
Emergency Condition: Pulmonary Hemorrhages and Hemoptysis
1. Dr. Kurmanaliev Nurlanbek
2. Venkatesh Athisesan,
Dongre Rohit Tejrao, Jadhav Ganesh Dnyaneshwar, Kannan Saradha Poorvaja,
Lingdale Muktai Santosh, Modak Bhushan Uttamrao, Mohamed Rasheed Nashreen,
Mohammad Adil, Murugan Vaishnavi, Sandhiya Sureshkumar,
Tripathi Vivek, Zareen Khan, Yadav Abhishek Babulal,
Gupta Vivek, Rajendran Devadharshini
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Respiratory emergencies represent some of the most high-stakes scenarios in clinical medicine. This article examines the etiology, pathogenesis, and management of three life-threatening conditions: pulmonary hemorrhage (and its clinical hallmark, hemoptysis), spontaneous pneumothorax, and acute cor pulmonale. By synthesizing physiological mechanisms with practical clinical examples, we explore the transition from aggressive stabilization to the nuanced application of palliative care in advanced disease. The goal is to provide a detailed roadmap for identifying these conditions and managing them with both technical precision and human empathy.
Introduction
The respiratory system is the body’s primary interface with the external environment, and its failure is often instantaneous and catastrophic. When a patient presents with “emergency” respiratory distress, the clinician must quickly differentiate between vascular rupture (hemorrhage), structural collapse (pneumothorax), and pump failure (cor pulmonale). While modern medicine offers advanced interventions like bronchial artery embolization and video-assisted surgery, there is a growing recognition that for many patients—particularly those with end-stage chronic disease—the “emergency” is not just a physiological crisis but a profound moment of human suffering that requires a palliative approach.
Context and Background: The Vulnerable Lung
The lungs are unique because they receive the entire cardiac output through a low-pressure system (pulmonary circulation) while being nourished by a high-pressure system (bronchial circulation). This dual supply is at the heart of many emergencies.
Pulmonary Hemorrhage often arises from the high-pressure bronchial arteries, which are prone to rupture when chronically inflamed. Pneumothorax represents a failure of the pleural seal, where the delicate balance of negative pressure that keeps the lungs inflated is disrupted.
Acute Cor Pulmonale is the sudden “bottlenecking” of the heart, where the right ventricle fails because it cannot push blood through obstructed or constricted pulmonary vessels.
Pulmonary Hemorrhages and Hemoptysis: Hemoptysis—the coughing up of blood—is one of the most frightening symptoms a human can experience.
Etiology and Pathogenesis
The most common causes of massive hemoptysis (defined as >300–600 mL in 24 hours) include:
Infectious: Tuberculosis (historically the leader), bronchiectasis, and necrotizing pneumonia.
Malignancy: Bronchogenic carcinoma eroding into a vessel.
Vascular/Autoimmune: Vasculitis (e.g., Granulomatosis with polyangiitis) or Goodpasture syndrome, where the immune system attacks the alveolar-capillary membrane.
Clinical Management
The primary goal is airway protection. In massive hemorrhage, patients do not typically die from blood loss (exsanguination) but from drowning (asphyxiation).
The Gold Standard: Opioids
Opioids are the first-line pharmacological treatment for refractory dyspnea. They work by reducing the perception of breathlessness, blunting the ventilatory response to hypoxia/hypercapnia, and acting as mild pulmonary vasodilators.
Oral Morphine
Opioid-Naïve Patients: Start with 2.5 mg to 5 mg of immediate-release (IR) morphine every 4 hours.
Already on Opioids (for pain): Increase the total daily dose by 25% to 50%.
PRN (As Needed): Provide a “rescue dose” equal to roughly 10% of the total daily dose or the standard starting dose (2.5 mg) every 1–2 hours for breakthrough episodes.
Parenteral Morphine (IV/Subcutaneous)
For patients unable to swallow or in acute distress:
Starting Dose: 1 mg to 2 mg IV or Sub-Q every 4 hours.
Continuous Infusion: In the final hours of life, a syringe driver starting at 10 mg to 20 mg over 24 hours may be used, titrated upward based on clinical response.
2. Managing the Anxiety Cycle: Benzodiazepines
Anxiety is both a cause and a consequence of dyspnea. Benzodiazepines do not improve the respiratory drive but are highly effective at breaking the “panic-breathlessness” loop.
Reducing “Death Rattle” (Secretions)
Antimuscarinics are used to dry up oronasal and bronchial secretions that the patient can no longer clear, which can cause a distressing “rattling” sound for family members.
Glycopyrrolate: 0.2 mg Sub-Q or IV every 4–6 hours (Preferred as it does not cross the blood-brain barrier, reducing the risk of delirium).
Hyoscine Butylbromide (Buscopan): 20 mg Sub-Q every 4 hours or via syringe driver (60–120 mg/24 hours).
Adjunctive Therapies
Corticosteroids: (e.g., Dexamethasone 4 mg to 8 mg daily) to reduce peritumoral edema or inflammation in COPD/ILD.
Oxygen Therapy: Indicated only if the patient is hypoxic and reports symptomatic relief. If the patient is not hypoxic, a simple electric fan blowing cool air across the face (trigeminal nerve stimulation) is often as effective as supplemental oxygen. Positioning: Place the patient “bleeding side down” to prevent blood from flooding the healthy lung Intervention: Bronchial Artery Embolization (BAE) is the gold standard for stopping the flow.
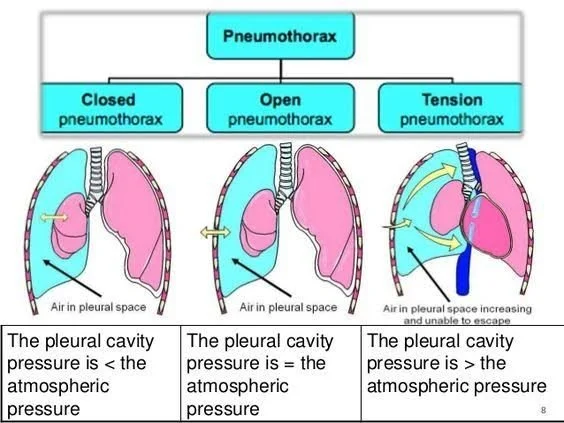
Spontaneous Pneumothorax: A pneumothorax occurs when air enters the pleural space, causing the lung to pull away from the chest wall.
Etiology and Pathogenesis
Primary Spontaneous Pneumothorax (PSP): Occurs in healthy individuals, often tall, thin young men. It is usually caused by the rupture of small "blebs" (air blisters) at the top of the lung.
Secondary Spontaneous Pneumothorax (SSP): Occurs in patients with existing disease, like COPD or Cystic Fibrosis. This is far more dangerous because these patients have no respiratory reserve.
The Emergency: Tension Pneumothorax
In a "tension" scenario, air enters the pleural space but cannot escape. This creates a one-way valve effect that shifts the heart and compresses the great veins, leading to rapid cardiovascular collapse.
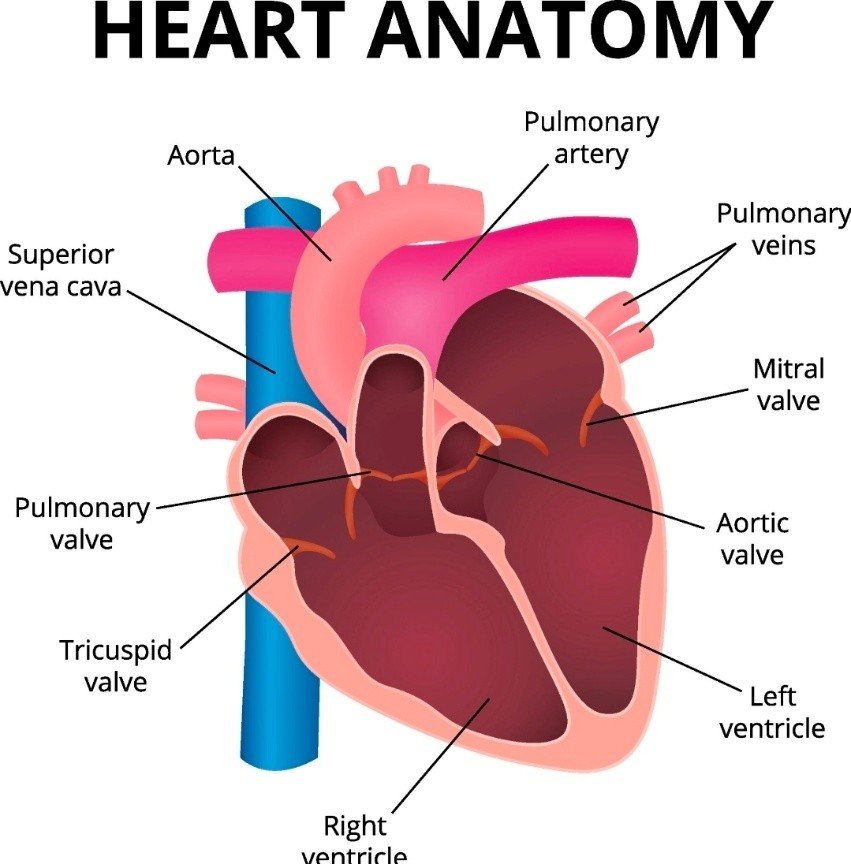
Acute Cor Pulmonale
Cor pulmonale is “heart failure caused by the lungs.”
Pathogenesis
The right ventricle (RV) is built to be a high-volume, low-pressure pump. In acute cor pulmonale, a sudden rise in pulmonary vascular resistance (most commonly from a massive Pulmonary Embolism) forces the RV to work against a wall. The thin-walled RV dilates rapidly, fails, and can no longer deliver blood to the left side of the heart, leading to a drop-in blood pressure and shock.
Clinical Examples
The Hemoptysis Case: A 65-year-old smoker presents with 400ml of bright red blood. Management focuses on BAE and ruling out lung cancer.
The Pneumothorax Case: A 19-year-old student feels sharp chest pain while sitting in class. A simple chest tube (thoracostomy) resolves the collapse.
The Cor Pulmonale Case: A post-surgical patient suddenly becomes short of breath and faints. Ultrasound shows a dilated right heart, confirming a massive PE.
Palliative Care in Respiratory Emergencies
When "fixing" the lung is no longer possible, the focus shifts to dyspnea management.
Opioids: Low-dose morphine is the most effective tool for reducing the "air hunger" sensation.
Anxiolytics: Benzodiazepines help break the cycle of "breathlessness-anxiety-more breathlessness."
Environmental: Simple things like a cool fan blowing on the face can physiologically reduce the sensation of dyspnea.
Conclusion
Emergency respiratory conditions require a dual-track mind: the technical ability to stop a bleed or drain a chest, and the human wisdom to know when to shift toward comfort. Whether it is the terrifying sight of hemoptysis or the silent failure of cor pulmonale, the goal remains the same—to restore the patient's ability to breathe, or to ensure their final breaths are peaceful.
References
1. MSD Manual Professional Edition: Hemoptysis and Pulmonary Disorders.
2. StatPearls: Spontaneous Pneumothorax Management and Diagnosis.
3. Cleveland Clinic: Cor Pulmonale Symptoms and Causes.
4. Marie Curie Knowledge Zone: Managing Breathlessness in Palliative Care.