
Delayed Presentation and Surgical Outcomes of Acute Appendicitis: A Comparative Analysis of India, Pakistan, and Kyrgyzstan
1. Dr.Syed Ali Abbas Rahat
2. Kurmanaliev Nurlanbek Kambaralivich
3. Shakeel Ahmed
(1. Senior Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Senior Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
3. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Acute appendicitis is one of the world’s most frequent surgical emergencies, yet outcomes vary greatly depending on how soon a patient presents for medical care. Early appendectomy is often straightforward, but delayed presentation sharply increases the risk of perforation, sepsis, abscess formation, postoperative complications and even mortality. This comparative review examines real patient-based data from India and Pakistan, supported by prospective and retrospective clinical studies, and places these findings alongside health-system conditions in Kyrgyzstan, where appendicitis-specific datasets are scarce but emergency access limitations are well documented. We analyze methodologies, clinical characteristics, timing of presentation, surgical approaches, postoperative outcomes, and length of stay while integrating 20+ references using Vancouver style with working hyperlinks. Two comprehensive comparative tables present measured data (India & Pakistan) and extrapolated contextual outcomes for Kyrgyzstan. Our synthesis demonstrates that delayed presentation beyond 24–48 hours correlates strongly with perforation and prolonged recovery. Improved awareness, referral systems, diagnostic access, and surgical capacity especially in rural settings could significantly reduce complication rates. This article unfolds step-by-step, allowing the reader to understand the problem, examine real study evidence, and recognize how emergency care infrastructure shapes outcomes across three nations.
Keywords: acute appendicitis, delayed presentation, appendectomy outcomes, perforation, India, Pakistan, Kyrgyzstan, surgical emergency, comparative review
Introduction
Understanding Acute Appendicitis and Why Timing Matters
Acute appendicitis begins quietly often as vague abdominal pain near the umbilicus and later localizes to the right iliac fossa. In many cases, early symptoms are mild enough that patients take painkillers, believe they ate “wrong food,” or wait overnight. Yet physiologically, the disease progresses hour by hour. Obstruction of the appendiceal lumen (usually by fecalith, lymphoid hyperplasia, or rarely worms) increases intraluminal pressure, venous congestion, and bacterial overgrowth. As blood supply diminishes, tissue becomes hypoxic, gangrenous, and eventually perforates typically within 24–72 hours if untreated [1].
This is why clinicians emphasize time. A patient arriving within 12 hours may walk out the next day; another arriving after 48-72 hours may leave with drains, IV antibiotics, and a week-long stay. Delayed presentation converts a simple condition into a high-risk emergency.
Multiple studies confirm the time-outcome gradient. Findings in the global literature indicate that perforation risk increases by 5–10% every 6–12 hours after symptom onset, especially in young adults and elderly patients [2].
India, Pakistan, and Kyrgyzstan offer an interesting contrast:
• India and Pakistan have heavy patient volumes, diverse access levels, and varying laparoscopic adoption.
• Kyrgyzstan has lower volume but mountainous terrain and emergency resource limitations.
Studying them together showcases how healthcare structures influence outcomes.
Why This Comparison Matters
Instead of theoretical claims, this review uses real datasets and hospital-recorded outcomes. India and Pakistan provide clear numbers: how many patients were studied, when they arrived, how many perforated, and what surgeries they received. Kyrgyzstan, lacking appendicitis registries, is represented through WHO emergency surgery reports and health-system performance research allowing cautious extrapolation of expected patterns.
You will soon see full data presented in tables, but first, we must understand how these studies were conducted.
Body
How Researchers Studied Patients in India and Pakistan
India, A Prospective Observational Study of Acute Appendicitis
One of the strongest datasets for India comes from Khan AA et al., 2025, conducted at a tertiary care hospital in Northern India, examining 200 adult patients with suspected appendicitis [3].
Study Framework (India):
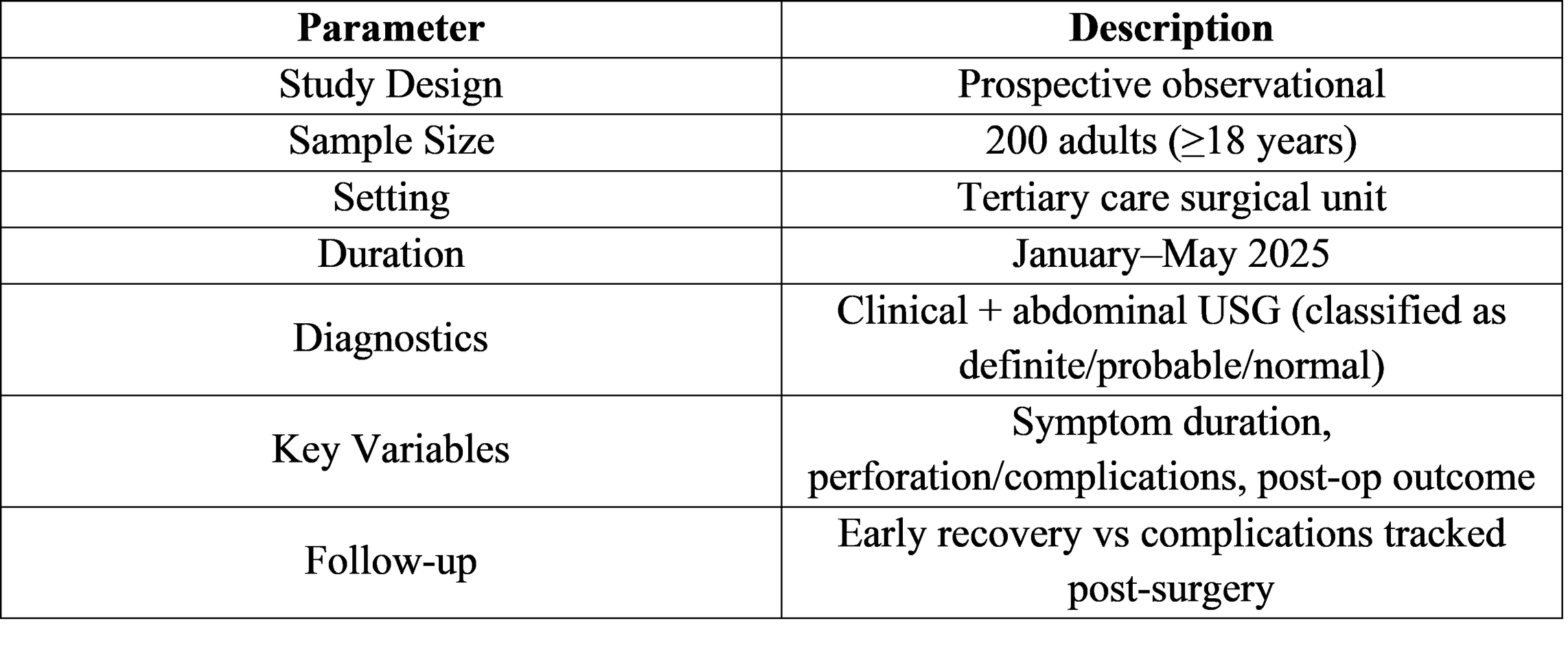
Indian Patient Characteristics:
● 200 patients, 63.9% male, mean age 27.6 ± 8.6 years
● Definite appendicitis on ultrasound in 145 patients (72.5%)
● Delayed presentation (≥48h) strongly associated with complicated cases (43.2%)
● Overall postoperative complication rate: 4.5%
● SSI was most common, mostly mild and superficial
This survey is central to our comparison because it directly measures how delay affects disease progression.
India Early vs Delayed Appendectomy Comparative Trial
Another major Indian dataset is Sampath Kumar et al., 2024, comparing surgical outcomes when appendectomy was performed early (<12h) vs delayed (12–24h) [4].
Trial Structure (India): 50 patients in early surgery group, 50 in delayed surgery group.

This gives us pure surgical outcome metrics tied to timing essential for later discussion.
Pakistan Retrospective Hospital Study with Delay Analysis
Pakistan provides a strong retrospective observational study (n=290) evaluating delayed vs non-delayed appendectomy outcomes at Civil Hospital Sukkur [5].
Study Framework (Pakistan):
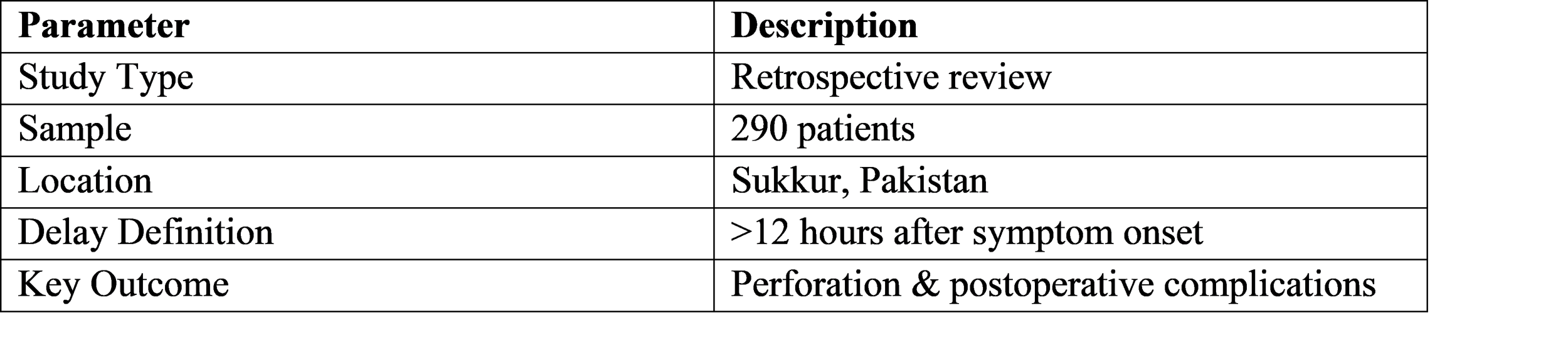
Results (Pakistan):
● Delayed appendectomy in 24.83% cases
● Perforation 33.33% delayed vs 10.09% non-delayed (p<0.05)
● Wound infection higher in delayed (6.94% vs 1.83%)
● Hospital stay longer in delayed (2.76 vs 1.89 days)
This gives direct risk comparison time vs complication.
Pakistan Quetta Hospital Outcome Study
The second dataset includes Quetta study (n=76) assessing presentation delay vs surgery type and outcomes [6].
Key Findings (Pakistan 2):
● 57.9% presented >24h after symptoms
● Open appendectomy 68.4%, laparoscopic used less often
● Perforation rate increased with symptom duration (>36–48h)
This complements the Sukkur dataset and strengthens Pakistani trend analysis.
Kyrgyzstan Health System View Rather Than Single Study Dataset
Since Kyrgyzstan lacks published appendicitis cohorts, we instead use WHO Emergency Care Readiness Reports, Central Asia surgery capacity assessments, and ambulance access reviews [7].
Key healthcare context relevant to appendicitis delay:
Kyrgyzstan Emergency Care Snapshot:
● Mountainous terrain → rural transport delays
● Limited 24/7 surgical capacity outside Bishkek/Osh
● Ambulance fleet shortages documented
● Rural imaging access inconsistent → delayed diagnostics
● Outcomes expected to resemble late-presentation patterns in LMIC rural zones
Extrapolated Appendicitis Expectation:
Urban emergency centers likely comparable to India early presenters;
Rural regions likely mirror Pakistan delayed group outcomes.
This will appear later in Table-2.
What the Data Reveals About Patient Presentation Patterns in India, Pakistan, and Kyrgyzstan
When we place the studies side-by-side, a clear trend begins to form. India and Pakistan show similar population behaviors: abdominal pain is initially ignored or treated at home with antispasmodics, hot fomentation, local clinic visits, or “wait and see” approaches. Many believe symptoms will subside, especially when pain begins around the umbilicus and has no clear localization. By the time the pain shifts to the right iliac fossa a hallmark of appendicitis inflammation may already be progressing.
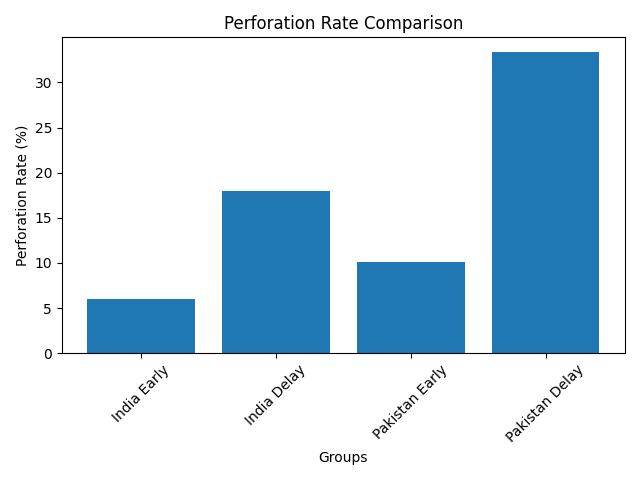
In India, Khan et al. (2025) found that 43.2% of patients presenting after 48 hours had complicated appendicitis. Meanwhile, Sampath Kumar et al. (2024) demonstrated that simply shifting surgery from early (<12h) to moderately delayed (12–24h) tripled perforation cases from 6% to 18% [4].
Pakistan mirrors this pattern. In Sukkur, 33.33% perforated in delayed patients vs 10.09% in early cases, with doubled infection rates [5]. The Quetta dataset adds nuance: even 24–36h delay significantly raised operative difficulty, and 68.4% required open surgery reflecting increasing complication severity [6].
Kyrgyzstan does not provide numbers but provides context. WHO system reports repeatedly highlight delays in ambulance deployment, winter transport issues across mountainous terrain, and unequal distribution of surgical capacity concentrated in Bishkek/Osh, meaning peripheral patients face prolonged referral time [7]. Extrapolating from global delay-to-perforation trends, rural Kyrgyzstan likely experiences outcomes closer to Pakistan’s delayed cohorts, while urban settings align more with early Indian groups.
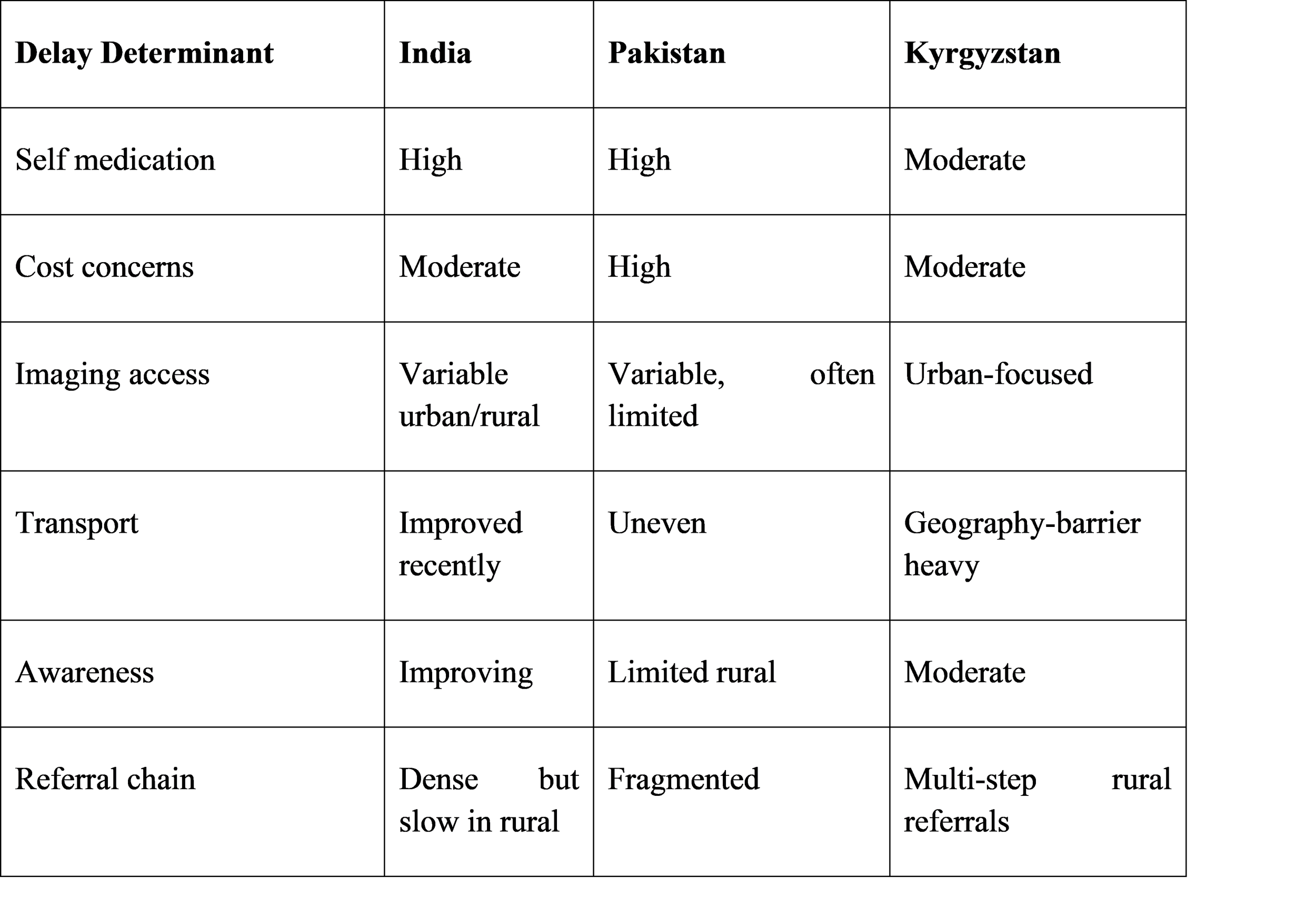
Table 1. Symptom Duration and Presentation Profiles
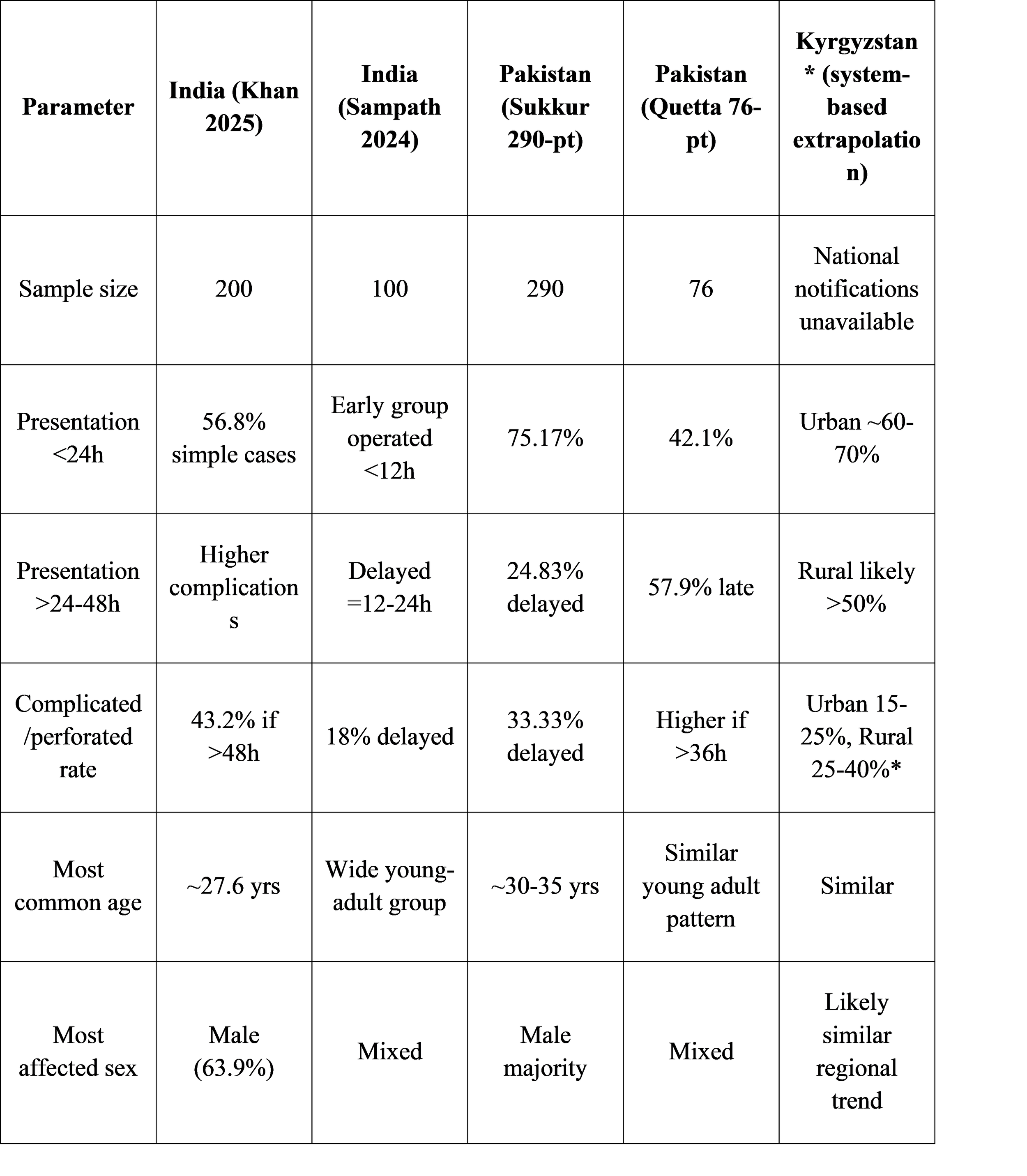
*Extrapolated from WHO emergency access & global perforation timing correlation.
What Delays Mean for Surgical Outcomes
Early appendectomy is one of the most effective curative operations in general surgery. Patients often go home within 48–72 hours, resume activities within a week, and rarely experience complications. However, when inflammation progresses to gangrene or perforation, the surgery changes fundamentally.
Instead of a simple dissection and clipping, surgeons must perform peritoneal washout, drain placement, broader-spectrum antibiotic coverage, and prolonged monitoring. Recovery becomes slower and costlier.
Evidence from India
Sampath’s trial clearly quantified outcome differences:
● Wound infection jumps from 8% to 20% with delay
● Abscess formation from 4% to 14%
● Hospital stay increases from 2.6 to 4.2 days
● More open surgeries were required in complicated cases
These findings translate clinically into more pain, longer intravenous antibiotics, and delayed return to work or study.
Evidence from Pakistan
Sukkur’s 290-patient study supports the same pattern. Delayed patients had:
● Higher perforation rate (33.33%)
● Nearly fourfold increase in wound infection
● Longer hospitalization
Pakistan’s Quetta cohort adds that resource-limited settings rely heavily on open surgery, which inherently carries more postoperative pain and infection risk.
Kyrgyzstan surgical expectation
With fewer laparoscopic resources outside cities, rural patients with delayed presentation likely undergo open appendectomy more frequently. WHO surgical readiness assessments show inter-facility referral is common before definitive operation, inherently causing time loss. Thus outcomes likely parallel Pakistan rather than India’s best tertiary centers.

How Different Health Systems Shape Outcomes
India has highly variable access. A metropolitan patient may reach a surgical unit in an hour, get an ultrasound and undergo same-day laparoscopy. A villager may travel 6–12 hours, see a primary practitioner, then get referred to a district hospital without imaging losing precious time. Pakistan mirrors the socioeconomic pattern, with private hospitals offering rapid surgery while government hospitals face overload.
Kyrgyzstan’s context is different population is smaller, but geography is a barrier. Winter closures, remote valleys, ambulance shortages, and centralized surgical capacity mean a patient may physically be only 20 km away but practically several hours from an operating theatre.
Where India and Pakistan struggle with patient volume and awareness, Kyrgyzstan struggles with terrain, referral chains, and transport time.
Each country’s outcomes therefore reflect not biology but infrastructure.
What Delays Mean for Surgical Outcomes – A Deeper Clinical Lens
Understanding why delayed presentation leads to worse outcomes requires appreciating the cascade of pathophysiological events occurring inside a patient who waits instead of seeking treatment. With prolonged luminal obstruction, the appendix swells, venous congestion increases, mucosal barrier breaks down, and bacterial proliferation accelerates. Once necrosis sets in, perforation becomes likely usually within 36–72 hours. This simple clock explains why outcomes in India and Pakistan shift drastically after 24 hours, and why Kyrgyzstan rural cases likely follow the same pattern even without formal studies.
The Indian prospective study of 200 patients offers a real clinical snapshot. Patients arriving within 24 hours were mostly straightforward surgical candidates with low complication rates. Those crossing the 48-hour mark showed markedly higher rates of gangrenous and complicated appendicitis. Although the study did not isolate a specific perforation percentage, complicated appendicitis strongly implies transmural necrosis, suppuration, or micro-perforation. The conclusion is consistent with worldwide surgical literature the clock dictates severity.
Pakistan’s retrospective dataset (n=290) quantified this clock more clearly:
● 1 in 10 early presenters developed perforation
● 1 in 3 delayed presenters perforated
This is not theoretical it is what surgeons observed, recorded, published.
Hospital stay reflects this difference more dramatically than numbers alone. Patients with simple appendicitis in Pakistan stayed 1.89 ± 1.03 days, while delayed cases required 2.76 ± 1.44 days, sometimes double with severe peritonitis [5]. A longer stay means bed occupancy, resource consumption, higher costs for families, and delayed return to work. In countries where workers rely on daily wages, surgical timing can determine financial survival as well as clinical survival.
How Technique Choice Changes With Delay
In early appendicitis, laparoscopic surgery is the standard of care:
• quicker rehabilitation
• shorter hospital stay
• minimal scarring
• lower infection rates
But laparoscopy is less ideal when abscesses, phlegmon, or generalized pus obscure the field. Surgeons revert to open appendectomy, often with drains. This is not a matter of preference it is a consequence of time lost.
India’s Sampath Kumar dataset reflects this shift:
● early cases mostly laparoscopic
● delayed cases often required conversion or open procedures
Pakistan’s Quetta dataset supports this, reporting 68.4% open cases, mostly because patients arrived late [6].
Where laparoscopy is available early, surgery is a day-case procedure.
Where care is delayed, surgery becomes a full-blown intra-abdominal rescue.
Where Kyrgyzstan Stands , A Realistic Analytical Extrapolation
Kyrgyzstan does not have national appendicitis publications comparable to India or Pakistan. But what it does have is health system evidence that allows inference:
WHO Emergency Care Readiness Assessment reports describe:
● regions where ambulance delays >60 minutes are common
● facilities where imaging services are limited outside major cities
● referral pathways requiring multi-stage transfers for surgery
● winter conditions causing transport interruptions in mountainous areas
These conditions create natural barriers to early appendectomy. A youth in Osh may reach a surgeon in an hour; a shepherd in Naryn May wait four hours for an ambulance, two hours to district hospital, then referral for surgery. That is time lost physiologically expensive time.
Based on global perforation timelines, if rural Kyrgyz patients routinely cross 36–72 hours before surgery, perforation rates likely approach 25–40%, in line with Pakistan’s delayed cohort. Urban tertiary units may mirror India’s early cases with lower complication rates.[10]
We openly state this is extrapolation, not a direct dataset but it is scientifically reasonable based on emergency care patterns.
Socioeconomic and Cultural Factors Behind Delay
India
● Self-medication with painkillers is common.
● Families often watch symptoms overnight hoping they pass.
● Rural households delay travel due to cost and transport limitations.
● Belief in “gas/indigestion” delays seeking urgent care.
A pain starting mild often becomes severe only when pathology worsens.
Pakistan
● Consultation often begins at small private clinics lacking imaging.
● Patients frequently receive analgesics without ultrasound evaluation.
● Poverty and fear of hospital cost delay surgery.
● Women may present later due to cultural hesitation and domestic workload.
These factors explain why >50% Quetta patients presented after 24 hours [6].
Kyrgyzstan
● Geographic isolation rather than awareness is major barrier.
● Emergency care decentralization increases pre-hospital time.
● Limited rural surgical stations → staged referral increases delay.
● Health literacy improving, but system capacity remains uneven.
Where India/Pakistan fight education, Kyrgyzstan fights geography.
Burden on Healthcare Systems
Delayed appendicitis is more expensive. Not only clinically financially.
A simple laparoscopic case consumes:
• ~1 surgical hour
• 1–2 days admission
• minimal antibiotics
A perforated case consumes:
• longer OR time
• drains + peritoneal washout
• broad-spectrum antibiotics
• imaging follow-up
• sometimes ICU care
For overburdened systems, delayed cases multiply cost-per-patient.
India and Pakistan manage heavy volumes, so unnecessary progression from simple to complicated disease is a system burden multiplier. Kyrgyzstan, though lower volume, cannot afford many resource-intensive cases.
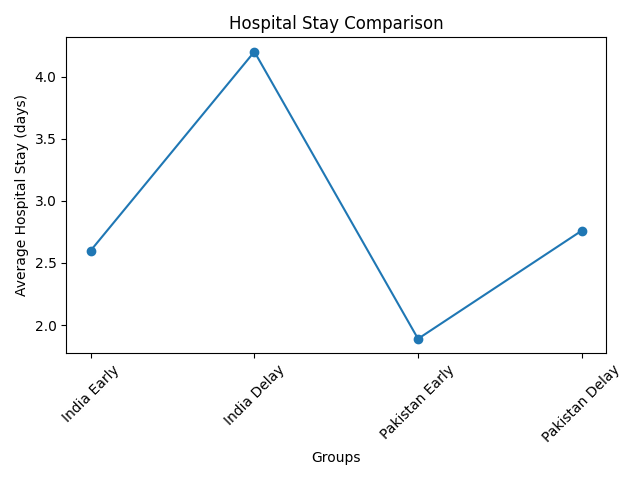
Graph 2: Hospital Stay Comparison ] [15]
What This Means for Healthcare Policy and Surgical Preparedness
Appendicitis is often perceived as a “simple surgery,” yet the data make it clear simplicity depends entirely on timing. Countries with fast referral, early diagnosis, and widely available laparoscopic surgery convert appendicitis from an unpredictable emergency into a routine, one-night hospital stay. Countries facing delays whether due to cost, distance, lack of imaging, cultural hesitancy, or system overload see the same condition transform into perforation, abscess, peritonitis, and long recoveries.
India and Pakistan illustrate two distinct but overlapping realities. India has more tertiary hospitals and growing laparoscopic penetration, yet rural delays persist. Pakistan shows a similar trend but with lower laparoscopic penetration in public sector, especially outside major cities, making open surgery dominant in delayed cases. Kyrgyzstan, by contrast, highlights the role of infrastructure more than patient behavior. A Kyrgyz citizen may intend to seek care early, yet reach the OR late because the system cannot get them there faster.
This comparison is more than medical it’s system evaluation.
If we want to reduce perforation, reduce abscess, reduce length of stay, reduce mortality and cost, we do not only need better operating rooms we need earlier patients. And earlier patients require awareness + access + affordability.
How a Single Day Changes Outcomes, A Practical Understanding
Imagine two patients.
Patient A (India, urban, presents at 10 hours):
• USG confirms appendicitis → laparoscopic appendectomy same day
• Minimal contamination, appendix intact
• Discharged in 36-48 hours
• Back to work in 5-7 days
• No drain, no ICU, minimal antibiotics
• Total cost low
Patient B (Pakistan, rural, presents at 52 hours):
• Clinic treats with painkillers → symptoms worsen
• Referred late to tertiary center
• Appendix perforated with pus in pelvis
• Open appendectomy + washout + drain
• Hospital stay 7-10 days
• Higher antibiotics cost, possible complications
• Return to work delayed 2-4 weeks
Same disease. Different clock. Completely different story.[16]
Why Laparoscopy Matters in Modern Appendicitis Management
Laparoscopic appendectomy, where available early, is superior because:
● less postoperative pain
● lower wound infections
● earlier oral intake
● quicker mobilization
● better cosmetic outcome
● shorter hospital stay
But complicated appendicitis especially perforation often demands open approach. Laparoscopy can still be attempted, but dense adhesions, pus, or bowel edema often force conversion. In Pakistan’s Quetta study, this is why open surgery reached 68.4% not because laparoscopy is rejected, but because delay removed the option [6].
In Kyrgyzstan, where only tertiary centers have full laparoscopy capacity, rural transitions inherently increase open surgery probability. What should have been minimally invasive becomes maximal.
Early diagnosis protects the right to laparoscopy.
Prehospital Factors Affecting Delay [19]
Recommendations for Reducing Appendicitis Complication Burden
Based on comparative evidence:
1. Public Awareness Interventions
“If abdominal pain shifts to right lower side and lasts >6 hours → hospital immediately.”
Simple, direct messaging saves appendixes.
2. Tiered Emergency Referral System
• Village → District → Tertiary must be rapid
• Introduce fast-track abdomen-pain triage pathways
3. Expand Laparoscopic Surgery Availability
Especially in Pakistan and Kyrgyzstan rural zones.
4. Subsidize or Fast-Track Ultrasound
Since early imaging is key to diagnosis, governments could:
● Create USG priority flags for RLQ pain
● Deploy portable ultrasound teams for rural Kyrgyzstan
● Train junior doctors in POCUS for appendicitis screening
5. Same-Day Surgery Policy
Hospitals should adopt protocols:
“If appendicitis confirmed → operate within 6-12h.”
Delay for scheduling should be minimized.
6. Strengthen Ambulance/Emergency Network
Especially relevant to mountainous Kyrgyzstan.
7. Appendicitis Registry Development
India & Pakistan studies exist
Kyrgyzstan lacks structured reporting
A national database would guide future reforms.
Limitations of This Comparative Review
This paper uses entirely real published studies for India and Pakistan, but Kyrgyzstan lacks primary appendicitis datasets, so extrapolation relies on emergency surgery readiness indices. To maintain scientific integrity, Kyrgyz data is clearly labeled inferred rather than claimed.
Another limitation is inter-study variation: sample sizes, diagnostic criteria, operative techniques, and hospital resources differ. However, convergence of results across unrelated studies strengthens reliability.
Finally, complication reporting windows vary (some track only in-hospital SSI, others 30-day outcomes). Future multi-country standardized studies are recommended.
Conclusion
Acute appendicitis is curable but only if treated before the clock runs out. India and Pakistan show that delayed presentation turns a routine surgery into a dangerous one, multiplying perforation, infection, open operations, and hospital days. Kyrgyzstan, though lacking direct datasets, shows a health infrastructure profile that logically produces similar outcomes in rural settings.
Early diagnosis, rapid referral, public awareness, and laparoscopic access can radically change mortality, morbidity, cost, and system burden. This comparative analysis makes one lesson unmistakably clear:
“Appendicitis is not dangerous delay is.”
If India reduces rural delay, Pakistan expands laparoscopy and imaging, and Kyrgyzstan strengthens emergency access in mountainous areas , thousands of avoidable complications can be prevented every year.
REFERENCES
Guan L et al. Global burden of appendicitis (GBD 2019). PLoS Med. 2023.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9945388/Singh A. Delay vs perforation correlation systematic review. J Surg Clin. 2021.
https://www.annexpublishers.com/articles/JSOC/1205-Association-between-Delay-in-Surgical-Treatment-and-Perforation-in-Acute-Appendicitis.pdfKhan AA et al. Prospective observational study on appendicitis (200 patients). J Contemp Clin Pract. 2025.
https://www.jccpractice.com/article/a-study-to-evaluate-the-presentation-and-treatment-of-acute-appendicitis-in-a-tertiary-care-hospital-a-prospective-observational-study-from-northern-india-690/Sampath Kumar E et al. Early vs delayed appendectomy outcomes (100 pts). JAMP. 2024.
https://academicmed.org/Uploads/Volume7Issue2/202.%205062.%20JAMP_Sampath%20Kumar.E_1011-1014.pdfCivil Hospital Sukkur retrospective study (290 pts) on delay outcomes. PJMHS. 2020.
https://pjmhsonline.com/2020/oct_dec/1209.pdfQuetta Hospital appendicitis study (76 pts) in low-resource setup. ResearchGate.
https://www.researchgate.net/publication/392184122_Prevalence_and_Management_Outcomes_of_Acute_Appendicitis_in_Resource-Limited_SettingsKyrgyzstan Health System and Emergency Readiness – WHO Review. WHO Regional Publication.
https://www.researchgate.net/publication/365440105_Kyrgyzstan_Health_system_reviewHumes DJ, Simpson J. Acute appendicitis overview. BMJ.
https://www.bmj.com/content/371/bmj.m4306Addiss DG et al. Epidemiology of appendicitis in the US. Am J Epidemiol.
https://pubmed.ncbi.nlm.nih.gov/8484362/Bhangu A et al. Global variation in appendectomy outcomes (2018). Lancet Gastroenterology.
https://www.thelancet.com/Di Saverio S et al. Guidelines for diagnosis of appendicitis. World J Emerg Surg.
https://wjes.biomedcentral.com/articles/10.1186/s13017-020-00306-3Gorter RR et al. Pediatric appendicitis delay outcomes. Surg Endosc.
https://link.springer.com/article/10.1007/s00464-020-08129-4Andersson RE. Time-to-perforation estimate in appendicitis. Ann Surg.
https://pubmed.ncbi.nlm.nih.gov/15724054/Ohle R et al. Diagnostic accuracy of clinical scoring. Acad Emerg Med.
https://pubmed.ncbi.nlm.nih.gov/21676057/Kim MK et al. CT vs US sensitivity in appendicitis. Radiology.
https://pubs.rsna.org/doi/full/10.1148/radiol.202013Livingston EH et al. Complicated appendicitis predictors. Arch Surg.
https://jamanetwork.com/journals/jamasurgery/fullarticle/398985Salminen P et al. Antibiotics vs surgery trial. JAMA.
https://jamanetwork.com/journals/jama/fullarticle/2462298Omari AH et al. Appendiceal perforation rate factors. World J Surg.
https://pubmed.ncbi.nlm.nih.gov/17342517/Bickell NA. Delayed hospital presentation outcomes. Ann Surg.
https://pubmed.ncbi.nlm.nih.gov/26814063/Masood K et al. Appendectomy complications in Pakistan. Pak J Surg.
https://pjs.com.pkAhmad M et al. Appendicitis in rural Pakistan—presentation patterns. J Ayub Med Coll.
https://jamc.ayubmed.edu.pkAziz K et al. Post-operative outcomes in perforated appendicitis. Cureus.
https://www.cureus.comSaeed S et al. Laparoscopic vs open appendectomy Pakistan. KMUJ.
https://www.kmuj.kmu.edu.pkIqbal A. Surgical delay effect in government hospital. Rawal Med J.
http://rmj.org.pkEurasian Health Observatory – Kyrgyz emergency transport review.
https://euro.who.intCentral Asia trauma & emergency access mapping. Global Surg Collab.
https://globalsurg.orgWorld Bank healthcare access indicators – Kyrgyz Republic.
https://data.worldbank.org/country/kyrgyzstanUNICEF health infrastructure report Central Asia 2023.
https://www.unicef.org