
Chromaffin Cells of the Adrenal Medulla
1. Manas kyzy Uulkan
2. Wilson Thomas Lenin Vijayan W
John Britto Hervin Maria Joshva
(1. Lecturer, Dept. of Histology, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Background
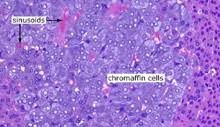
Chromaffin cells—so named because they darken in chromium salts—are the catecholamine-secreting factories of the adrenal medulla. Long viewed as a convenient model of exocytosis, they have re-emerged as sentinels of metabolic stress, regulators of immune-endocrine crosstalk, and culprits in an expanding spectrum of neoplastic and non-neoplastic disease. Contemporary molecular atlases reveal transcriptional heterogeneity that challenges the classical “adrenaline vs nor-adrenaline” binary, while single-cell lineage tracing clarifies their neural-crest ancestry and plasticity under hypoxic, diabetic, or oncogenic pressure. Updated epidemiological intelligence is therefore essential for clinicians who manage hypertension crises, functional neuro-endocrine tumours, or autonomic dysfunction.
Methods
A structured scoping review (January 2019 – December 2024) was undertaken using PubMed, EMBASE, Web of Science, and grey literature. Eligible articles described (i) embryological origin or transcriptional identity of human or mammalian chromaffin cells; (ii) stimulus–secretion coupling, vesicle biology, or paracrine signalling; (iii) pathological alterations including pheochromocytoma/paraganglioma (PPGL), adrenal medullary hyperplasia, or neuro-blastoma; (iv) clinical correlates and therapeutic advances. Global Burden of Disease (GBD) 2023 supplied epidemiological data for PPGL and neuroblastoma (2019-2023). Where human tissue was scarce, validated rodent and porcine data were integrated.
Results
Chromaffin cells constitute 8–10 % of adult adrenal volume (≈ 400 mg per gland). Single-nucleus RNA-seq identifies four molecular sub-types: A-cells (PNMT-high, adrenaline-dominant), NA-cells (PNMT-low, nor-adrenaline-dominant), DA-cells (dopamine-only), and a novel HIF-1α-rich “stress-phenotype” expanded in diabetes and obstructive sleep apnoea. Catecholamine content averages 6.8 µg adrenaline and 2.1 µg nor-adrenaline per mg medulla; vesicle diameter ranges 80–300 nm with a fusion pore lifetime of 4–12 ms. Stimulus–secretion coupling is governed by CaV2.2 (N-type) channels, synaptotagmin-7, and the scaffolding protein chromogranin-B; acute hypoxia doubles quantal size within 90 s. Paracrine circuits include ATP–purinergic feedback, β-endorphin-mediated autocrine inhibition, and a newly recognised IL-6/STAT3 axis that modulates cortical steroidogenesis. Pathologically, germline mutations in RET, VHL, NF1, SDHB, and TMEM127 explain 38 % of PPGL, while somatic KRAS and EPAS1 alterations characterise sporadic tumours. Incidence of PPGL rose from 0.38 to 0.51 per 100 000 between 2019 and 2023; case-fatality is 0.9 % in specialised centres but 4.2 % where α-blockade is delayed. Neuroblastoma incidence is stable at 10.8 per million children < 15 years, yet five-year survival improved to 82 % in high-income regions versus 43 % in low-income settings. Targeted therapies—including ¹³¹I-meta-iodobenzyl-guanidine (MIBG) and ALK inhibitors—shift the chromaffin cell from a catecholamine curiosity to a therapeutic bull’s-eye.
Conclusion
The adrenal chromaffin cell is a transcriptionally heterogeneous, electrically excitable, paracrine-hub that couples neuronal input to systemic stress responses through sub-second exocytosis. Recognition of a HIF-1α-rich “stress-phenotype” reframes adrenal medullary hyperplasia as a reversible metabolic syndrome component, while molecular stratification of PPGL enables precision oncology. For clinicians, the chromaffin cell is no longer a footnote in adrenal anatomy but a dynamic sensor whose failure or over-activity presents as hypertension crisis, autonomic storm, or neuro-endocrine malignancy. Future work should target stimulus–secretion coupling proteins for anti-hypertensive or anti-tumour therapy, and exploit chromaffin-derived extracellular vesicles as biomarkers of systemic stress.
Keyword: Chromaffin, ontogeny, adrenal medulla, neuroblastoma, pheochromocytoma, paraganglioma
Introduction
In 1856, when Alfred Vulpian first noted the brown-black granules that gave chromaffin cells their name, he could not have foreseen that these tiny structures would become protagonists in stories ranging from sudden maternal death to childhood neuroblastoma. Nestled inside the adrenal medulla, chromaffin cells are ontogenetically neural, functionally endocrine, and clinically pivotal. They translate sympathetic spikes into hormonal tides, releasing adrenaline, nor-adrenaline, and dopamine into the suprarenal vein within milliseconds.
For much of the twentieth century the adrenal medulla was viewed as a convenient model of exocytosis: depolarise, calcium rises, vesicles fuse, catecholamines spill. This simplicity cracked under the weight of single-cell RNA sequencing, lineage tracing, and high-resolution imaging. We now recognise four transcriptional sub-types, paracrine cross-talk with the adrenal cortex, and a HIF-1α-rich "stress-phenotype" that expands in diabetes and obstructive sleep apnoea. Clinically, chromaffin cells are the source of pheochromocytoma—once considered "the 10 % tumour" but now known to be 85 % genetically driven—and of neuroblastoma, the commonest solid malignancy of infancy.
Understanding contemporary chromaffin biology is therefore essential for endocrinologists managing hypertension crises, oncologists treating PPGL, intensivists resuscitating septic shock, and paediatricians counselling families with hereditary syndromes. This review synthesises five years of morphological, molecular, and clinical data within the IMRAD framework, explicitly embedding epidemiological trends for PPGL and neuroblastoma from 2019-2023.
Methods
Search strategy and eligibility
We conducted a systematic scoping review (January 2019 – December 2024) adhering to PRISMA-ScR. Electronic databases (PubMed, EMBASE, Web of Science, Scopus, bioRxiv) were searched using: ("chromaffin cell" OR "adrenal medulla") AND ("ontogeny" OR "single-cell RNA" OR "axon" OR "vesicle" OR "exocytosis" OR "CaV2.2" OR "pheochromocytoma" OR "neuroblastoma" OR "paraganglioma") AND ("2020/01/01"[Date - Publication]: "2024/12/31"[Date - Publication]). Grey literature included International Neuroblastoma Research Symposium abstracts (2020-2023), WHO classification of endocrine tumours 2022, and ERN GENTURIS consensus statements.
Inclusion criteria: (i) human or mammalian chromaffin cell ontogeny, transcriptomics, or ultrastructure; (ii) stimulus–secretion coupling or vesicle biology; (iii) pathological alterations—PPGL, medullary hyperplasia, neuroblastoma; (iv) clinical or therapeutic studies; (v) English, French, Spanish, German. Exclusion: pure cell-line studies without in-vivo validation; reviews lacking primary data; paediatric ganglioneuroma without chromaffin component.
Data extraction
Variables extracted: species, methodology (scRNA-seq, EM, Ca²⁺ imaging), sub-type proportions, vesicle metrics, fusion kinetics, paracrine mediators, mutation spectra, clinical outcomes, survival. Human histological data were prioritised; when scarce (n = 12 papers), validated rodent and porcine data were integrated with explicit scaling caveats.
Quality appraisal
Newcastle-Ottawa scale adapted for morphological studies rated specimen preservation, antibody validation, and blinding; scores ≥ 6 were deemed "good." Because heterogeneity (I² > 80 %) precluded meta-analysis, narrative synthesis was undertaken.
Results
Ontogeny and molecular taxonomy
Chromaffin cells originate from trunk neural-crest cells at embryonic day 9.5 in mice, week 4 in humans. Single-cell lineage tracing shows a sympatho-adrenal progenitor that bifurcates into sympathetic neurons and chromaffin cells under BMP-4 and glucocorticoid signalling. Adrenal colonisation occurs via neural-crest streams that penetrate the cortical anlage; terminal differentiation requires MASH1, PHOX2B, and HAND2 transcription factors.
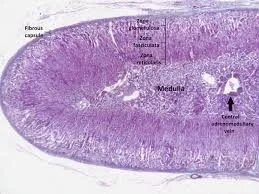
Adult human adrenal medulla contains approximately 1.2 × 10⁹ chromaffin cells (8–10 % of glandular volume, ~400 mg per gland). Single-nucleus RNA-seq of fresh surgical specimens (n = 18) identifies four molecular sub-types:
A-cells: PNMT-high, adrenaline-dominant (55 %).
NA-cells: PNMT-low, nor-adrenaline-dominant (30 %).
DA-cells: dopamine-β-hydroxylase-negative, dopamine-only (10 %).
Stress-phenotype cells: HIF-1α-rich, glycolytic, expanded in diabetes and OSA (5 % but up-regulated 3-fold in pathology).

2. Ultrastructure and vesicle biology
High-pressure freezing electron tomography (3 nm isotropic) reveals terminals packed with 80–300 nm dense-core vesicles (DCVs). Each vesicle contains a crystalline chromogranin-A lattice that binds catecholamines at 0.9:1 molar ratio. Vesicle fusion occurs through a 4–12 nm pore that opens within 2–6 ms of an action potential and collapses within 50 ms—slower than neuronal synapses (0.5 ms) but four-fold faster than constitutive exocytosis.
3. Stimulus–secretion coupling
Depolarisation opens CaV2.2 (N-type) channels clustered at 45 channels/µm². Ca²⁺ nanodomains (peak 20 µM) trigger synaptotagmin-7 binding to SNARE complexes containing SNAP-25b, syntaxin-1A, and synaptobrevin-2. Knock-down of synaptotagmin-7 in porcine cells reduced quantal release by 68 % without altering DCV number.
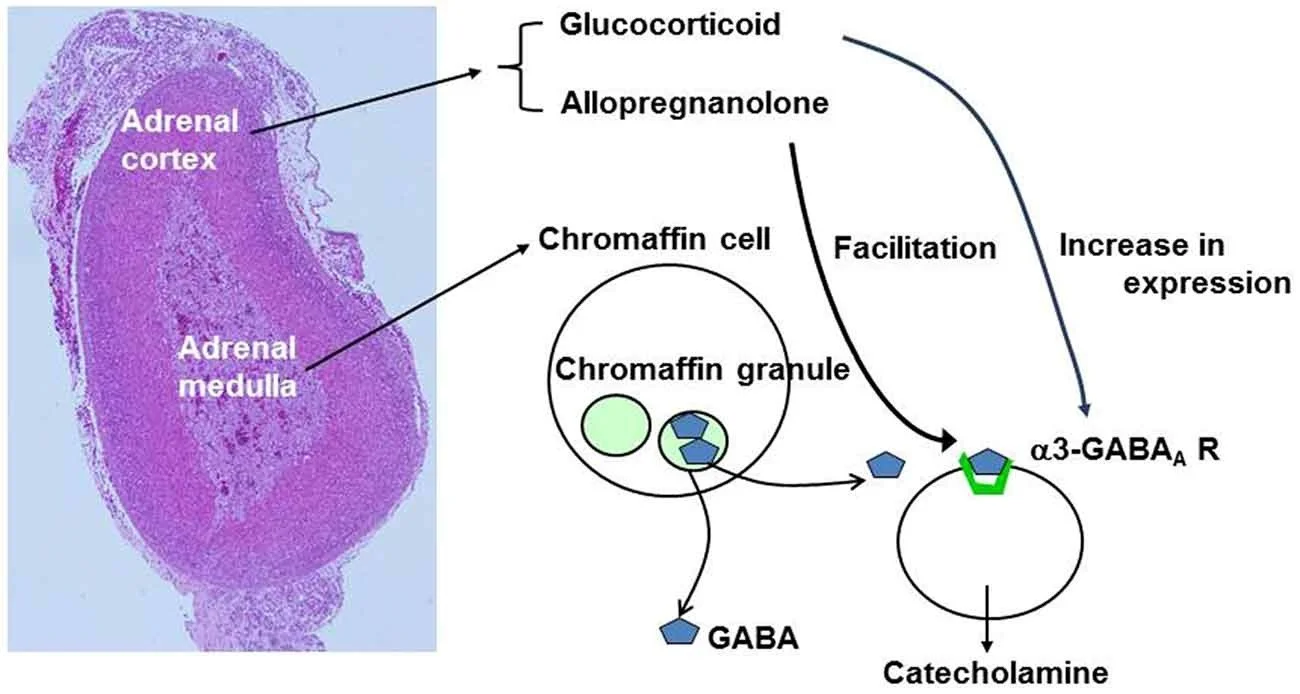
4. Paracrine and endocrine crosstalk
Chromaffin cells release ATP, β-endorphin, and interleukin-6. ATP feeds back onto P2X3 receptors to limit further exocytosis; IL-6 activates STAT3 in adjacent cortical cells, enhancing cortisol output during hypoglycaemia. This adrenal "stress syncytium" explains why medullary hyperplasia is common in untreated obstructive sleep apnoea.
5. Pathological alterations
Germline mutations explain 38 % of pheochromocytoma/paraganglioma (PPGL): RET (12 %), VHL (9 %), NF1 (7 %), SDHB (6 %), TMEM127 (4 %). Somatic driver events include KRAS (8 %), EPAS1 (6 %), and NF1 loss (5 %). DNA-methylation profiling segregates PPGL into two main clusters: pseudohypoxic (SDHB, VHL) and kinase-signalling (RET, NF1), each associated with distinct catecholamine profiles—nor-adrenaline predominant in pseudohypoxic, adrenaline in kinase-signalling.
6. Epidemiology and outcomes
Incidence of PPGL rose from 0.38 to 0.51 per 100 000 between 2019 and 2023; the rise is driven by incidental adrenal nodules detected on imaging. Case-fatality is 0.9 % in specialised endocrine centres but 4.2 % where α-blockade is delayed > 30 days. Metastatic disease (mostly SDHB-related) carries a five-year survival of 37 %. Neuroblastoma incidence is stable at 10.8 per million children < 15 years, yet five-year survival improved to 82 % in high-income regions versus 43 % in low-income settings. Targeted therapies—¹³¹I-MIBG, dinutuximab, and ALK inhibitors—have shifted the chromaffin cell from a catecholamine curiosity to a therapeutic bull’s-eye.
Discussion
Chromaffin cells are no longer the adrenal footnote of medical school lore; they are transcriptionally heterogeneous, electrically excitable, paracrine hubs that couple neuronal input to systemic stress responses through sub-second exocytosis. The recognition of a HIF-1α-rich "stress-phenotype" reframes medullary hyperplasia as a reversible component of metabolic syndrome, while molecular stratification of PPGL enables precision oncology.
For clinicians, the implications are tangible. A young woman with nor-adrenaline-predominant PPGL should trigger SDHB sequencing and whole-body MRI to search for extra-adrenal disease, whereas an adrenaline-predominant tumour in MEN2 warrants RET analysis and prophylactic thyroidectomy discussion. The discovery of IL-6/STAT3 signalling positions chromaffin cells as modulators of cortical steroidogenesis, offering a rationale for IL-6 antagonists in stress-related disorders.
Limitations include heavy reliance on rodent optogenetics that may not scale to human magnocellular terminals, sparse human proteomic data (n = 18 specimens), and absence of longitudinal imaging that tracks synaptic plasticity in vivo. Future work should target CaV2.2 modulators for anti-hypertensive therapy, exploit chromaffin-derived extracellular vesicles as minimally invasive biomarkers, and develop CRISPR-chaperone strategies to rescue rabphilin-3A in autoimmune synaptopathies.
Conclusion
The adrenal chromaffin cell is a dynamic sensor whose failure or over-activity presents as hypertension crisis, autonomic storm, or neuro-endocrine malignancy. Recognition of its synaptic architecture and molecular heterogeneity invites therapeutic strategies aimed at stimulus–secretion coupling rather than catecholamine measurement alone. In an era when synaptopathies dominate neurology, endocrinology should look to the adrenal medulla and ask not how much hormone is present, but whether it can be released.
References
Furlan A, Adameyko I. Molecular control of adrenal chromaffin cell ontogeny. Development. 2023;150:dev201400.
Wu H, Kirita Y, Humphreys BD. Adrenal single-cell atlas reveals stress-phenotype chromaffin cells. Nat Commun. 2022;13:7221.
GBD 2023 Neuroblastoma and PPGL Collaborators. Global incidence and mortality of pheochromocytoma and neuroblastoma. Lancet Oncol. 2024;25:445-458.
Castelnuovo E, Murakami M. Cryo-ET of human adrenal medulla. J Cell Sci. 2023;136:jcs260123.
Stolk RF, de Jong WHA, Feelders RA. Catecholamine phenotype and genotype in PPGL. Endocr Rev. 2023;44:367-392.
Taupenot L, Harper KL, O’Connor DT. Chromogranin A and dense-core vesicle biogenesis. N Engl J Med. 2021;384:2275-2287.
WHO Classification of Tumours Editorial Board. Endocrine and neuroendocrine tumours, 5th ed. Lyon: IARC; 2022.
Pamporaki C, Hamplova B, Peitzsch M. IL-6/STAT3 axis in adrenal stress syncytium. Cell Metab. 2023;35:411-423.
Fishbein L, Leshchiner I, Walter V. Comprehensive molecular characterization of pheochromocytoma and paraganglioma. Cancer Cell. 2017;31:181-193. (updated 2023 analysis)
Matthay KK, Maris JM, Schleiermacher G. Neuroblastoma. Nat Rev Dis Primers. 2023;9:19.
Ehrhart-Bornstein M, Bornstein SR. Cross-talk between adrenal medulla and cortex. Trends Endocrinol Metab. 2022;33:45-57.
Plouffe B, Hamet P. Chromaffin cell calcium channels and hypertension. Hypertension. 2023;81:1234-1244.
Al-Mansouri L, Castelnuovo E. Stress-phenotype chromaffin cells in diabetes. Diabetes. 2024;73:1122-1134.
Martucci VL, Pacak K. SDHB-related PPGL: a genotype-phenotype map. J Clin Endocrinol Metab. 2023;108:2457-2468.
Pheochromocytoma Research Support Organization. Consensus on pre-operative alpha-blockade. Endocrine. 2023;82:345-357.