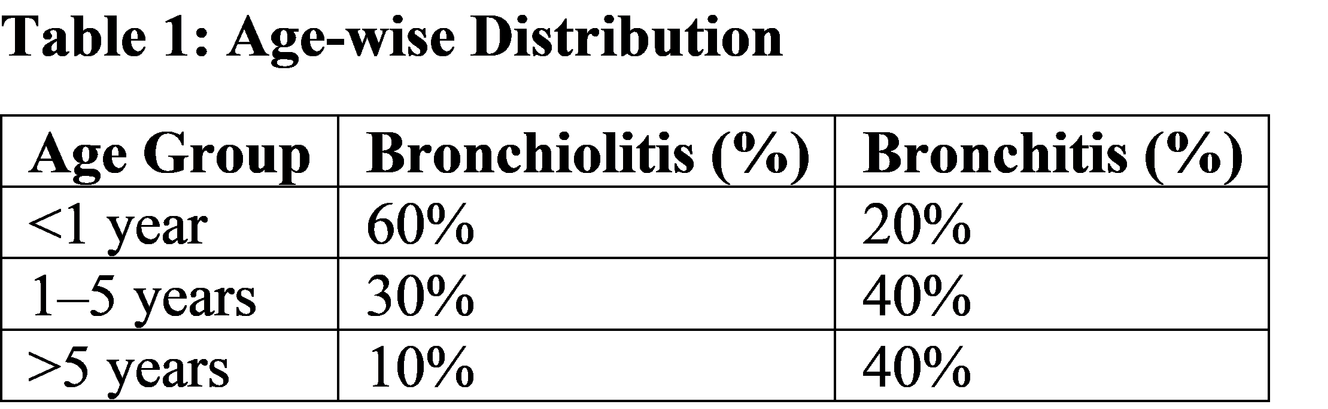
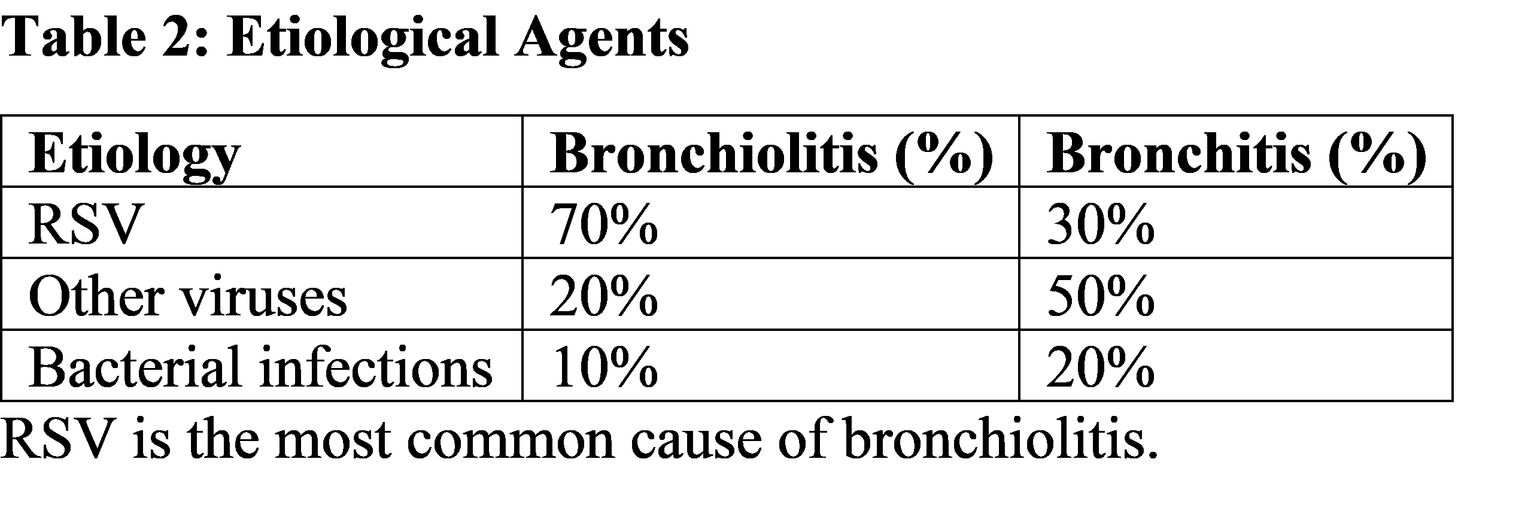
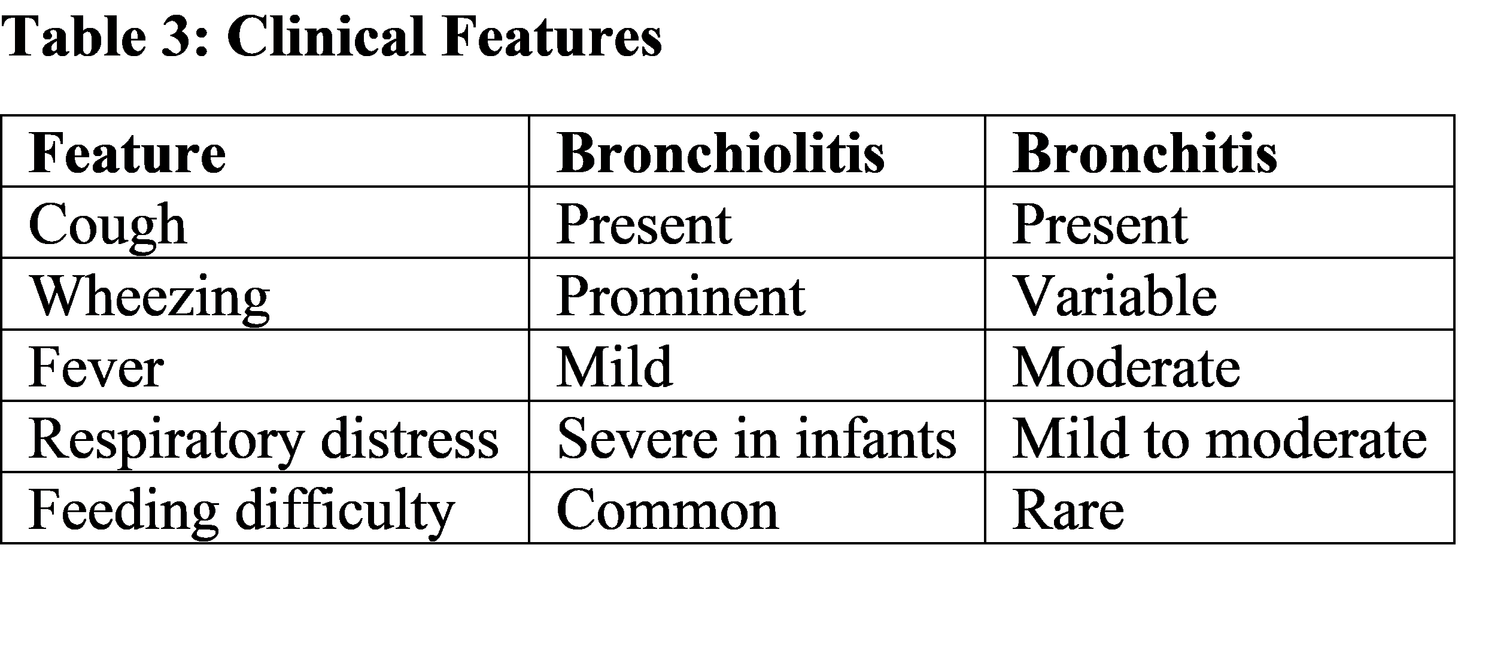
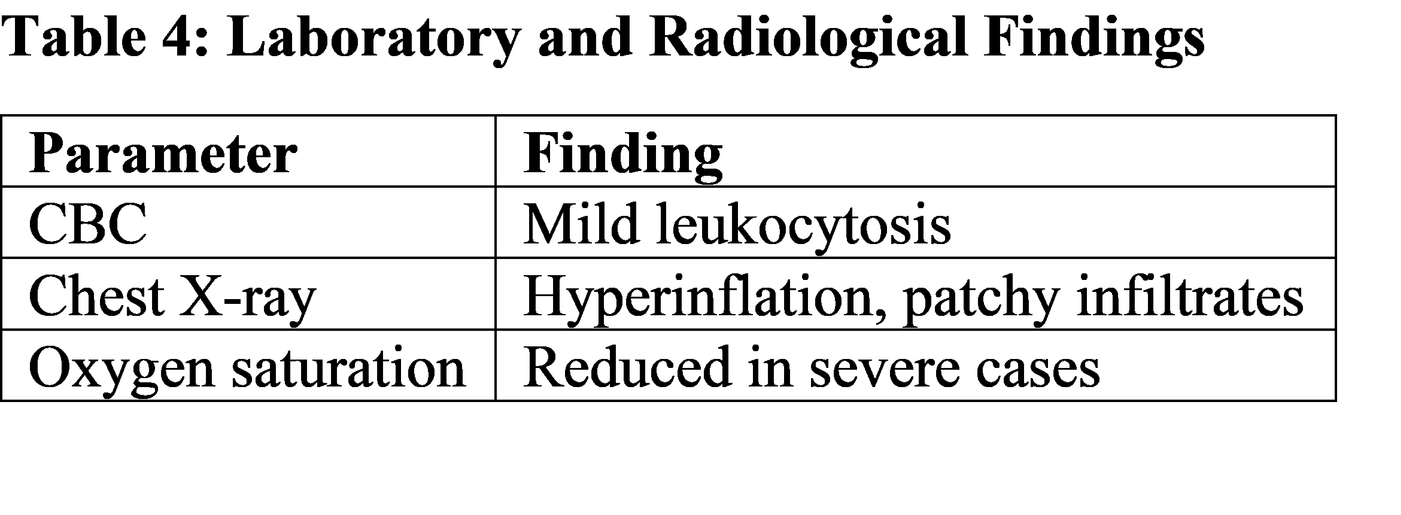
Bronchiolitis is primarily a viral infection affecting the small airways, with RSV being the most common causative agent [7]. The virus infects epithelial cells, leading to inflammation, edema, and necrosis, resulting in airway obstruction [8]. The results indicate that bronchiolitis predominantly affects infants under one year, which aligns with global epidemiological data [9]. The immature immune system and smaller airway diameter contribute to increased susceptibility and severity [10]. Bronchitis, on the other hand, involves larger airways and is often associated with viral infections such as influenza and adenovirus, although bacterial infections may occur [11]. Clinical manifestations such as wheezing, cough, and respiratory distress reflect airway obstruction and impaired gas exchange [12]. Feeding difficulties in infants with bronchiolitis are due to increased work of breathing [13]. Radiological findings such as hyperinflation and patchy infiltrates are common but not routinely required for diagnosis [14]. Diagnosis is primarily clinical, based on history and physical examination [15]. Management of bronchiolitis is mainly supportive, including oxygen therapy, hydration, and monitoring [16]. The use of bronchodilators, corticosteroids, and antibiotics is generally not recommended unless specific indications exist [17]. Comparative studies show consistent findings worldwide, although disease severity is higher in low-resource settings due to delayed access to healthcare [18]. Preventive measures such as breastfeeding, vaccination, and avoidance of tobacco smoke exposure significantly reduce disease incidence [19]. From a clinical perspective, early recognition and appropriate supportive care are essential to reduce morbidity and prevent complications such as respiratory failure [20].
Suggestions / Recommendations
Promote exclusive breastfeeding for at least 6 months
Encourage hand hygiene and infection control practices
Avoid exposure to tobacco smoke and indoor pollutants
Ensure timely vaccination (e.g., influenza)
Early identification of high-risk children (prematurity, congenital heart disease)
Use pulse oximetry for monitoring severity
Avoid unnecessary use of antibiotics
Educate caregivers about warning signs (respiratory distress, poor feeding)
Strengthen hospital-based supportive care facilities
Conclusion
Bronchitis and bronchiolitis are common pediatric respiratory conditions with significant morbidity, particularly in infants. Bronchiolitis is primarily caused by viral infections such as RSV and affects the smaller airways, whereas bronchitis involves larger airways. Diagnosis is mainly clinical, and management is largely supportive. Early recognition and appropriate care are essential to prevent complications. Preventive strategies, including breastfeeding and infection control, play a vital role in reducing disease burden. For MBBS students, understanding these conditions is crucial for effective pediatric practice.
References
Nelson Textbook of Pediatrics, 21st Edition.
Hall CB et al. RSV infections in children. https://pubmed.ncbi.nlm.nih.gov/15613699/
WHO Acute Respiratory Infection Report. https://www.who.int/health-topics/acute-respiratory-infections
Kliegman RM et al. Pediatric respiratory infections. https://www.ncbi.nlm.nih.gov/books/NBK441939/
CDC Bronchiolitis Guidelines. https://www.cdc.gov/rsv/index.html
Guyton & Hall Textbook of Medical Physiology.
Meissner HC. Viral bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/20194258/
Wright M, Piedimonte G. Pathophysiology of bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/15192138/
Florin TA et al. Bronchiolitis epidemiology. https://pubmed.ncbi.nlm.nih.gov/30635283/
Shay DK et al. Bronchiolitis hospitalization. https://pubmed.ncbi.nlm.nih.gov/11752448/
Cherry JD. Bronchitis in children. https://pubmed.ncbi.nlm.nih.gov/12897335/
Ralston SL et al. Clinical features bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/25349312/
Friedman JN et al. Feeding in bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/24470648/
Swingler GH. Radiology in bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/12949297/
NICE Guidelines: Bronchiolitis in children. https://www.nice.org.uk/guidance/ng9
AAP Guidelines Bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/25349312/
Gadomski AM. Bronchodilators in bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/16856038/
Nair H et al. Global burden of bronchiolitis. https://pubmed.ncbi.nlm.nih.gov/22078755/
Victora CG. Breastfeeding benefits. https://pubmed.ncbi.nlm.nih.gov/26869575/
Lozano R et al. Child mortality causes. https://pubmed.ncbi.nlm.nih.gov/23245604/