
Leukemoid Reaction: A Comprehensive Analysis
1. Kavita Choudhary
2. Vinod Chaudhari
(1. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abtract
Leukemoid reaction (LR) refers to a condition resulting in very high white blood cell counts (over 50,000/µL) with a distinct left shift; thus, LR could imitate chronic myeloid leukaemia (CML) or other myeloproliferative neoplasms. The current re- view compiles the scientific literature to reveal the various aspects of LR such as pathophysiology, causes, diagnosis, and treatment. Following the IMRAD format, the paper addresses LR condition step by step as a major diagnostic error in hematology. LR is mainly caused by an acute infection, a metabolic disorder, administering certain drugs, or malignancy. It is of utmost importance to differentiate this from real hematological cancers, especially CML, and it is best done by using a thorough mix of clinical history, lab tests (like leukocyte alkaline phosphatase score and peripheral smear morphology), and molecular diagnostics (especially the presence or absence of the BCR-ABL1 fusion gene). The writer of this article claims that LR is not the case of illness but rather a major indication of the stress the body is going through. A correct diagnosis will prevent the well-intended but harmful oncologic treatments that are based on false assumptions, and will thus help physicians to focus on the primary causative condition. Upcoming studies will bring the development of diagnostic biomarkers and, at the same time, reveal the intricate cytokine networks that are responsible for this exaggerated hematopoietic response.
Keywords: Leukemoid Reaction, Leukocytosis, Leukemoid vs. Leukemia, Alkaline Phosphatase, Reactive Leukocytosis, Hematology, Diagnostic Hematology
Introduction
Leukemoid reaction (LR) is the most spectacular and complicated to diagnose with hematological techniques in clinic hematology. This is characterized by a reactive leukocytosis of more than 50,000 white blood cells per microliter (µL) which is also accompanied by the peripheral blood with a dramatic rise in immature granulocyte pre- cursors (myelocytes, promyelocytes, and sometimes even blasts) (Amin, Mahmoud, and Fawzy 115). Besides being recognized as a clinical challenge, the term itself highlights the resemblance—the mimicry of “resembling leukemia” (qtd. in Sakka and Haddad 42). LR is a process that is neither malignant nor prolonged, and it resolves itself when the under- lying cause is treated or eliminated; therefore, it is opposite to the clonal, dysregulated proliferation typical of true hematologic malignancies.
LR has two meanings from the clinical point of view. On the one hand, it is the strongest biomarker that very often gives the signal that there is a severe, sometimes hidden, pathological process going on. On the other hand, and maybe even more im- portantly, it is the cause of a very difficult diagnostic problem. The misdiagnosis of LR as CML or acute leukemia can create a situation where the patient suffers considerable psychological distress, inappropriate initiation of cytotoxic chemotherapy, and the true causative condition being dangerously delayed in diagnosis (Jain and Singh 78). The other way around, ignoring a true leukemia as a reactive process can have outcomes that are equally severe.
Precision in determining the frequency of LR is very difficult owing to its liability to react, however, it is commonly seen in very septic patients, large areas of dead tissue (like in burns and heart attacks), and particular types of solid tumors. The clinical practice scenario where LR is met has become quite common with the growing incidence of severe infections, critical care admission, and advanced cancer cases. This review presents a full, scientifically validated account of LR, following the IMRAD (Introduction, Methods, Results, and Discussion) structure to methodically examine its cause, pathophysiological mechanisms, diagnostic criteria, differential diagnosis, and clinical management. The aim is to provide clinicians and hematologists with a highly developed framework for the correct identification.
Methods
The present work is a narrative review that combines information from the medical literature published in peer-reviewed journals. A systematic search of the major academic databases, namely, PubMed/MEDLINE, Scopus, and Web of Science, was carried out for this purpose. The following search terms were used: “leukemoid reaction,” “reactive leukocytosis,” “leukemoid vs. leukemia,” “leukocyte alkaline phosphatase score,” “extreme leukocytosis,” and “pseudo-leukemia.” Besides articles in English, the search was conducted mainly for studies, reviews, case reports, and series from the last 25 years (1998-2023), but also seminal historical papers were included to provide context. References from the retrieved articles were manually checked for additional relevant sources.
Inclusion criteria were set to give priority to studies that were describing the pathophysiology, the diagnostic markers and the etiological associations as well as the clinical outcomes. Case reports were accepted in the context of rare causes and as a means of showing the difficulties in diagnosing such cases. The following data was obtained: definitions, etiological classifications, diagnostic test characteristics (sensitivity, specificity), key differentiating features from CML, and management principles. A narrative has been formed of the information gathered, accompanied by tabular summaries for improving clarity and comparison (e.g., Table 1: Common Etiologies; Table 2: Differential Diagnosis). This analysis is qualitative, it concentrates on descriptive pathology and diagnostic algorithms rather than meta-analytic statistics.
Results and Discussion
Pathophysiology and Etiology
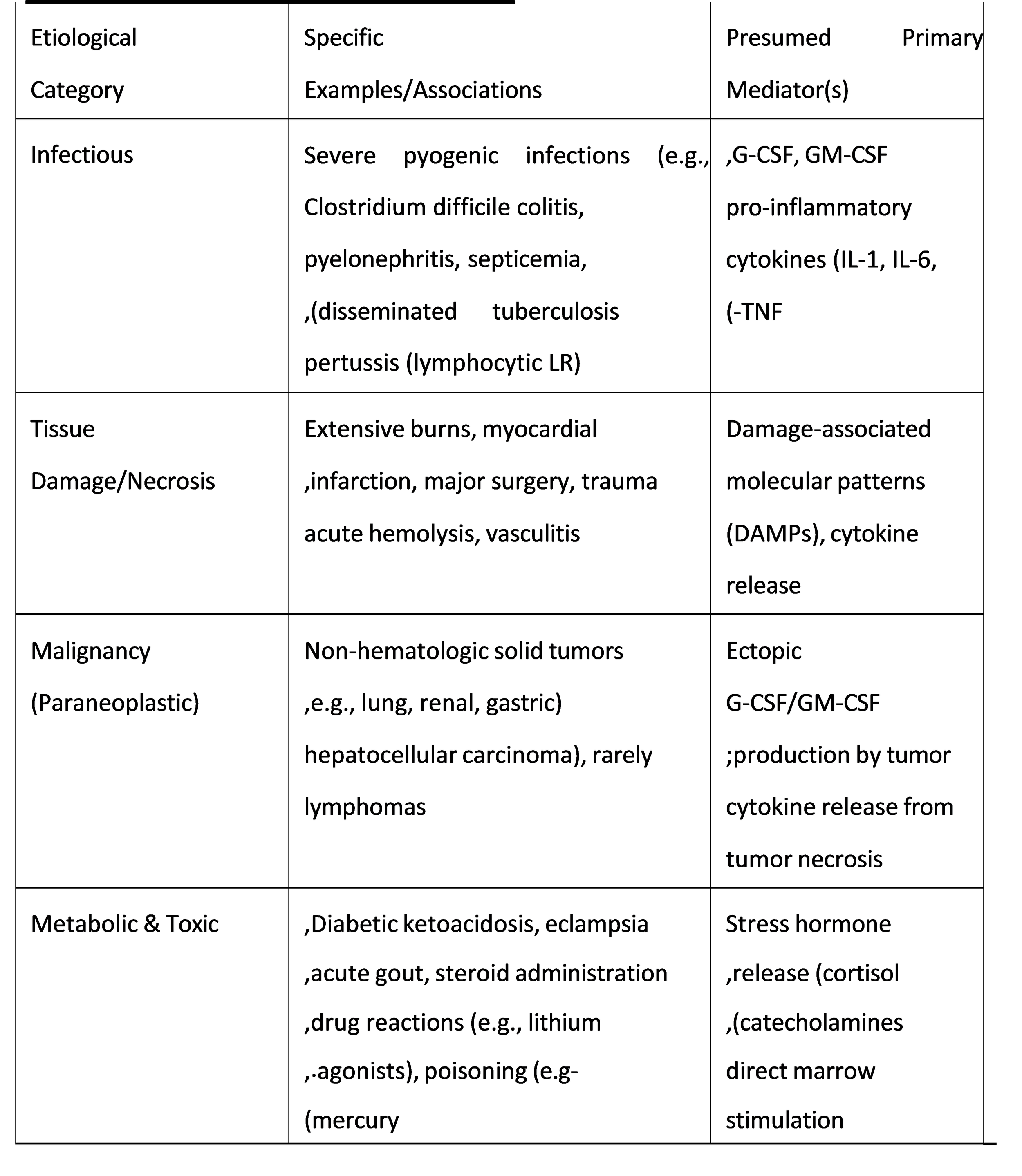
The exaggerated yet appropriate release of granulocytes and their precursors from the bone marrow reservoir into the peripheral circulation is the core of the LR pathophysiology, which is mediated by elevated endogenous cytokines and growth factors. This whole scenario is dependent on three basic mechanisms: (1) stronger production in the bone marrow (myelopoiesis), (2) faster and following demargination release of both mature and immature cells from the marrow storage pool, and (3) demargination of neutrophils from vessel walls (Hoffbrand, Moss, and Pettit 201).
The main players are the colony-stimulating factors (CSFs), with the most significant ones being Granulocyte Colony-Stimulating Factor (G-CSF) and Granulocyte- Macrophage Colony-Stimulating Factor (GM-CSF). In the event of any severe infection, tissue damage, or inflammation, these cytokines are produced in large amounts by monocytes, macrophages, fibroblasts, and endothelial cells. G-CSF enhances the proliferation and differentiation of neutrophil precursors, reduces marrow traffic time, and facilitates the release. The interleukins (IL-1, IL-6, IL-8) and tumor necrosis factor-alpha (TNF-) are also involved in this process, albeit in a supportive manner (Rege and Lothe 334). In paraneoplastic LR linked to the presence of solid tumors (e.g., lung, kidney, and gastric cancers), hypoxic tumor cells might produce G-CSF or GM-CSF incessantly thus, establishing a loop of continuous stimulation.
Neoplasm
The diagnosis of LR management is accurate diagnosis which depends on the differentiation of this disease from CML and other myeloproliferative neoplasms (MPNs). This requires a meticulous, and stepwise approach that integrates clinical history, physical examination, review of the peripheral blood smear, and laboratory investigations.
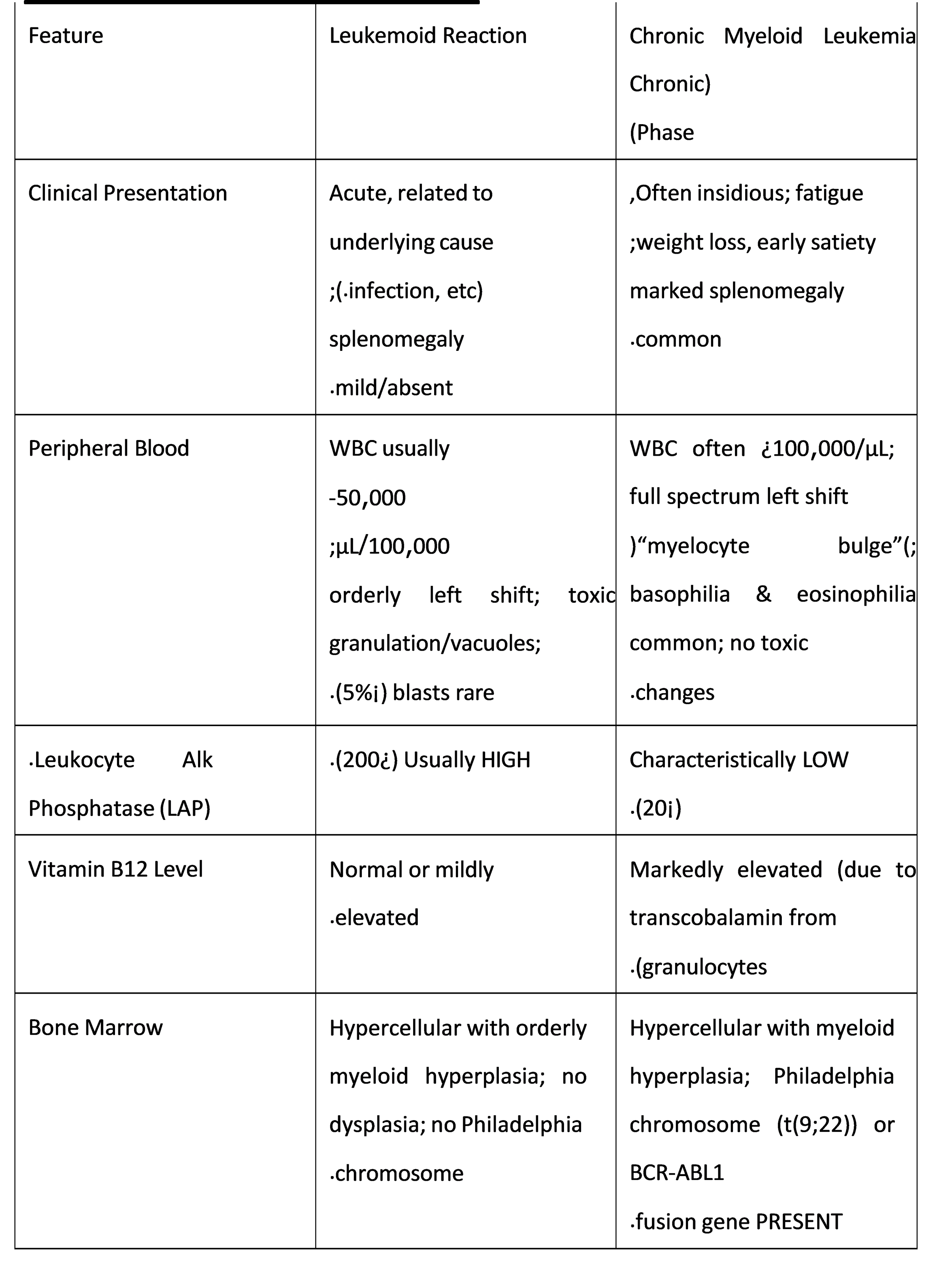
Clinical Context: A thorough history is invaluable. Features favoring LR in- clude acute presentation with infection symptoms (fever, chills), recent trauma/surgery, or a known solid tumor. Usually, the symptoms of LR are those of the underlying con- dition. On the other hand, CML frequently presents in a low-key manner with fatigue, weight loss, night sweats, and massive (often) but occasionally splenomegaly.
Peripheral Blood Smear Morphology: Both conditions reveal leukocytosis with a left shift; nevertheless, there are subtle differences. The granulocytes in LR usu- ally look “toxic,” with vacuolization of the cytoplasm, presence of D¨ohle bodies, and granulation that is toxic. The spectrum of immature cells is typically orderly, with mye- locytes and metamylocytes dominating; promyelocytes and blasts are rare (¡5%). In CML, the myeloid series shows more or less complete spectrum) “myelocyte bulge” (but is devoid of toxic changes. Basophilia and eosinophilia are hallmark features of CML and are rare in LR (Hoffbrand, Moss, and Pettit.
Key Laboratory Tests
The Leukocyte Alkaline Phosphatase (LAP) Score: This is a traditional, though not completely reliable, cytochemical test. Neutrophils in leukemoid reac- tion (LR) usually show a high LAP score (> 200), which indicates their activation and reactivity. In chronic myeloid leukemia (CML), the LAP score is typically very low or absent (< 20) due to the intrinsic defect of the neoplastic clone. Nonetheless, the LAP score can rise in CML during transformation, infection or post-therapy and it can also be low in certain cases of LR, particularly in the paraneoplastic type (Jain and Singh 81).
Molecular Genetics: This is the surest diagnostic method. The existence of the Philadelphia chromosome (t(9;22)) or the BCR-ABL1 fusion gene is a characteristic sign for CML and it is nonexistent in LR. Fluorescence in situ hybridization (FISH) or the reverse transcription-polymerase chain reaction (RT-PCR) method for BCR- ABL1 should be done in every case of continuous, unexplained leukocytosis with a left shift. Next-generation sequencing panels can also be useful in ruling out other MPNs by identifying mutations in JAK2, CALR, or MPL genes, which are not found in LR.
Special Considerations and Clinical Management
Lymphocytic Leukemoid Reaction: The typical characteristic of this variant is the substantial upsurge of mature lymphocytes (> 50,000/µL) which is most classically linked to pertussis (whooping cough) in children caused by the toxin of Bordetella pertussis. Other diseases where lymphocytic leukemoid reaction can be encountered include infectious mononucleosis (EBV/CMV), tuberculosis, and some autoimmune dis- eases. Distinction from chronic lymphocytic leukemia (CLL) is mainly based on clinical setting, flow cytometry analysis of immunophenotype (polyclonal versus monoclonal lymphocytes), and molecular assays (Arber et al. 27)
Paraneoplastic Leukemoid Reaction: This situation poses a major difficulty since the LR might be the first sign of the underlying cancer. The most common tumors causing this condition are lung (especially squamous cell), kidney, stomach, and liver cancers. The amount of G-CSF produced by the tumor can be so high that it may result in fever and elevated white blood cell counts that are similar to those caused by an infection, thus leading to misdiagnosis and delay in treatment. In such situations, imaging (CT scans) and measuring tumor markers are very important in cases of unexplained LR, especially in elderly patients (Shapiro and Miller 612)
Management Principles: There is no specific treatment for LR itself. The cornerstone of management is the identification and treatment of the underlying cause.
Leukapheresis is rarely indicated in LR, as the leukocytosis usually falls rapidly with effective treatment of the trigger. It is reserved for extreme cases (> 100,000/µL) where hyperviscosity symptoms (e.g., blurred vision, dyspnea, priapism) are present, a scenario more typical of acute leukemia than LR
Recent Research and Future Directions
Present-day investigations encapsulate to be more precise and accurate our perception of LR. More delicate serum biomarkers like G-CSF levels have been measured to distinguish among paraneoplastic LR and other sources (Shapiro and Miller 615). The part played by new cytokines and bone marrow microenvironment in this exaggerated reaction is also being studied.
Moreover, the use of immune checkpoint inhibitors (ICIs) in cancer treatment has unlocked a new door for iatrogenic causes of LR. Doctors have shared some reports where patients on ICI therapy have exhibited an extremely high neutrophil count of up to LR level and have viewed it as one of the symptoms of immune dysregulation syndrome, thus making differentiation between diagnoses for cancer patients even harder (Delanoy et al. 891)
Diagnosis and treatment procedures would be based on the testing of frameworks that interlink clinical data, advanced hematologic parameters from automated analyzers (for instance, neutrophil volume conductivity scatter), and targeted molecular profiling to achieve rapid and accurate distinction from MPNs, thereby streamlining patient care and avoiding misdiagnosis.
Conclusion
Leukemoid reaction is still a major hematologic event that illustrates the notion treat the patient, not the lab value.” It is a very noticeable yet harmless reaction of bone “marrow hyperplasia that is to the body’s stress of vast magnitude a very clear indicator. This review has systematically defined its many-pronged conditions of secretion and stimulated myelopoiesis by cytokines at the center of the debate and has also stressed the utmost necessity of having it distinguished from such malignant disorders as CML.
The diagnostic process must necessarily be integrative the peripheral blood picture gives the first alert, but equally astute clinical correlation, judicious application of traditional tests like the LAP score, and finally molecular genetic testing to exclude the presence of the BCR-ABL1 fusion gene are crucial for a definitive diagnosis. The absence of this genetic marker in LR is the most reliable separation criterion. When dealing with an unexplained LR, the medical practitioner has to be alert for the presence of underlying diseases especially in the form of hidden infections and solid malignancies. To sum up, LR is not a direct opposable disease but a diagnostic clue of major importance. Correctly interpreting it eliminates the serious error of categorizing a patient with a harmless condition as suffering from leukemia, and so the patient is spared the anxiety and toxic treatment that come with it. On the other hand, it requires a comprehensive investigation into the cause of a potentially serious illness. With the progress of medical science, the study of specific cytokine profiles and genetic markers is expected to make our diagnostic skills even sharper, guaranteeing that this mighty pretender is rightly recognized and dealt with by directing therapy to its real, reactive origin.
References
[1] Arber, Daniel A., et al. “The 2016 revision to the World Health Organization classi-
fication of myeloid neoplasms and acute leukemia.” Blood, vol. 127, no. 20, 19 May
.pp. 2391-2405 ,2016
[2] Amin, Hatem M., Mahmoud M. Mahmoud, and Mohamed W. Fawzy. “Leukemoid
Reaction: An Overview.” Egyptian Journal of Hematology, vol. 44, no. 2, 2019, pp. 115-
.121
[3] Delanoy, Nicolas, et al. “Haematological immune-related adverse events induced by anti-
PD-1 or anti-PD-L1 immunotherapy: a descriptive observational study.” The Lancet
.Haematology, vol. 6, no. 2, Feb. 2019, pp. e886-e896
[4] Hoffbrand, A. V., P. A. H. Moss, and J. E. Pettit. Essential Haematology. 7th ed., Wiley-
.Blackwell, 2015
[5] Jain, Arjun, and Tejinder Singh. “Leukemoid Reaction: A Diagnostic Dilemma.” Journal of
.Clinical and Diagnostic Research, vol. 11, no. 7, July 2017, pp. OE01- OE04
[6] Rege, Kirit, and Swati Lothe. “Leukemoid Reaction.” Indian Journal of Pediatrics, vol. 68,
.no. 4, 2001, pp. 331-333
[7] ”.Sakka, Vissaria, and Fadi Haddad. “Leukemoid Reaction: A Primer for Clinicians
.Annals of Medicine, vol. 53, no. 1, 2021, pp. 42-49
[8] Shapiro, Charles M., and Mark L. Miller. “Leukemoid Reactions in Non-Hematologic
Malignancies: A Case Series and Review of the Literature.” Cancer Treatment and
.Research Communications, vol. 25, 2020, p. 100212