
Emerging Threats and Future Perspectives of Public Health in Kyrgyzstan
1. Kalybekova K.D.
2. Faizan Mohd
Karangale Om
Yadav Yogesh
(1. Teacher, Public Health Dept., International Medical Faculty, Osh State University, Osh, Kyrgyzstan.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyzstan.)
Abstract
Background: Kyrgyzstan, a lower-middle income country in Central Asia with a population of 6.63 million, faces a complex and evolving public health landscape characterised by a dual burden of communicable and non-communicable diseases (NCDs), significant environmental hazards, and systemic health system constraints. Despite notable progress since independence in 1991—including improvements in life expectancy, child mortality, and universal health coverage—critical threats persist and new ones are emerging.
Objectives: This narrative review synthesises the most current data from the World Health Organization (WHO), UNICEF, the World Bank, the WHO European Observatory on Health Systems and Policies, and peer-reviewed literature to identify Kyrgyzstan's major emerging public health threats and outline future perspectives for health system strengthening.
Key Findings: Non-communicable diseases account for 83% of all deaths. Tuberculosis incidence remains the highest in the WHO European Region at 112 per 100,000 population (2023 data). Air pollution in the capital Bishkek exceeds WHO PM2.5 guidelines by nearly sevenfold. Out-of-pocket health expenditure constitutes 40.7% of total health spending, creating catastrophic financial risk. Antimicrobial resistance, HIV/TB co-infection, climate-sensitive diseases, and mental health service gaps represent emerging challenges requiring urgent multi-sectoral responses. Maternal mortality has declined by only 7% since 1990, substantially lagging the regional average.
Conclusions: Sustained investment in primary healthcare, targeted disease control programmes, environmental health policy reform, and a strengthened health financing architecture are essential for Kyrgyzstan to achieve its 2030 health goals under the national Healthy Person – Prosperous Country strategy (2019–2030). Reducing out-of-pocket payments, expanding health insurance coverage, and scaling evidence-based interventions are the most critical near-term priorities.
Keywords: Kyrgyzstan; public health; tuberculosis; non-communicable diseases; air pollution; antimicrobial resistance; health system reform; Central Asia; health financing; maternal health
1. Introduction
Kyrgyzstan is a landlocked lower-middle income country in Central Asia, bordering China, Kazakhstan, Tajikistan, and Uzbekistan. With a population of approximately 6.63 million as of 2022 and a projected 42% increase by 2050, Kyrgyzstan presents a unique demographic and epidemiological context that shapes its public health priorities.¹
Since gaining independence from the Soviet Union in 1991, Kyrgyzstan has implemented four consecutive national health reform programmes: Manas (1996–2005), Manas Taalimi (2006–2011), Den Sooluk (2012–2018), and the current Healthy Person – Prosperous Country programme (2019–2030).²⁰ These reforms have yielded measurable gains: life expectancy at birth rose from 66.0 years in 2000 to 71.2 years in 2021, and the Universal Health Coverage (UHC) Service Coverage Index improved from 52 in 2000 to 70 in 2019.⁷ Under-five child mortality declined from 50 per 1,000 live births in 2000 to 16.5 per 1,000 live births in 2023, as documented by UNICEF's Multiple Indicator Cluster Survey (MICS 2023).⁴
Despite this progress, Kyrgyzstan faces a formidable set of persistent and emerging public health threats: a high burden of non-communicable diseases, the highest tuberculosis incidence rate in the WHO European Region, rising HIV/AIDS burden, escalating antimicrobial resistance (AMR), severe urban air pollution, the growing health impacts of climate change, fragile maternal and child health indicators—particularly in rural areas—and a health financing model that exposes households to catastrophic out-of-pocket expenditure.³ This narrative review systematically examines these threats using the most recent official datasets and peer-reviewed evidence, and proposes evidence-based recommendations for future health system strengthening.
2. Demographic and Health Overview
2.1 Population and Life Expectancy
Kyrgyzstan had a population of 6,630,631 in 2022.¹ Life expectancy at birth in 2021 stood at 71.2 years—a gain of 5.2 years from 66.0 years in 2000—while healthy life expectancy (HALE) increased from 58.7 to 63.4 years over the same period.¹ Despite this progress, both indicators remain substantially below the WHO European Region averages of 76.3 years for life expectancy and 66.0 years for HALE as of 2021.¹
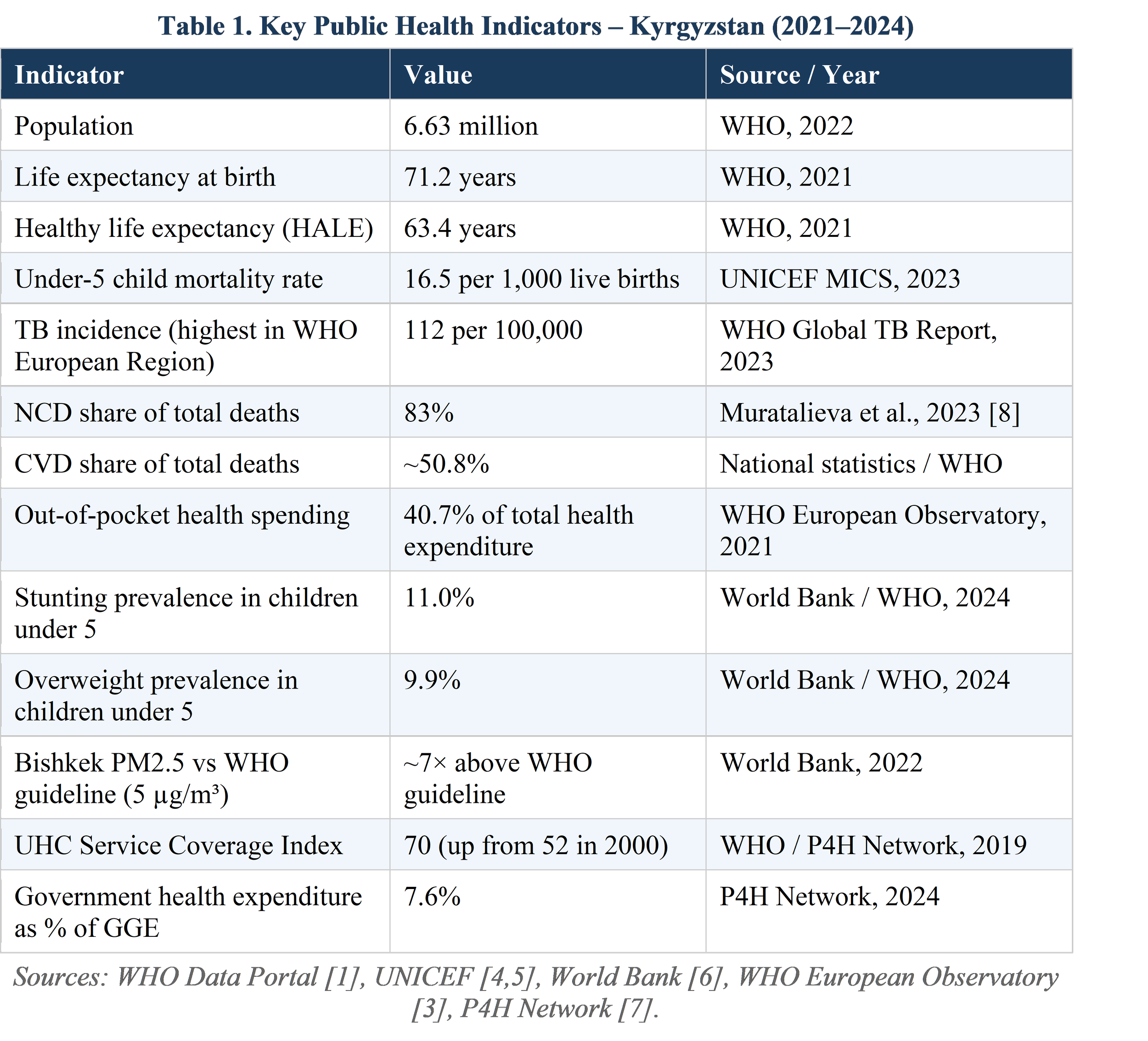
Table 1 presents a summary of key public health indicators for Kyrgyzstan drawn from official sources.
2.2 Burden of Disease
Non-communicable diseases (NCDs) are the primary driver of mortality in Kyrgyzstan, responsible for an estimated 83% of all deaths.⁸ Cardiovascular diseases (CVDs) constitute the single largest cause, accounting for approximately 50.8% of deaths. Among 51 WHO European and Central Asian countries, Kyrgyzstan ranks 3rd highest for CVD mortality in women and 5th highest in men, with over 19,000 CVD-related deaths annually.¹¹
When assessed by Disability-Adjusted Life Years (DALYs)—which capture years of healthy life lost to both premature death and disability—maternal and neonatal disorders and musculoskeletal conditions gain additional prominence beyond their mortality impact. According to the WHO Global Burden of Disease estimates, the leading risk factors driving disease burden in Kyrgyzstan are malnutrition, air pollution, and high blood pressure. ¹
3. Communicable Disease Threats
3.1 Tuberculosis: The Region's Highest Burden Country
Tuberculosis (TB) remains the most acute communicable disease crisis in Kyrgyzstan. According to the WHO Global Tuberculosis Report 2024, Kyrgyzstan recorded an incidence rate of 112 cases per 100,000 population in 2023—the highest TB burden in the entire WHO European Region—surpassing Kazakhstan (70/100,000), Tajikistan (79/100,000), Uzbekistan (57/100,000), and Turkmenistan (49/100,000).¹⁰ Kyrgyzstan is itself listed among the countries on the WHO global high-burden MDR-TB list, along with four other Central Asian states.¹⁰
Multidrug-resistant tuberculosis (MDR-TB) compounds the challenge significantly. As of 2024, WHO reports that over 2.5% of new TB cases and 18% of previously treated cases globally are resistant to first-line anti-TB drugs.¹⁶ MDR-TB—defined by resistance to both isoniazid and rifampicin—necessitates longer, more expensive, and less effective treatment regimens. A prospective analysis of 138 hospitalised MDR-TB patients at the National Referral Centre in Bishkek (January 2020–August 2022) documented pulmonary complications in 23%, malnutrition in 33%, severe anaemia in 17%, and diabetes mellitus comorbidity in 13% of cases—demonstrating the critical intersection of TB with NCDs and nutritional deficiency.⁹
While TB treatment coverage rates in Kyrgyzstan are relatively high, significant gaps persist in access to rapid molecular diagnostics, second-line drug availability, and community-based adherence support. The COVID-19 pandemic further disrupted TB service delivery and contact tracing capacity.³ In April 2025, Kyrgyzstan joined a WHO-led regional initiative aimed at TB elimination in Central Asia by 2030.²
3.2 HIV/AIDS: Growing Burden and Co-infection Risk
HIV/AIDS presents a growing public health concern. Kyrgyzstan's HIV incidence among the population aged 15–24 was reported at 0.10 per 1,000 uninfected individuals in 2024, stable from 2023.¹⁸ As of December 2021, national statistics recorded 725 children living with HIV.⁴ Globally, TB is the leading infectious cause of death among people with HIV, making HIV/TB co-infection a particularly high-priority concern in the Kyrgyz context.¹⁶
The government has made measurable progress toward eliminating vertical (mother-to-child) HIV transmission through mandatory antenatal testing, early antiretroviral therapy initiation, and integration of HIV services into perinatal care.⁴ However, stigma, geographic barriers to services in remote areas, and healthcare workforce capacity gaps remain significant obstacles to universal programme reach.
3.3 Antimicrobial Resistance: An Escalating Systemic Threat
Antimicrobial resistance (AMR) is a rapidly escalating threat. Globally, AMR was associated with approximately 5 million deaths per year as of 2024, making it the third-leading cause of death worldwide.¹⁹ In Kyrgyzstan, a critical contributing factor is that antibiotics remain widely accessible over-the-counter without a prescription, fostering widespread, unsupervised use and accelerating resistance development among common bacterial pathogens.¹³
The overuse of antibiotics for respiratory tract infections in primary care settings is particularly well-documented. International research partners have initiated clinical interventions to address this: the INSTALL project (ClinicalTrials.gov NCT07261969, 2024) is evaluating the use of C-reactive protein (CRP) point-of-care testing and patient information leaflets to optimise antibiotic prescribing in Kyrgyz primary care settings.¹³
3.4 Vaccine-Preventable Diseases: The 2023 Measles Outbreak
In 2023, Kyrgyzstan experienced a significant measles outbreak requiring an emergency public health response. In September 2023, the country received 755,500 doses of measles and rubella vaccine through the Measles and Rubella Partnership. A two-week supplementary immunisation campaign was launched, targeting children aged 9 months to 7 years in Bishkek, Osh, and surrounding regions. Vaccinations were administered at 750 temporary sites and by 60 mobile outreach teams deployed to reach remote communities. The campaign was coordinated by the Republican Centre for Immunoprophylaxis with support from WHO, UNICEF, and the Red Crescent Society of Kyrgyzstan.⁴
This outbreak illustrates the persistent vulnerability arising from immunisation coverage gaps in hard-to-reach populations and the ongoing risk of preventable disease resurgence when routine vaccination programmes are interrupted.
4. Non-Communicable Diseases: The Dominant Mortality Burden
4.1 Cardiovascular Disease
Cardiovascular disease is the leading cause of death in Kyrgyzstan, accounting for over 19,000 deaths annually—approximately 50.8% of all-cause mortality.¹¹ Kyrgyzstan recorded the highest coronary heart disease (CHD) mortality rate in the WHO European Region in 2013 and was the only country in the region with an increasing CHD mortality rate at that time.¹¹ Although ischaemic heart disease mortality decreased by approximately 5% and stroke mortality by over 13% between 2009 and 2019, CVD mortality remains critically elevated by regional standards.¹¹
Behavioural risk factors documented by the WHO STEPwise approach to surveillance (STEPS) include: tobacco use (prevalence 25.7%), harmful alcohol use (31.4%), physical inactivity (83.7% of the population), insufficient fruit and vegetable consumption (74%), and excessive salt use (21% report adding salt to food before eating).⁸ These individual-level risks are compounded by air pollution exposure and hypertension, identified as the leading environmental and biological determinants of disease burden in the WHO Global Health Estimates.¹
4.2 Diabetes, Cancer, and Chronic Respiratory Disease
Beyond CVD, type 2 diabetes mellitus, cancer, and chronic respiratory diseases contribute substantially to the NCD burden. These conditions are increasingly interlinked with rising overweight and obesity prevalence: in 2024, 9.9% of children under five were overweight—an all-time recorded high—according to World Bank-modelled estimates.⁵ Globally, NCDs cause 41 million deaths annually (74% of all deaths), with cardiovascular diseases accounting for 17.9 million deaths, cancers 9.3 million, and chronic respiratory diseases 4.1 million per year.²⁵
The co-occurrence of diabetes mellitus in 13% of hospitalised MDR-TB patients in Kyrgyzstan⁹ highlights the bidirectional relationship between communicable and non-communicable diseases—a critical consideration for integrated care planning.
4.3 Mental Health: A Significant Evidence and Service Gap
Mental health remains a significantly underresourced domain in Kyrgyzstan's health system. No current national population-level prevalence surveys for mental disorders exist, reflecting a fundamental evidence gap that constrains policy formulation and resource allocation. The national Healthy Person – Prosperous Country programme (2019–2030) identifies mental health and well-being as a target area, in alignment with UN Sustainable Development Goal (SDG) 3.4, which calls for a one-third reduction in premature NCD mortality and promotion of mental health by 2030.¹⁵ The absence of a national mental health action plan with dedicated funding, community-based services, and anti-stigma programmes represents a critical gap requiring urgent attention.
5. Environmental and Climate-Related Health Threats
5.1 Urban Air Pollution: A Critical Emergency
Air pollution is the principal environmental risk factor for premature death and ill-health in Kyrgyzstan. In Bishkek, average annual PM2.5 concentrations in 2022 exceeded the WHO guideline value of 5 µg/m³ by nearly sevenfold—among the worst urban air quality situations in the Central Asian and European region.⁶ In recognition of this crisis, in November 2023 the World Bank approved a USD 50 million Kyrgyz Republic Air Quality Improvement Project to support the country in reducing air pollution and mitigating its public health and economic consequences.⁶
Fine particulate matter (PM2.5) drives a broad spectrum of health harm, including acute and chronic respiratory infections, cardiovascular diseases, lung cancer, and premature mortality. A 2023 study on the health and social impacts of air pollution on women and children in Bishkek found exposure levels far above thresholds known to cause major adverse health effects in urban populations.⁴ Prenatal PM2.5 exposure has been shown to impair neurological development and cognitive function, alter fetal and neonatal lung architecture, and predispose individuals to cardiovascular disease in adulthood.⁴
A primary driver of both indoor and outdoor pollution in Kyrgyzstan is the domestic combustion of coal and other solid fuels for heating, which is widespread in Bishkek's peri-urban areas and throughout rural regions. This practice simultaneously elevates household and ambient air pollutant concentrations, creating a year-round health burden with peak severity in winter months.
5.2 Climate Change and Emerging Health Vulnerabilities
Kyrgyzstan is highly vulnerable to climate change given its mountainous topography, dependence on glacial meltwater for agriculture and drinking water, and limited adaptive capacity. Climate change intersects with public health through multiple pathways: increased frequency of extreme heat events that exacerbate CVDs and respiratory morbidity; shifts in disease vector distribution, expanding the geographic range of vector-borne diseases; disruption of clean water access and sanitation infrastructure; and food insecurity arising from changes in agricultural productivity and glacier retreat.¹⁷
WHO's Global Health Estimates database tracks climate change-attributable deaths and DALYs as specific indicators for Kyrgyzstan, reflecting the growing scientific consensus on this nexus.¹⁷ UNICEF supports Kyrgyzstan in developing climate-resilient WASH programmes, community-level preparedness systems, and climate adaptation measures within the health sector.⁴
Malaria, which had been controlled in Kyrgyzstan, experienced a documented resurgence, analysed in a 2023 WHO publication that examined the epidemiological factors driving this re-emergence and proposed evidence-based elimination strategies.² Climate-related changes in temperature and precipitation are among the recognised contributors to shifts in Anopheles mosquito vector habitat.
5.3 Water, Sanitation, and Hygiene (WASH)
Inadequate access to safely managed water, sanitation, and hygiene services continues to affect significant segments of the Kyrgyz population, with the most severe deficits in rural, mountainous, and peri-urban communities. These gaps directly contribute to waterborne diarrhoeal disease—a leading cause of child mortality—and sustain the risk of enteric disease outbreaks. Safe domestic wastewater treatment coverage and basic handwashing facility access are tracked as SDG 6 indicators by WHO and UNICEF and remain below targets across multiple regions of the country.⁴
6. Maternal and Child Health
Maternal and child health represent both notable achievements and persistent vulnerabilities in Kyrgyzstan. Between 1990 and 2018, the country reduced under-five child mortality by 69% and neonatal mortality by 46%, according to a Lancet Global Health analysis.¹² Kyrgyzstan was among the first countries in the eastern WHO European Region to enact legislation protecting, promoting, and supporting breastfeeding. The UNICEF MICS 2023 survey confirms that under-five child mortality fell from 20.0 to 16.5 per 1,000 live births over the five years prior to the survey.⁴
However, significant disparities persist. Mortality rates remain consistently higher in rural areas than in urban ones, with household income and maternal education being strong independent predictors of child survival.⁴ Neonatal mortality—defined as death within the first 28 days of life—now constitutes more than half of all under-five deaths, with preterm birth and low birth weight representing the most critical risk factors. The regional variation in progress is striking: neonatal mortality in Jalal-Abad oblast fell from 29 per 1,000 live births in 2018 to 5 per 1,000 in 2023, demonstrating what targeted intervention can achieve, while highlighting the inequitable distribution of health gains across oblasts.⁴
Maternal mortality presents a particularly concerning picture. Kyrgyzstan's maternal mortality ratio declined by only 7% between 1990 and 2017—from 82 to approximately 76 deaths per 100,000 live births—compared with a 54% reduction recorded across the broader Central Asian region over the same period.¹² Contributing factors include a high adolescent fertility rate (32.4 births per 1,000 women aged 15–19 years in 2018, twice as high in rural versus urban settings), a high total fertility rate (3.3 births per woman in 2018), prevalent anaemia among women of reproductive age, limited access to emergency obstetric care in remote areas, and weak contraceptive coverage.¹² As of 2018, a five-year government programme was established to fund contraceptive access for 50% of women identified at high medical and social risk of maternal mortality.¹²
7. Health System: Financing, Workforce, and Governance
7.1 Health Financing
Kyrgyzstan operates a mandatory health insurance system administered by the Mandatory Health Insurance Fund (MHIF), established in 1996, with compulsory insurance launched on 1 January 1997. The State-Guaranteed Benefits Package (SGBP) provides all citizens with free access to primary and outpatient specialist services, with co-payments required for most inpatient care. However, the scope of publicly funded care is limited: the government covers only 50% of the cost of a restricted list of approximately 70 essential medicines.³ As of 2019, only 69% of the population was enrolled in the MHIF.⁷
Out-of-pocket (OOP) payments constituted 40.7% of total health expenditure in 2021, creating catastrophic financial risk for households—particularly in lower income quintiles.³ While the OOP share has decreased from 51.6% in 2000 to 38.6% in 2019 as a result of mandatory insurance reforms, it remains among the highest in the WHO European Region.⁷ Per capita health expenditure was the lowest in the entire WHO European Region in 2021 and has declined as a proportion of total government spending.³
Domestic general government health expenditure as a share of general government expenditure stood at 7.6%, with a GDP of approximately USD 12 billion in constant 2020 US dollars.⁷ WHO's 2010 World Health Report identified a threshold of 5–6% of GDP in government health spending as necessary for countries to provide a basic package of essential health services, a benchmark Kyrgyzstan has not yet consistently met from public sources alone.
7.2 Health Workforce and Infrastructure
Primary healthcare faces significant structural challenges, particularly in remote and mountainous communities. Shortages of trained medical personnel, limited availability of essential medicines and diagnostics, and the absence of integrated digital health information systems hamper disease surveillance and programme monitoring capacity.⁴ Extensive hospital closures and reductions in inpatient bed capacity since 1997—undertaken as part of structural reform to shift care to the primary level—have created access deficits that disproportionately affect rural and isolated populations.³
Urban-rural disparities are a defining feature of health service access and outcomes. Primary health care facilities in rural areas face critical shortages of specialist staff, diagnostic equipment, and reliable supply chains for essential medicines.⁴ Telemedicine and digital health represent underutilised levers for extending specialist care to remote communities.
7.3 National Health Strategy 2019–2030
The current Healthy Person – Prosperous Country programme (2019–2030) sets broad strategic goals: strengthening primary care, restructuring the hospital sector, protecting the population from financial risk, and guaranteeing essential service delivery. Its disease priority areas—cardiovascular disease, maternal and child health, tuberculosis, and HIV/AIDS—directly reflect the country's highest-burden conditions.²⁰ The strategy is aligned with WHO's Triple Billion targets and the UN SDG 3 framework for good health and well-being.¹⁵
8. Future Perspectives and Recommendations
The following evidence-based strategic priorities are identified to advance public health in Kyrgyzstan toward 2030 and beyond:
8.1 Strengthening Infectious Disease Control
• Accelerate implementation of WHO-endorsed TB elimination targets by 2030, prioritising deployment of rapid molecular diagnostics (Xpert MTB/RIF and next-generation platforms), shorter MDR-TB regimens (BPaL-M protocol), and community-based treatment adherence support programmes.
• Expand HIV/TB co-infection management capacity, achieve full antiretroviral therapy coverage, and scale prevention of mother-to-child transmission (PMTCT) to eliminate vertical HIV transmission.
• Enact and enforce prescription-only antibiotic dispensing legislation; implement a national antimicrobial stewardship programme in primary care facilities; and adopt point-of-care diagnostic tools (including CRP testing as evaluated in the INSTALL project) to reduce inappropriate antibiotic prescribing.¹³
• Strengthen the Expanded Programme on Immunisation (EPI) through catch-up campaigns in remote communities, improved cold-chain infrastructure, and robust outbreak surveillance systems.
8.2 Addressing the NCD Epidemic
• Scale the WHO Package of Essential Non-Communicable Disease Interventions (PEN) protocol nationally; its effectiveness in improving healthy behaviour has been demonstrated in the Kyrgyz primary care setting.⁸
• Implement comprehensive tobacco control measures including plain packaging, advertising restrictions, and tobacco tax increases; and adopt alcohol policy measures including minimum unit pricing and drink-drive enforcement.
• Integrate systematic CVD and diabetes risk screening into family medicine centre practice, with capacity building for hypertension management and lipid-lowering therapy prescribing at primary care level.
• Develop and resource a national mental health action plan with dedicated funding, community mental health services, anti-stigma campaigns, and integration of mental health screening into routine primary care visits.
8.3 Environmental and Climate Health
• Utilise the World Bank's USD 50 million Air Quality Improvement Project as a platform for comprehensive urban air quality management, with particular focus on transitioning residential and district heating systems away from coal combustion in Bishkek and secondary cities.⁶
• Integrate climate change health adaptation into the national health strategy, encompassing heat-health action plans, surveillance of climate-sensitive diseases (malaria, diarrhoeal diseases, heat stroke), and a climate-resilient health facilities programme.
• Accelerate progress toward SDG 6.1 and 6.2 by expanding safely managed water and sanitation services across rural and mountainous regions, with priority for schools and health facilities.
8.4 Health System Strengthening and Financing
• Progressively increase domestic government health expenditure toward internationally recommended benchmarks, targeting a reduction in out-of-pocket payments to below 30% of total health expenditure by 2030.
• Expand MHIF enrolment from 69% toward universal population coverage, removing financial access barriers for the most vulnerable populations—including remote rural communities, informal sector workers, and the poorest income quintile.
• Invest in a nationally integrated digital health information system for real-time disease surveillance, health workforce management, supply chain monitoring, and patient outcome tracking across all levels of care.
• Develop the rural health workforce through targeted medical and nursing training, deployment incentive schemes, and systematic telemedicine infrastructure to extend specialist consultation capacity to underserved areas.
8.5 Maternal, Neonatal, and Child Health
• Scale evidence-based neonatal care interventions—including Kangaroo Mother Care, antenatal corticosteroids for preterm birth, and community case management of neonatal sepsis—which modelling suggests could prevent up to 39% of neonatal deaths by 2030.¹²
• Strengthen adolescent sexual and reproductive health services, expand family planning access, and address social determinants of early marriage and adolescent pregnancy, particularly in rural oblasts.
• Improve emergency obstetric care availability, skilled birth attendant capacity, and quality of antenatal and postnatal care at district hospital level to reduce the persistently high maternal mortality ratio.
9. Conclusion
Kyrgyzstan's public health landscape in 2025 is characterised by a convergence of longstanding challenges and emergent threats. The country has achieved internationally recognised progress in life expectancy, child survival, and health coverage since independence. However, it simultaneously confronts the region's highest TB incidence, a severe air pollution crisis in its capital, an NCD epidemic accounting for 83% of all deaths, escalating AMR, climate-driven health vulnerabilities, and a health financing model that leaves nearly half of all health expenditure as out-of-pocket costs borne by households.
The national Healthy Person – Prosperous Country strategy (2019–2030) provides a credible and comprehensive framework for addressing these challenges, but its successful implementation will require a significant increase in public health investment, stronger inter-sectoral collaboration, sustained engagement with WHO, UNICEF, and the World Bank, and an unwavering commitment to evidence-based policy and programme design. The convergence of primary care strengthening, disease-specific programme scaling, environmental and climate health action, and health financing reform constitutes the most promising pathway toward improved, equitable, and resilient population health outcomes in Kyrgyzstan.
References
1.World Health Organization (WHO). Health Data Overview for Kyrgyzstan. WHO Data Portal, 2021–2022. Available from: https://data.who.int/countries/417 [Accessed May 2025].
2.World Health Organization (WHO). Country Overview: Kyrgyzstan – Publications and News. WHO, 2023–2025. Available from: https://www.who.int/countries/kgz [Accessed May 2025].
3.European Observatory on Health Systems and Policies. Health Systems in Action: Kyrgyzstan 2024. Copenhagen: WHO Regional Office for Europe, 2024. Available from: https://eurohealthobservatory.who.int/publications/i/health-systems-in-action-kyrgyzstan-2024
4.UNICEF Kyrgyzstan. Improving Health Care. Available from: https://www.unicef.org/kyrgyzstan/improving-health-care [Accessed May 2025]. Incorporates MICS 2023 data.
5.UNICEF. Kyrgyzstan Country Profile: Demographics, Health & Infant Mortality. UNICEF Data, 2024. Available from: https://data.unicef.org/country/kgz/
6.World Bank. World Bank Supports Air Quality Improvement in the Kyrgyz Republic. Press Release, 29 November 2023. Available from: https://www.worldbank.org/en/news/press-release/2023/11/29/world-bank-supports-air-quality-improvement-in-the-kyrgyz-republic
7.P4H Network. Kyrgyzstan Country Profile – Social Health Protection and Health Financing. Updated 2024. Available from: https://p4h.world/en/countries/kyrgyzstan/
8.Muratalieva E, Ablezova M, Djamangulova T, Hoffarth T, Kissimova-Skarbek K, Graeser S, Nendaz M, Beran D. Addressing Non-Communicable Diseases in Primary Healthcare in Kyrgyzstan: A Study on Population's Knowledge and Behavioral Changes. Frontiers in Public Health. 2023;11:1605381. DOI: 10.3389/fpubh.2023.1605381
9.Zhdanova E, Goncharova O, Kadyrov M, Hazoyan A, Sargsyan A, Istamov K, Ortunogutierrez N. Discharge Outcomes of Severely Sick Patients Hospitalised with Multidrug-Resistant Tuberculosis, Comorbidities, and Serious Adverse Events in Kyrgyz Republic, 2020–2022. Tropical Medicine and Infectious Disease. 2023;8. PMC10384159.
10.Yegizbayeva A, Bekova A, Rakhymzhanova G, et al. Multidrug-Resistant Tuberculosis in Central Asia and Predominant Beijing Lineage: Challenges in Diagnosis, Treatment Barriers, and Infection Control Strategies – An Integrative Review. PubMed Central. 2025. PMC12291989.
11.Jenish N, Koichumanova R, Payzuldaeva M, et al. Risk Factors of Cardiovascular Disease in Different Ethnic Groups in Kyrgyzstan. Frontiers in Cardiovascular Medicine. 2024. PMC12039340.
12.Kamali M, et al. Trends and Determinants of Newborn Mortality in Kyrgyzstan: A Countdown Country Case Study. The Lancet Global Health. 2021;9(3):e352–e361. PMC7886656. DOI: 10.1016/S2214-109X(20)30480-X. Commentary: Improving Maternal and Newborn Health in Kyrgyzstan. Lancet Global Health. 2021;9(3):e237–e238.
13.INSTALL Project Team. CRP and Patient Information Leaflets to Optimise Antibiotic Treatments for Adults with Respiratory Tract Infections in Primary Care in Kyrgyzstan. ClinicalTrials.gov Identifier: NCT07261969. Study Protocol Version 2.2, December 2024. Bishkek – Copenhagen.
14.European Observatory on Health Systems and Policies. Kyrgyzstan Health System Summary. Copenhagen: WHO Europe. Available from: https://eurohealthobservatory.who.int/publications/i/kyrgyzstan-health-system-summary
15.United Nations Kyrgyz Republic. Sustainable Development Goal 3: Good Health and Well-being. Available from: https://kyrgyzstan.un.org/en/sdgs/3
16.World Health Organization. Global Tuberculosis Report 2024. Geneva: WHO, 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
17.World Health Organization. WHO Triple Billion Targets – Kyrgyzstan Country Profile 2024. Available from: https://www.who.int/about/accountability/results/who-results-report-2024-2025/country-profile/2024/kyrgyzstan
18.UNAIDS / Joint United Nations Programme on HIV/AIDS. HIV Incidence Data – Kyrgyzstan. Via World Bank World Development Indicators. UNAIDS, 2024. Available from: https://aidsinfo.unaids.org/
19.The Global Fund. Antimicrobial Resistance: A Fast-Growing Threat to the Fight Against HIV, TB and Malaria. 16 September 2024. Available from: https://www.theglobalfund.org/en/video/2024/2024-09-16-antimicrobial-resistance/
20.World Health Organization Regional Office for Europe. Kyrgyzstan Adopts New Health Strategy for 2019–2030. Copenhagen: WHO Europe, 2019. Available from: https://www.euro.who.int/en/countries/kyrgyzstan
21.World Health Organization. World Health Report 2010: Health Systems Financing – The Path to Universal Coverage. Geneva: WHO, 2010. Available from: https://www.who.int/publications/i/item/9789241564021
22.World Bank. Kyrgyzstan Social Health Statistics – World Development Indicators. CEIC/World Bank, 2024. Available from: https://www.ceicdata.com/en/kyrgyzstan/social-health-statistics
23.World Health Organization. WHO STEPwise Approach to Noncommunicable Disease Risk Factor Surveillance (STEPS). Data for Kyrgyzstan. Available from: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps
24.World Health Organization Regional Office for Europe. Drug-Resistant Tuberculosis in Georgia, Kazakhstan, Kyrgyzstan, Moldova, and Ukraine, 2017–2022. Emerging Infectious Diseases. 2024;30(4). Available from: https://wwwnc.cdc.gov/eid/article/30/4/23-1732_article
25.World Health Organization. Noncommunicable Diseases Fact Sheet. Geneva: WHO, 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases