
Compare the age characteristics of blood vessel
1. Manas kyzy Uulkan
2. Jenisha Prabhu
(1. Lecturer, Dept. of Histology, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Introduction
The human circulatory system is a marvel of biological engineering, comprising a vast network of blood vessels that extend over 60,000 miles within the body. This intricate system ensures the delivery of oxygen and nutrients to tissues, the removal of metabolic waste, and the maintenance of homeostasis. Central to its function are three primary types of blood vessels: arteries, veins, and capillaries. Each vessel type exhibits unique structural and functional characteristics, adapting to specific roles in the circulatory process. Understanding these differences is essential for students of biology and medicine, as it provides the foundation for grasping cardiovascular physiology, pathology, and clinical interventions.
This article presents a comprehensive comparison of arteries, veins, and capillaries, exploring their histological architecture, pressure dynamics, wall thickness, presence of valves, oxygen content, and their respective roles in the circulatory system. Special attention is given to the subtypes of arteries and capillaries, the mechanisms of blood flow regulation, and the clinical implications of vessel dysfunction.
Overview of Blood Vessel Types
Blood vessels are classified into three main categories: arteries, veins, and capillaries. Each plays a distinct role in the circulatory system:
Arteries carry blood away from the heart, typically under high pressure.
Veins return blood to the heart, operating under lower pressure and often against gravity.
Capillaries serve as the exchange sites between blood and tissues, facilitating the transfer of gases, nutrients, and waste products.
The sequence of blood flow follows a logical progression: heart → arteries → arterioles → capillaries → venules → veins → heart.
Structural Comparison: Vessel Wall Architecture
The Three Tunics
Both arteries and veins share a common wall structure composed of three layers, known as tunics:
Tunica Intima: The innermost layer, consisting of a single layer of endothelial cells supported by a basement membrane and subendothelial connective tissue.
Tunica Media: The middle layer, primarily composed of smooth muscle cells and elastic fibers. This layer is much thicker in arteries than in veins.
Tunica Externa (Adventitia): The outermost layer, made up of connective tissue (mainly collagen), which provides structural support and anchors the vessel to surrounding tissues.
Capillaries, in contrast, possess only the tunica intima—a single endothelial cell layer with a basement membrane—optimizing them for exchange rather than transport.
Cross-Sectional Structure: Visual Comparison
The image above illustrates the cross-sectional differences between an artery, vein, and capillary. Arteries have thick muscular walls and a rounded lumen, veins have thinner walls and a larger, often irregular lumen, while capillaries are composed of a single endothelial layer.
Arteries are designed to withstand high pressure, veins to accommodate large volumes of blood at low pressure, and capillaries to maximize exchange efficiency.
Table 1: Structural and Functional Comparison of Arteries, Veins, and Capillaries
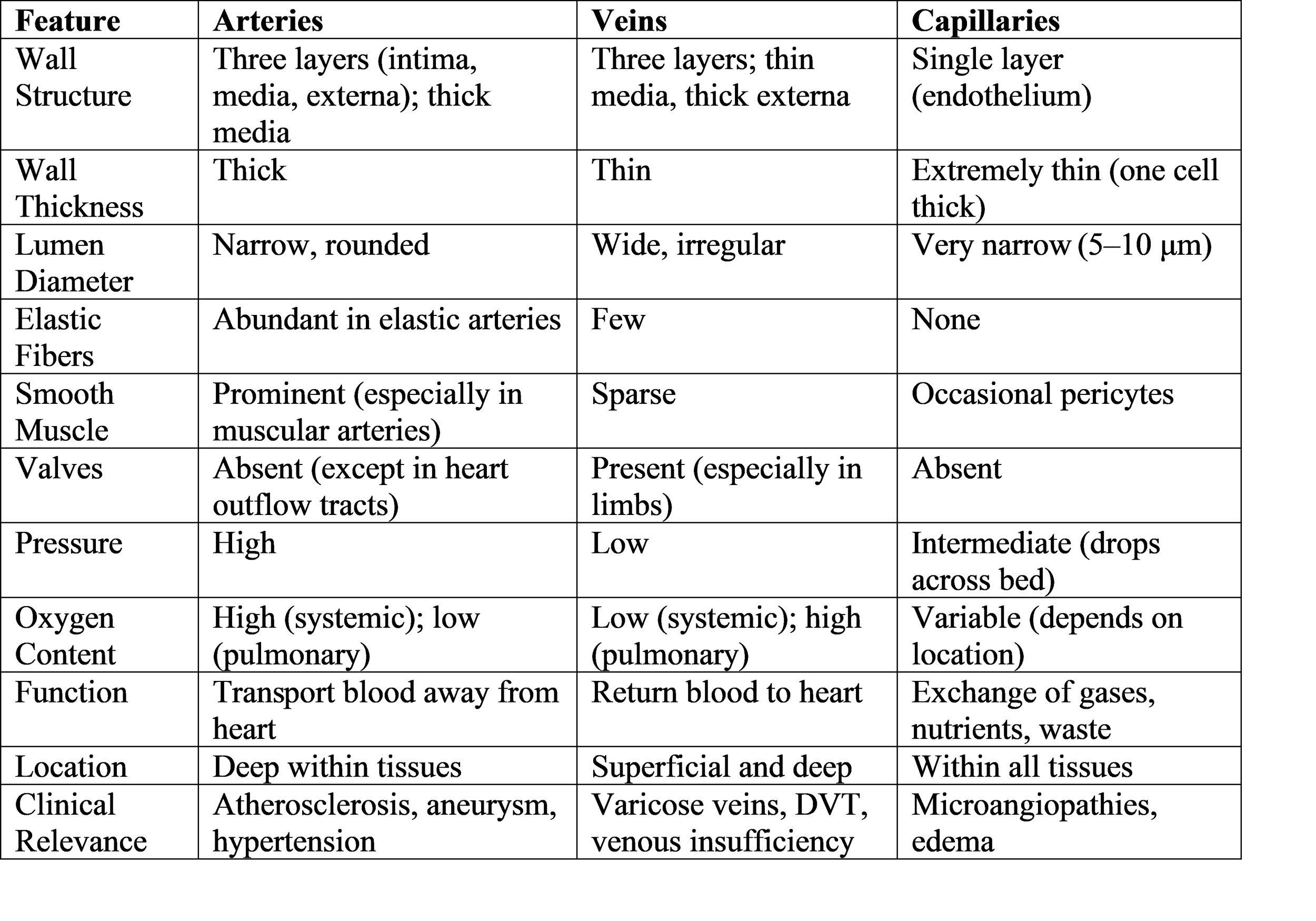
Arteries: Structure, Types, and Specializations
General Features
Arteries are robust vessels that conduct blood away from the heart. Their walls are thick and muscular, designed to withstand and regulate the high pressure generated by cardiac contractions. The tunica media is especially prominent, containing multiple layers of smooth muscle and elastic fibers.
Arteries are typically located deep within the body, protected by muscle and connective tissue. Their lumens are narrow and rounded, maintaining pressure and facilitating rapid blood flow.
Types of Arteries
Arteries are further classified based on their size and wall composition:
1. Elastic Arteries (Conducting Arteries)
Location: Closest to the heart (e.g., aorta, pulmonary trunk, major branches)
Structure: Thick tunica media with abundant elastic fibers (elastic laminae)
Function: Accommodate surges of blood from the heart, expand during systole, and recoil during diastole (Windkessel effect), maintaining continuous blood flow and pressure.
Diameter: >10 mm
Elastic arteries buffer the pulsatile output of the heart, reducing pressure fluctuations and protecting downstream vessels.
2. Muscular Arteries (Distributing Arteries)
Location: Further from the heart, supplying organs and tissues (e.g., radial, femoral, coronary arteries)
Structure: Tunica media dominated by smooth muscle, less elastic tissue
Function: Regulate blood flow to specific regions via vasoconstriction and vasodilation
Diameter: 0.1–10 mm
Muscular arteries are the primary regulators of blood distribution, responding to neural and hormonal signals.
3. Arterioles
Location: Terminal branches before capillary beds
Structure: Thin walls, 1–2 layers of smooth muscle, minimal adventitia
Function: Major site of vascular resistance; control blood flow into capillaries and contribute to systemic blood pressure regulation.
Diameter: <30 μm
Arterioles are often referred to as "resistance vessels" due to their critical role in modulating blood pressure and flow.
Quantitative Data: Arterial Pressures
Aorta/Brachial Artery: Systolic ~120–130 mmHg, Diastolic ~70–80 mmHg, Mean ~85–93 mmHg.
Arterioles: Pressure drops significantly, typically 35 mmHg at the entrance to capillary beds.
Arterial Wall Histology
The tunica media in arteries is rich in smooth muscle and elastic fibers, allowing for both strength and flexibility. The internal and external elastic laminae are prominent in larger arteries, providing additional resilience.
Clinical Relevance: Arterial Diseases
Atherosclerosis: Plaque buildup in arterial walls, leading to narrowing, reduced elasticity, and risk of heart attack or stroke.
Aneurysm: Localized dilation of an artery due to wall weakness, risk of rupture.
Hypertension: Chronic high blood pressure, often due to increased arterial resistance.
Veins: Structure, Adaptations, and Function
General Features
Veins are vessels that return blood to the heart. Their walls are thinner and less muscular than arteries, reflecting the lower pressure of venous blood. The tunica externa is often the thickest layer, providing structural support and anchoring veins to surrounding tissues.
Veins are frequently located closer to the body surface and are more distensible, acting as capacitance vessels that store a large proportion of the body's blood volume (about 65%).
Venous Valves: Structure and Function
A defining feature of veins, especially in the limbs, is the presence of valves. These are bicuspid (two-cusp) folds of the tunica intima, reinforced with connective tissue and covered by endothelium.
Function: Ensure unidirectional blood flow toward the heart, preventing backflow and pooling, particularly in the lower extremities where gravity opposes venous return.
Mechanisms: The skeletal muscle pump and respiratory pump assist venous return by intermittently increasing pressure and propelling blood past the valves.
Valves are less common or absent in central veins (e.g., vena cava) and veins above the heart, where gravity assists blood flow.
Table 2: Venous Structure and Adaptations
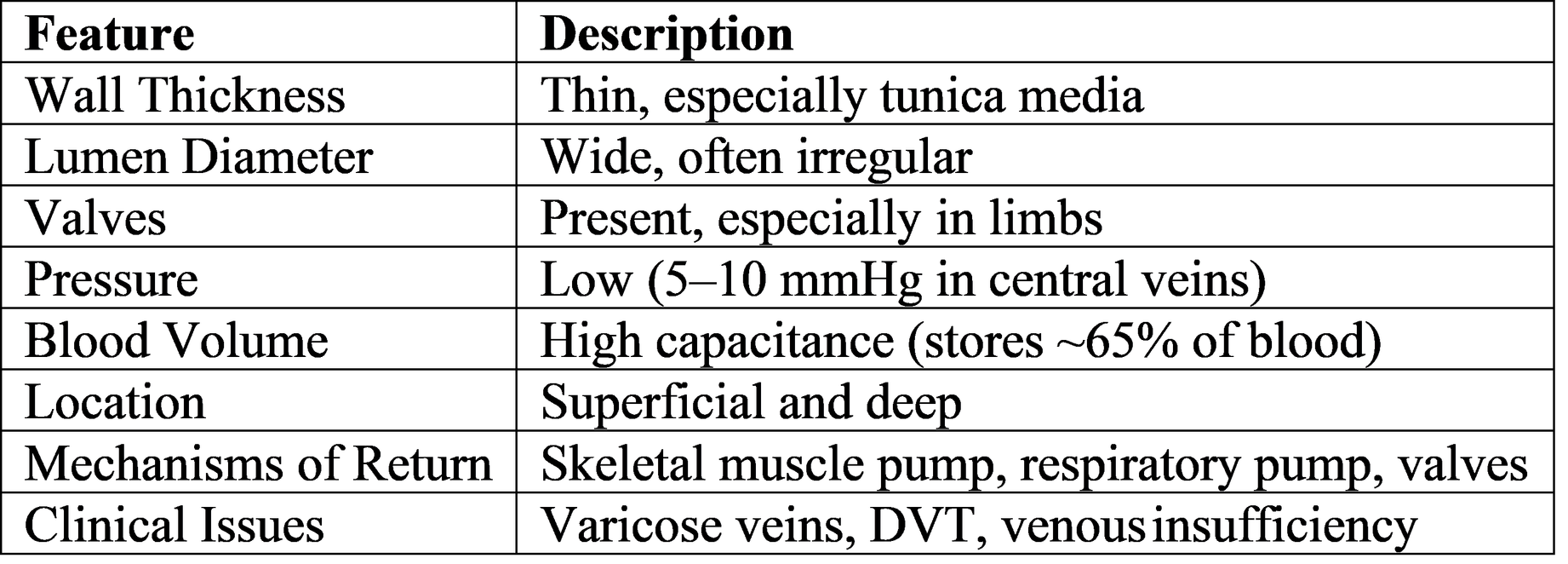
Venous Wall Histology
Veins have all three tunics, but the tunica media is much thinner than in arteries. The tunica externa is often the thickest layer, composed of collagen and some smooth muscle fibers.
Venous Pressure and Hemodynamics
Venous pressure is much lower than arterial pressure, typically 5–10 mmHg in central veins. Blood flow in veins relies on pressure gradients, muscle contractions, and valve function.
Clinical Relevance: Venous Diseases
Varicose Veins: Dilated, twisted superficial veins due to valve failure, leading to pooling and increased pressure.
Deep Vein Thrombosis (DVT): Formation of blood clots in deep veins, risk of pulmonary embolism.
Venous Insufficiency: Chronic failure of venous return mechanisms, leading to edema, skin changes, and ulcers.
Capillaries: Structure, Types, and Exchange Function
General Features
Capillaries are the smallest and most numerous blood vessels, forming extensive networks throughout tissues. Their walls consist of a single layer of endothelial cells supported by a basement membrane, optimizing them for exchange of gases, nutrients, and waste products.
Diameter: 5–10 μm, just wide enough for red blood cells to pass through in single file.
Wall Thickness: One cell thick (endothelium), facilitating rapid diffusion.
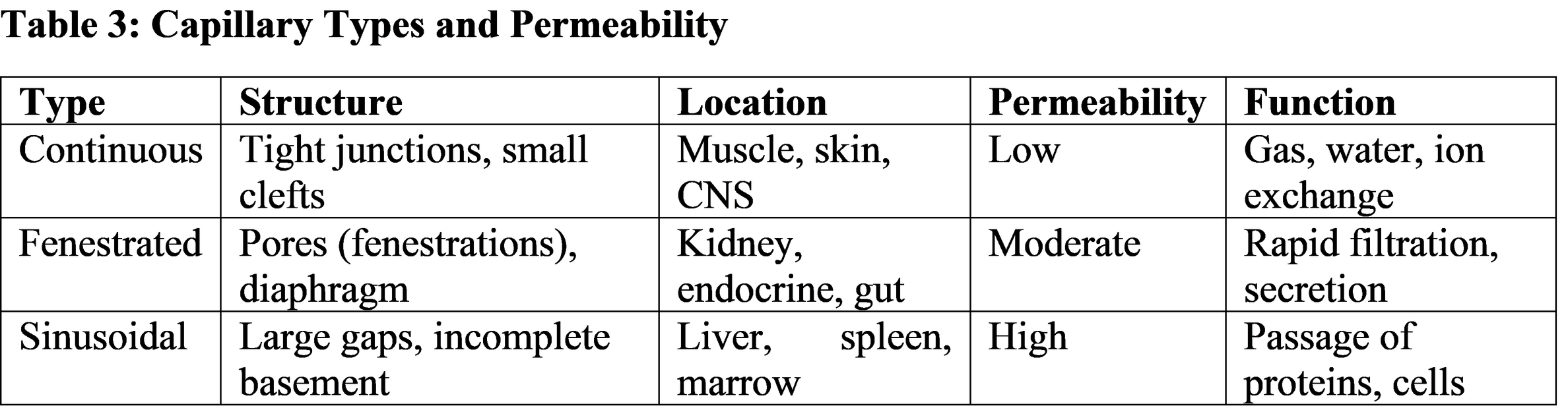
Types of Capillaries
Capillaries are classified based on their permeability and structural features:
1. Continuous Capillaries
Structure: Complete endothelial lining with tight junctions and small intercellular clefts.
Location: Most tissues (muscle, skin, lungs, brain).
Function: Restrict passage to small molecules (water, ions, gases); form the blood-brain barrier in the CNS.
2. Fenestrated Capillaries
Structure: Endothelial cells contain pores (fenestrations) 60–100 nm in diameter, covered by thin diaphragms.
Location: Kidneys (glomeruli), endocrine glands, intestinal villi.
Function: Allow rapid exchange of water, small proteins, and solutes; specialized for filtration and secretion.
3. Sinusoidal (Discontinuous) Capillaries
Structure: Large, irregular lumens; incomplete or absent basement membrane; wide intercellular gaps.
Location: Liver, spleen, bone marrow, lymph nodes.
Function: Permit passage of large molecules, plasma proteins, and even cells; facilitate hematopoiesis and immune surveillance.
Capillary Exchange Mechanisms
Capillary exchange occurs via several processes:
Diffusion: Small, lipid-soluble molecules (O₂, CO₂) pass directly through endothelial cells.
Facilitated Transport: Glucose, amino acids, ions move via specific channels.
Bulk Flow (Filtration and Reabsorption): Driven by hydrostatic and osmotic pressures (Starling forces), fluid moves out at the arterial end (filtration, ~35 mmHg) and is reabsorbed at the venous end (reabsorption, ~18 mmHg), with net movement balanced by lymphatic drainage.
Capillary Bed Regulation
Blood flow through capillary beds is controlled by precapillary sphincters (smooth muscle rings at the entrance to capillaries) and metarterioles. These structures regulate perfusion based on tissue metabolic needs, opening to allow exchange when required and closing to shunt blood directly to venules.
Clinical Relevance: Capillary Disorders
Capillary Leak Syndrome: Increased permeability leads to edema and tissue dysfunction.
Microangiopathies: Thickening or weakening of capillary walls, common in diabetes and hypertension.
Edema: Excess filtration or reduced reabsorption causes fluid accumulation in tissues.
Hemodynamics: Pressure, Flow, and Vessel Properties
Pressure Gradients
Blood flows from regions of higher pressure to lower pressure. The heart generates high pressure in arteries, which drops progressively through arterioles, capillaries, venules, and veins.
Arteries: Highest pressure (systolic ~120–130 mmHg)
Arterioles: Major drop in pressure (to ~35 mmHg)
Capillaries: Pressure falls from ~35 mmHg (arterial end) to ~18 mmHg (venous end)
Veins: Lowest pressure (5–10 mmHg in central veins)
Wall Thickness and Mechanical Properties
Arteries: Thick walls, high elasticity, withstand pulsatile flow.
Veins: Thin walls, high distensibility, accommodate large volumes.
Capillaries: Extremely thin walls, maximize exchange.
Lumen Diameter and Cross-Sectional Area
Arteries: Narrow lumens, maintain pressure.
Veins: Wide lumens, facilitate low-resistance return.
Capillaries: Small individual diameter, but total cross-sectional area is vast, slowing blood flow and optimizing exchange.
Oxygen Content and Direction of Flow
Systemic Circulation:
Arteries: Carry oxygenated blood away from the heart.
Veins: Return deoxygenated blood to the heart.
Pulmonary Circulation:
Arteries: Carry deoxygenated blood to the lungs.
Veins: Return oxygenated blood to the heart.
Exceptions include the pulmonary and umbilical vessels, which reverse the typical oxygenation pattern.
Role in Exchange, Nutrient Delivery, and Waste Removal
Arteries
Deliver oxygen and nutrients to tissues, maintain blood pressure, and regulate flow via vasomotor mechanisms.
Capillaries
Serve as the primary sites for exchange of gases, nutrients, and waste products. Their thin walls and slow blood flow facilitate efficient diffusion and transport.
Veins
Collect deoxygenated blood and metabolic waste from tissues, returning it to the heart for reoxygenation and removal of waste via the lungs and kidneys.
Clinical Relevance: Common Diseases Affecting Vessel Types
Arterial Diseases
Atherosclerosis: Plaque buildup, narrowing, and stiffening of arteries; major cause of heart attacks and strokes.
Aneurysm: Localized dilation due to wall weakness; risk of rupture.
Hypertension: Chronic high pressure damages arterial walls.
Venous Diseases
Varicose Veins: Valve failure leads to pooling, dilation, and tortuosity of superficial veins.
Deep Vein Thrombosis (DVT): Clot formation in deep veins; risk of pulmonary embolism.
Venous Insufficiency: Chronic failure of venous return mechanisms; leads to edema, skin changes, ulcers.
Capillary Disorders
Capillary Leak Syndrome: Excessive permeability, edema, and organ dysfunction.
Microangiopathies: Thickening or weakening of capillary walls, common in diabetes and hypertension.
Edema: Imbalance of filtration and reabsorption.
Quantitative Data: Typical Pressures and Diameters
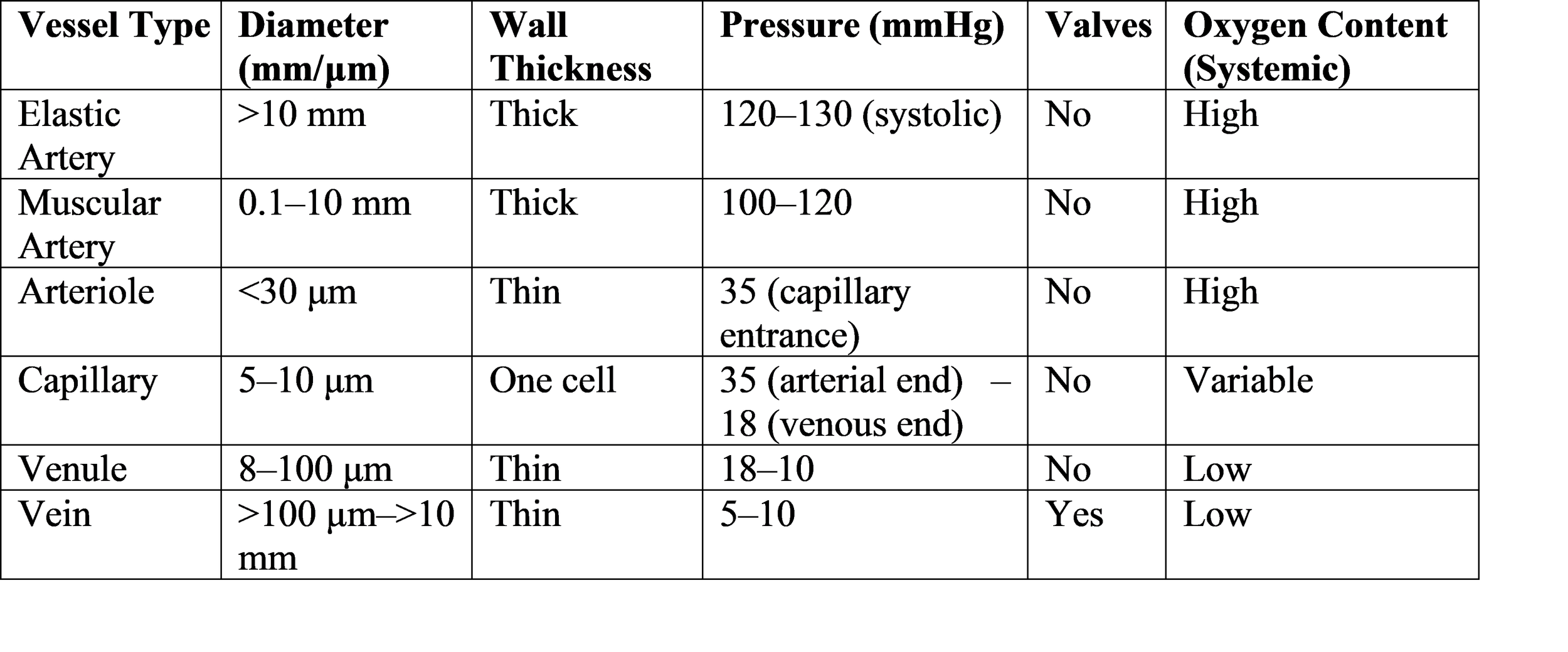
Microscopic and Macroscopic Imaging Resources
Histological slides and diagrams are invaluable for visualizing the differences among vessel types. Key features include:
Arteries: Thick media, prominent elastic laminae.
Veins: Thin media, thick externa, presence of valves.
Capillaries: Single endothelial layer, variable permeability.
This cross-sectional comparison highlights the differences in wall thickness, lumen diameter, and structural adaptations.
Educational Pedagogy: Structuring a 3000-Word Biology Article
A well-structured educational article for biology or medical students should:
Begin with an overview and context.
Progress through detailed structural and functional comparisons.
Integrate tables and images for clarity.
Address clinical relevance and quantitative data.
Conclude with a synthesis of key points and implications for health and disease.
Conclusion
The comparative analysis of arteries, veins, and capillaries reveals a spectrum of structural and functional adaptations that enable the circulatory system to fulfill its vital roles. Arteries are engineered for high-pressure delivery, veins for low-pressure return and volume storage, and capillaries for efficient exchange. Understanding these differences is crucial for interpreting cardiovascular physiology, diagnosing vascular diseases, and appreciating the complexity of human biology.
From the robust walls of elastic arteries to the delicate permeability of sinusoidal capillaries and the valvular safeguards of veins, each vessel type exemplifies the principle of form following function. Clinical conditions such as atherosclerosis, varicose veins, and microangiopathies underscore the importance of vessel integrity and regulation.
For students and practitioners alike, mastery of blood vessel anatomy and physiology provides the foundation for lifelong learning and effective healthcare. The integration of tables, images, and quantitative data enhances comprehension and prepares learners for advanced study and clinical application.
Key Takeaways:
Arteries: Thick-walled, high-pressure vessels; deliver oxygenated blood (except pulmonary arteries); no valves; prone to atherosclerosis and aneurysm.
Veins: Thin-walled, low-pressure vessels; return deoxygenated blood (except pulmonary veins); contain valves; susceptible to varicose veins and DVT.
Capillaries: Single-cell walls; sites of exchange; variable permeability; disorders include microangiopathies and edema.
By appreciating the unique characteristics and clinical relevance of each vessel type, students gain a holistic understanding of the circulatory system and its central role in health and disease.
References
1. Guyton AC, Hall JE. Textbook of Medical Physiology. 14th ed. Philadelphia: Elsevier; 2021.
2. Standring S, editor. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. London: Elsevier; 2021.
3. Mescher AL. Junqueira’s Basic Histology: Text and Atlas. 16th ed. New York: McGraw-Hill Education; 2021.
4. Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 8th ed. Philadelphia: Wolters Kluwer; 2018.
5. Ganong WF, Barrett KE. Review of Medical Physiology. 26th ed. New York: McGraw-Hill Education; 2023.
6. Ross MH, Pawlina W. Histology: A Text and Atlas. 8th ed. Philadelphia: Wolters Kluwer; 2020.
7. Boron WF, Boulpaep EL. Medical Physiology. 3rd ed. Philadelphia: Elsevier; 2017.
8. Tortora GJ, Derrickson BH. Principles of Anatomy and Physiology. 16th ed. Hoboken: Wiley; 2021.
9. Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 10th ed. Philadelphia: Elsevier; 2020.
10. Levick JR. An Introduction to Cardiovascular Physiology. 6th ed. London: Hodder Arnold; 2018.