
Complications of Hypertension A Comprehensive Review of Target Organ Damage, Diagnostic Standards, and Contemporary Management Strategies
1. Tamil Manthini Tamil Manthan
Velusamy Jeeva
2. Abdilazizova Asema
(1. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
Arterial hypertension is one of the most prevalent chronic conditions worldwide and remains the single largest modifiable risk factor for cardiovascular morbidity and mortality. Sustained elevation of blood pressure subjects the vasculature and vital organs to chronic hemodynamic stress, culminating in a spectrum of complications collectively termed hypertensive target organ damage (TOD). These complications include hypertensive heart disease (left ventricular hypertrophy, heart failure, and coronary artery disease), cerebrovascular accidents (ischemic and hemorrhagic stroke), chronic kidney disease progressing to end-stage renal failure, hypertensive retinopathy leading to visual impairment, and peripheral arterial disease. This review article examines the pathophysiological mechanisms by which uncontrolled hypertension inflicts cumulative damage on the cardiovascular, cerebrovascular, renal, and ocular systems. Furthermore, we detail current evidence-based diagnostic standards for early detection of subclinical organ damage, including echocardiographic assessment, microalbuminuria screening, and fundoscopic examination. Finally, the contemporary pharmacological and interventional management strategies recommended by the American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology/European Society of Hypertension (ESC/ESH) guidelines are critically discussed.
Keywords: Arterial Hypertension, Target Organ Damage, Left Ventricular Hypertrophy, Hypertensive Nephropathy, Stroke, Hypertensive Retinopathy, Guideline-Directed Therapy.
1. Introduction
Arterial hypertension, defined as a sustained systolic blood pressure (SBP) ≥ 130 mmHg and/or diastolic blood pressure (DBP) ≥ 80 mmHg according to the 2017 ACC/AHA guidelines, or ≥ 140/90 mmHg per the 2018 ESC/ESH framework, affects approximately 1.28 billion adults globally [1]. Often labeled the “silent killer,” hypertension frequently remains asymptomatic for years or even decades while progressively damaging the arterial vasculature and the organs it supplies. The World Health Organization estimates that hypertension is directly responsible for over 10 million deaths annually, making it the leading modifiable risk factor for premature cardiovascular death [2].
The clinical significance of hypertension lies not merely in the elevated pressure readings themselves, but in the devastating cascade of complications that arise from prolonged hemodynamic overload. These complications—encompassing hypertensive heart disease, stroke, chronic kidney disease, retinopathy, and peripheral vascular disease—constitute the true burden of the condition. Modern evidence-based guidelines from the ACC/AHA and ESC/ESH have therefore shifted the clinical paradigm from reactive treatment of acute events to proactive screening for subclinical target organ damage (TOD) and aggressive early intervention to prevent irreversible end-organ injury [1, 3].
This review aims to provide a structured analysis of the major complications of hypertension, their underlying pathophysiology, diagnostic approaches, and current management recommendations.
2. Pathophysiology of Hypertensive Target Organ Damage
Understanding the pathophysiological mechanisms through which sustained hypertension damages vital organs is essential for the clinician aiming to intervene at the earliest possible stage. The damage is mediated through interconnected vascular, neurohormonal, and inflammatory pathways.
2.1 Hemodynamic Stress and Vascular Remodeling
Chronic elevation of arterial pressure subjects the vascular endothelium to excessive shear stress and circumferential wall tension. This mechanical insult triggers endothelial dysfunction, characterized by reduced bioavailability of nitric oxide (NO) and increased production of vasoconstrictors such as endothelin-1 [4]. Over time, the medial layer of arterial walls undergoes hypertrophy and fibrosis, resulting in arterial stiffening and increased pulse wave velocity. This structural remodeling increases systolic pressure further through loss of arterial compliance, creating a self-perpetuating vicious cycle of rising pressure and progressive vascular damage.
2.2 Neurohormonal Activation
The Renin-Angiotensin-Aldosterone System (RAAS) plays a central role in hypertensive organ damage. Angiotensin II, beyond its vasoconstrictive properties, acts as a potent growth factor that promotes cardiomyocyte hypertrophy, vascular smooth muscle cell proliferation, and renal mesangial cell expansion [1]. Aldosterone contributes to myocardial and perivascular fibrosis. Simultaneously, chronic sympathetic nervous system overactivation elevates heart rate, increases myocardial oxygen demand, and promotes glomerular hyperfiltration—all of which accelerate end-organ injury [5].
2.3 Oxidative Stress and Inflammation
Hypertension promotes the generation of reactive oxygen species (ROS), primarily through NADPH oxidase activation in the vascular wall. ROS quench nitric oxide, oxidize low-density lipoproteins, and activate nuclear factor kappa-B (NF-κB), triggering a cascade of pro-inflammatory cytokine release. This chronic low-grade vascular inflammation accelerates atherosclerosis, promotes plaque instability, and contributes to glomerulosclerosis in the kidneys [4, 6].
3. Cardiovascular Complications
The heart is one of the primary targets of chronic hypertension. The spectrum of hypertensive heart disease encompasses left ventricular hypertrophy (LVH), coronary artery disease (CAD), heart failure (HF), and arrhythmias.
3.1 Left Ventricular Hypertrophy (LVH)
Chronic pressure overload forces the left ventricle to increase its wall thickness in order to normalize wall stress, a process termed concentric hypertrophy. While initially compensatory, sustained LVH leads to impaired diastolic relaxation, increased myocardial oxygen demand, reduced coronary flow reserve, and a predisposition to ventricular arrhythmias [1]. The Framingham Heart Study demonstrated that LVH, detected by echocardiography, is an independent predictor of cardiovascular events, with a two- to fourfold increase in risk of myocardial infarction, stroke, and sudden cardiac death [7]. The 2018 ESC/ESH guidelines recommend echocardiographic assessment of left ventricular mass index (LVMI) as a standard diagnostic measure for subclinical cardiac damage, with thresholds of >115 g/m² for men and >95 g/m² for women defining LVH [3].
3.2 Hypertensive Heart Failure
Hypertension is the most common predisposing factor for heart failure. The progression from LVH to diastolic dysfunction and eventually to overt Heart Failure with Preserved Ejection Fraction (HFpEF) is well-characterized. In advanced cases, the ventricle may transition from a concentric to an eccentric (dilated) pattern, leading to systolic failure (HFrEF). Current Guideline-Directed Medical Therapy for hypertensive heart failure follows the same four-pillar approach described in HFrEF management: ARNI (Sacubitril/Valsartan), evidence-based beta-blockers (Carvedilol, Bisoprolol, Metoprolol Succinate), mineralocorticoid receptor antagonists (Spironolactone, Eplerenone), and SGLT2 inhibitors (Dapagliflozin, Empagliflozin) [8].
3.3 Coronary Artery Disease
Hypertension accelerates the atherosclerotic process through endothelial injury, lipid infiltration, and inflammatory plaque development. Elevated blood pressure increases coronary shear stress, promotes plaque erosion, and raises the risk of acute coronary syndromes. Hypertension and hyperlipidemia together have a synergistic effect on coronary risk, and aggressive blood pressure control alongside statin therapy is the therapeutic standard [1, 3].
4. Cerebrovascular Complications
Hypertension is the most potent modifiable risk factor for both ischemic and hemorrhagic stroke. Chronic elevation of blood pressure accelerates cerebral atherosclerosis and weakens the walls of small perforating arteries, predisposing to distinct but equally devastating forms of cerebrovascular injury.
4.1 Ischemic Stroke
Approximately 80–85% of all strokes are ischemic in origin. Hypertension promotes large-vessel atherosclerosis affecting the carotid and vertebrobasilar arteries, as well as small-vessel lipohyalinosis that causes lacunar infarctions. Additionally, hypertension is a major risk factor for atrial fibrillation, which itself is a leading cause of cardioembolic stroke [2, 9]. Meta-analyses of antihypertensive trials have consistently shown that each 10 mmHg reduction in systolic blood pressure reduces the risk of stroke by approximately 27%, underscoring the paramount importance of blood pressure control in primary and secondary stroke prevention [10].
4.2 Hemorrhagic Stroke
Intracerebral hemorrhage (ICH) accounts for approximately 15% of all strokes but carries a mortality rate exceeding 40%. Chronic hypertension causes Charcot-Bouchard microaneurysms in the small penetrating arteries of the basal ganglia, thalamus, pons, and cerebellum. Acute hypertensive surges can rupture these weakened vessels, producing intracerebral hemorrhage. Rapid blood pressure reduction to a target of <140 mmHg systolic within the first hour of ICH presentation has been shown to improve functional outcomes [9].
4.3 Hypertensive Encephalopathy
A rare but life-threatening complication, hypertensive encephalopathy occurs when blood pressure exceeds the upper limit of cerebral autoregulation (typically above 180/120 mmHg). The resulting hyperperfusion and breakdown of the blood-brain barrier produces vasogenic cerebral edema, clinically presenting as severe headache, confusion, seizures, and visual disturbances. Neuroimaging classically reveals posterior reversible encephalopathy syndrome (PRES). This constitutes a hypertensive emergency requiring immediate parenteral antihypertensive therapy with agents such as nicardipine or labetalol [1, 3].
5. Renal Complications (Hypertensive Nephropathy)
The kidneys are both a cause and a consequence of hypertension. Chronic hypertension inflicts progressive damage on the renal vasculature and glomerular apparatus, ultimately leading to chronic kidney disease (CKD) and, in severe cases, end-stage renal disease (ESRD).
5.1 Pathology of Hypertensive Nephrosclerosis
Sustained hypertension causes two principal forms of renal vascular damage. Benign nephrosclerosis is characterized by hyaline arteriosclerosis of the afferent arterioles, leading to ischemic glomerular obsolescence and tubulointerstitial fibrosis. Malignant nephrosclerosis, seen in hypertensive emergencies, involves fibrinoid necrosis of the afferent arterioles and hyperplastic (“onion-skin”) changes of the interlobular arteries, causing rapidly progressive renal failure [1, 6].
5.2 Diagnostic Standards for Renal Involvement
Early detection of hypertensive renal damage requires systematic screening. The ESC/ESH guidelines recommend measurement of serum creatinine, estimation of the glomerular filtration rate (eGFR) using the CKD-EPI formula, and quantification of the urine albumin-to-creatinine ratio (UACR). Microalbuminuria (UACR 30–300 mg/g) is one of the earliest markers of hypertensive nephropathy and endothelial dysfunction, and its detection should prompt intensification of antihypertensive therapy [3, 6].
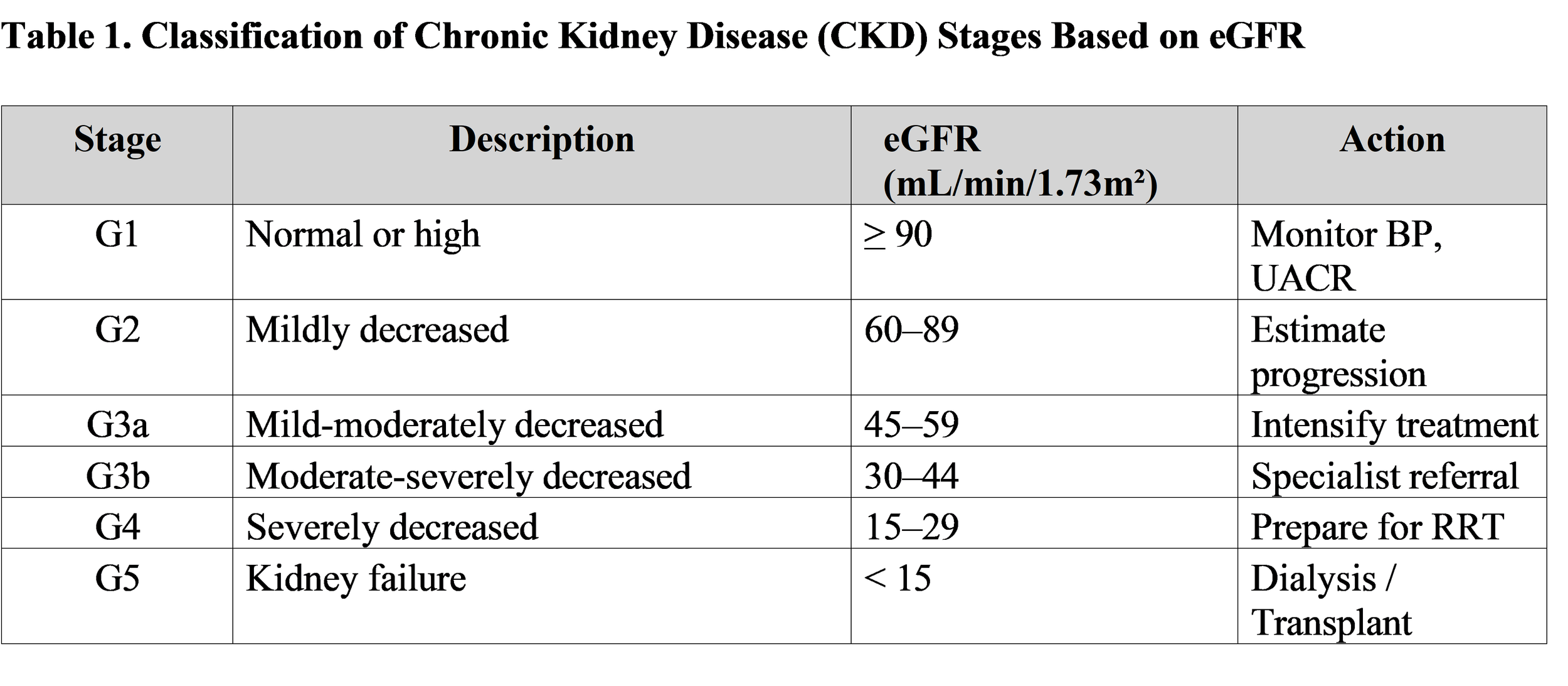
(Adapted from: KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease)
5.3 Pharmacological Renoprotection
Agents that block the RAAS—ACE inhibitors (e.g., Ramipril, Enalapril) or Angiotensin Receptor Blockers (e.g., Losartan, Valsartan)—form the cornerstone of renoprotective therapy due to their ability to reduce intraglomerular pressure and proteinuria independent of their systemic antihypertensive effects. SGLT2 inhibitors have also demonstrated significant renoprotective benefits in the DAPA-CKD and EMPA-KIDNEY trials, earning their recommendation in patients with CKD regardless of diabetes status [6, 8].
6. Ocular Complications (Hypertensive Retinopathy)
The retinal vasculature provides a unique, directly observable window into the systemic microvascular status. Fundoscopic examination allows clinicians to visualize the effects of hypertension on small vessels in real time, making it an invaluable diagnostic tool.
6.1 Keith-Wagener-Barker Classification
Hypertensive retinopathy is traditionally graded using the Keith-Wagener-Barker (KWB) classification system, which correlates retinal findings with the severity and chronicity of hypertension [1]:
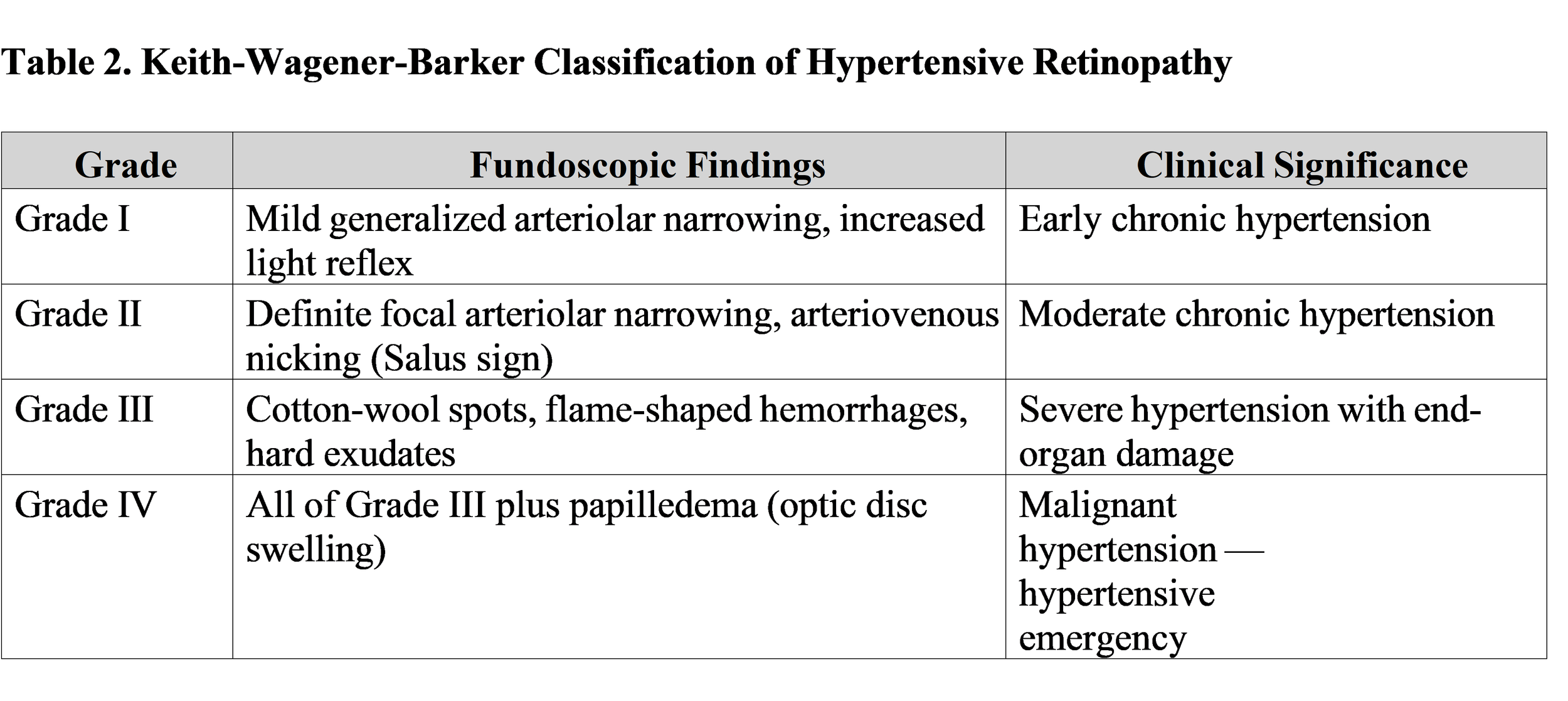
(Adapted from: Harrison’s Principles of Internal Medicine, 21st ed., McGraw Hill, 2022)
7. Peripheral Vascular Complications
Hypertension is a major independent risk factor for peripheral arterial disease (PAD) and aortic aneurysm formation.
7.1 Peripheral Arterial Disease (PAD)
Chronic hypertension accelerates atherosclerosis in the lower extremity arteries, leading to intermittent claudication, critical limb ischemia, and increased risk of amputation. The ankle-brachial index (ABI) is the standard screening tool; a value of <0.9 confirms the diagnosis of PAD and is also a strong predictor of generalized atherosclerotic burden and cardiovascular mortality [3, 11].
7.2 Aortic Aneurysm and Dissection
Sustained hypertension weakens the aortic media through chronic mechanical stress and medial degeneration, predisposing to aneurysm formation in both the thoracic and abdominal segments. Acute aortic dissection, one of the most catastrophic cardiovascular emergencies, is strongly associated with uncontrolled hypertension. Immediate reduction of systolic blood pressure to 100–120 mmHg using intravenous beta-blockers (e.g., Esmolol) is the standard of emergency management [1, 12].
8. Hypertensive Emergencies and Urgencies
A critical distinction exists between hypertensive urgency (severely elevated blood pressure without acute end-organ damage) and hypertensive emergency (severely elevated blood pressure with evidence of ongoing end-organ damage to the brain, heart, kidneys, or vasculature). Hypertensive emergencies include hypertensive encephalopathy, acute left ventricular failure with pulmonary edema, acute coronary syndrome, aortic dissection, eclampsia, and acute renal failure [1, 3].
Management of hypertensive emergencies requires admission to an intensive care unit and the use of titratable intravenous antihypertensive agents. The general recommendation is to lower the mean arterial pressure by no more than 25% within the first hour, then gradually to 160/100 mmHg over the next 2–6 hours, with the exception of aortic dissection which requires more aggressive initial reduction. Preferred intravenous agents include Nicardipine, Labetalol, Nitroprusside (with cyanide toxicity monitoring), and Clevidipine [3, 12].
9. Comprehensive Management Strategy
The prevention and management of hypertensive complications require a dual strategy of non-pharmacological lifestyle modification and pharmacological blood pressure control.
9.1 Lifestyle Modifications
The ACC/AHA and ESC/ESH guidelines recommend the following non-pharmacological interventions as the foundation of all antihypertensive therapy: dietary sodium reduction to <2 g/day (DASH diet), regular aerobic exercise (at least 150 minutes per week of moderate-intensity activity), weight reduction (target BMI <25 kg/m²), moderation of alcohol consumption, cessation of tobacco use, and stress management. Lifestyle modifications alone can reduce systolic blood pressure by 4–11 mmHg [1, 3].
9.2 Pharmacological Therapy
First-line antihypertensive drug classes include ACE inhibitors, Angiotensin Receptor Blockers (ARBs), Calcium Channel Blockers (CCBs, e.g., Amlodipine), and Thiazide-type diuretics (e.g., Chlorthalidone, Indapamide). For patients with Stage 2 hypertension (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg), dual combination therapy is recommended as first-line treatment. Fixed-dose single-pill combinations are preferred due to improved adherence. Target blood pressure for most patients is <130/80 mmHg per ACC/AHA guidelines [1].
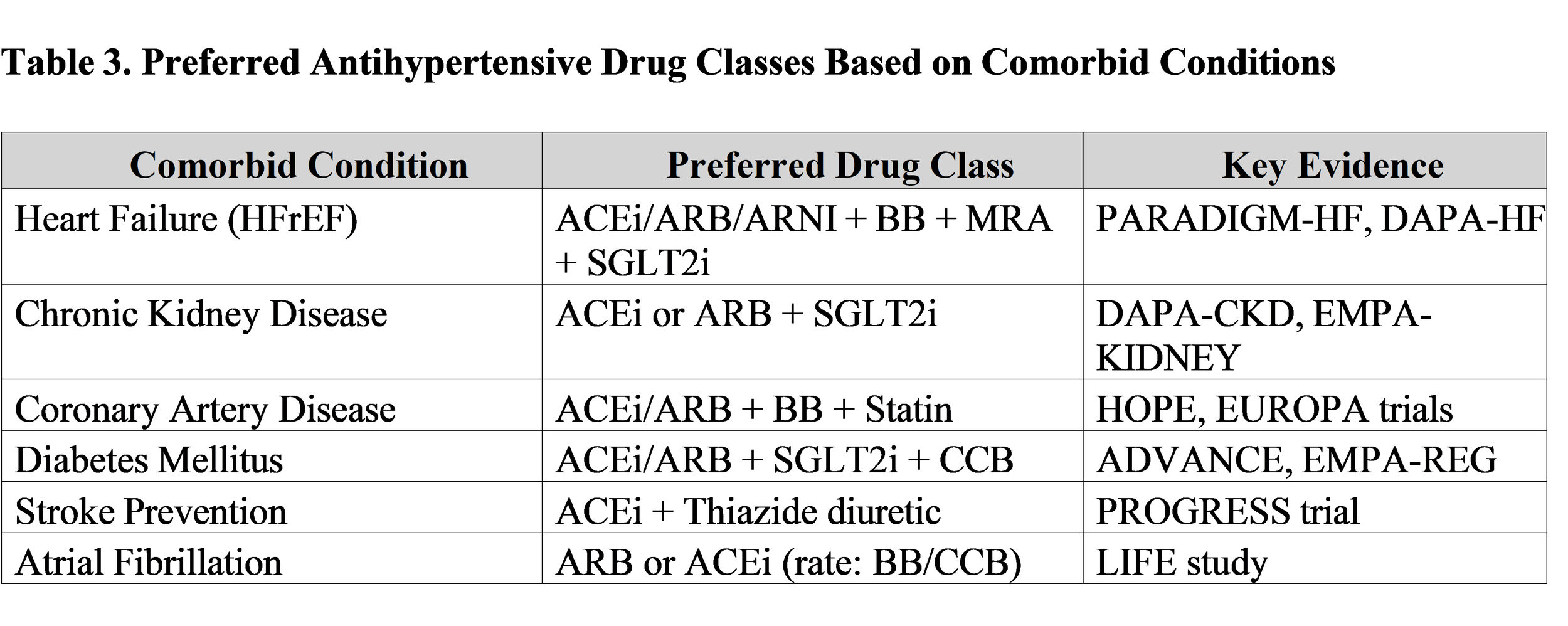
(Compiled from: 2017 ACC/AHA Hypertension Guideline and 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension)
10. Conclusion
Arterial hypertension, through sustained hemodynamic overload and chronic activation of neurohormonal and inflammatory pathways, inflicts progressive and often irreversible damage on virtually every major organ system. The complications of uncontrolled hypertension—ranging from left ventricular hypertrophy and heart failure, to ischemic and hemorrhagic stroke, chronic kidney disease, retinopathy, and aortic dissection—constitute the primary drivers of global cardiovascular morbidity and mortality. Modern clinical standards demand a proactive, prevention-oriented approach: systematic screening for subclinical target organ damage through echocardiography, microalbuminuria testing, and fundoscopy; aggressive blood pressure control with evidence-based pharmacotherapy tailored to comorbid conditions; and sustained lifestyle modification. Strict adherence to the recommendations outlined by the ACC/AHA and ESC/ESH guidelines can fundamentally alter the natural trajectory of hypertensive disease, preventing the transition from silent vascular injury to catastrophic end-organ failure.
Disclosure of Funding Sources
The authors declare that no specific funding was received for the preparation of this review article. No granting agencies, institutional support, or non-material project frameworks contributed to this work.
11. References
[1] Whelton, P. K., Carey, R. M., Aronow, W. S., et al. (2018). 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Journal of the American College of Cardiology, 71(19), e127–e248. https://doi.org/10.1016/j.jacc.2017.11.006
[2] World Health Organization. (2023). Global report on hypertension: The race against a silent killer. WHO. https://www.who.int/publications/i/item/9789240081062
[3] Williams, B., Mancia, G., Spiering, W., et al. (2018). 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal, 39(33), 3021–3104. https://doi.org/10.1093/eurheartj/ehy339
[4] Zipes, D. P., Libby, P., Bonow, R. O., Mann, D. L., & Tomaselli, G. F. (2021). Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine (12th ed.). Elsevier. ISBN: 978-0323824675.
[5] Jameson, J. L., Fauci, A. S., Kasper, D. L., Hauser, S. L., Longo, D. L., & Loscalzo, J. (2022). Harrison’s Principles of Internal Medicine (21st ed.). McGraw Hill. ISBN: 978-1264268504.
[6] KDIGO. (2024). KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements, 14(4), e1–e314. https://doi.org/10.1016/j.kisu.2024.05.001
[7] Levy, D., Garrison, R. J., Savage, D. D., Kannel, W. B., & Castelli, W. P. (1990). Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. The New England Journal of Medicine, 322(22), 1561–1566. https://doi.org/10.1056/NEJM199005313222203
[8] Heidenreich, P. A., Bozkurt, B., Aguilar, D., et al. (2022). 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. Circulation, 145(18), e895–e1032. https://doi.org/10.1161/CIR.0000000000001063
[9] Greenberg, S. M., Ziai, W. C., Cordonnier, C., et al. (2022). 2022 Guideline for the Management of Patients with Spontaneous Intracerebral Hemorrhage. Stroke, 53(7), e282–e361. https://doi.org/10.1161/STR.0000000000000407
[10] Ettehad, D., Emdin, C. A., Kiran, A., et al. (2016). Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. The Lancet, 387(10022), 957–967. https://doi.org/10.1016/S0140-6736(15)01225-8
[11] Gerhard-Herman, M. D., Gornik, H. L., Barrett, C., et al. (2017). 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease. Circulation, 135(12), e218–e275. https://doi.org/10.1161/CIR.0000000000000471
[12]Aronow, W. S. (2017). Treatment of hypertensive emergencies. Annals of Translational