
Evidence-Based Medicine in Cardiology: Methodological Guidelines and Standards for the Diagnosis and Treatment of Arterial Hypertension
1. Mohamed Mujahidislam Baig
Kaviya
2. Abdilazizova Asema
(1. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
Evidence-based medicine (EBM) has fundamentally transformed the practice of clinical cardiology over the past three decades by anchoring therapeutic decisions in rigorously derived, reproducible scientific evidence rather than empiricism or tradition. Nowhere is this transformation more consequential than in the management of arterial hypertension—the world’s most prevalent modifiable cardiovascular risk factor, affecting over 1.28 billion adults and responsible for more than
10 million deaths annually. Current international guidelines from the American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology/European Society of Hypertension (ESC/ESH) represent the crystallisation of decades of randomised controlled trials, systematic reviews, and meta-analyses into actionable clinical standards. This review article examines the methodological foundations of EBM as applied to cardiology, outlines the hierarchical framework of clinical evidence from landmark hypertension trials, details the contemporary diagnostic criteria and risk stratification standards recommended by major guidelines, and synthesises the pharmacological and non-pharmacological treatment strategies supported by the highest levels of evidence. Special attention is given to specific patient subgroups, hypertensive emergencies, and the challenge of therapeutic inertia in achieving guideline-concordant blood pressure control.
Keywords: Evidence-Based Medicine, Arterial Hypertension, Clinical Guidelines, ACC/AHA, ESC/ESH, Randomised Controlled Trials, Blood Pressure Control, Cardiovascular Risk.
1. Introduction
Evidence-based medicine, as defined by Sackett and colleagues in their seminal 1996 paper in the British Medical Journal, is “the conscientious, explicit, and judicious use of current best
evidence in making decisions about the care of individual patients” [1]. It represents a synthesis of the best available external clinical evidence from systematic research with individual clinical expertise and patient values. In the domain of cardiology—a specialty underpinned by a rich tradition of large-scale randomised controlled trials (RCTs)—EBM has become the default operational framework for developing clinical practice guidelines, evaluating diagnostic technologies, and appraising the efficacy and safety of therapeutic interventions.
Arterial hypertension serves as arguably the most powerful paradigm for the application of EBM principles in cardiovascular medicine. The condition is simultaneously ubiquitous, modifiable, and catastrophic in its untreated consequences—conferring a two- to threefold increase in the risk of stroke, myocardial infarction, heart failure, chronic kidney disease, and premature death [2]. The therapeutic landscape for hypertension has been shaped by over 150 major clinical trials enrolling millions of patients over six decades, generating an unparalleled evidence base for treatment decisions. Yet despite this wealth of evidence and clear guideline recommendations, global blood pressure control rates remain alarmingly poor, with fewer than one in five hypertensive adults worldwide achieving their target blood pressure [3].
This article therefore serves a dual purpose: first, to elucidate the methodological principles that underpin EBM and their application to hypertension research; and second, to provide a comprehensive, guideline-grounded reference for the diagnosis, risk stratification, and treatment of arterial hypertension, with emphasis on the landmark clinical trial evidence supporting each recommendation.
2. Methodological Foundations of Evidence-Based Medicine in Cardiology
2.1 The Hierarchy of Clinical Evidence
The EBM framework organises clinical evidence into a hierarchical pyramid, with study designs ranked according to their susceptibility to bias and their inferential power. The Oxford Centre for Evidence-Based Medicine (OCEBM) levels of evidence provide the most widely adopted classification system [1, 4]:
Level 1a — Systematic reviews and meta-analyses of RCTs: The highest level of evidence, synthesising results from multiple trials to provide pooled effect estimates with increased statistical power and precision. The Cochrane Collaboration maintains the most comprehensive repository of systematic reviews in cardiology.
Level 1b — Individual randomised controlled trials with narrow confidence intervals:
The methodological gold standard for evaluating therapeutic efficacy. Landmark hypertension trials
such as ALLHAT, SPRINT, HOPE, and PROGRESS have provided Level 1b evidence directly shaping current guidelines.
Level 2 — Cohort studies: Prospective longitudinal studies that established the epidemiological relationship between blood pressure levels and cardiovascular outcomes. The Framingham Heart Study is the exemplar, having defined the continuous, log-linear relationship between blood pressure and cardiovascular risk.
Level 3 — Case-control studies: Retrospective comparisons of patients with and without outcomes, useful for rare events and hypothesis generation.
Level 4 — Case series and cross-sectional studies: Descriptive studies that provide the lowest level of controlled evidence.
Level 5 — Expert opinion and mechanistic reasoning: The lowest level, relied upon only when higher-quality evidence is unavailable.
2.2 Guideline Development Methodology
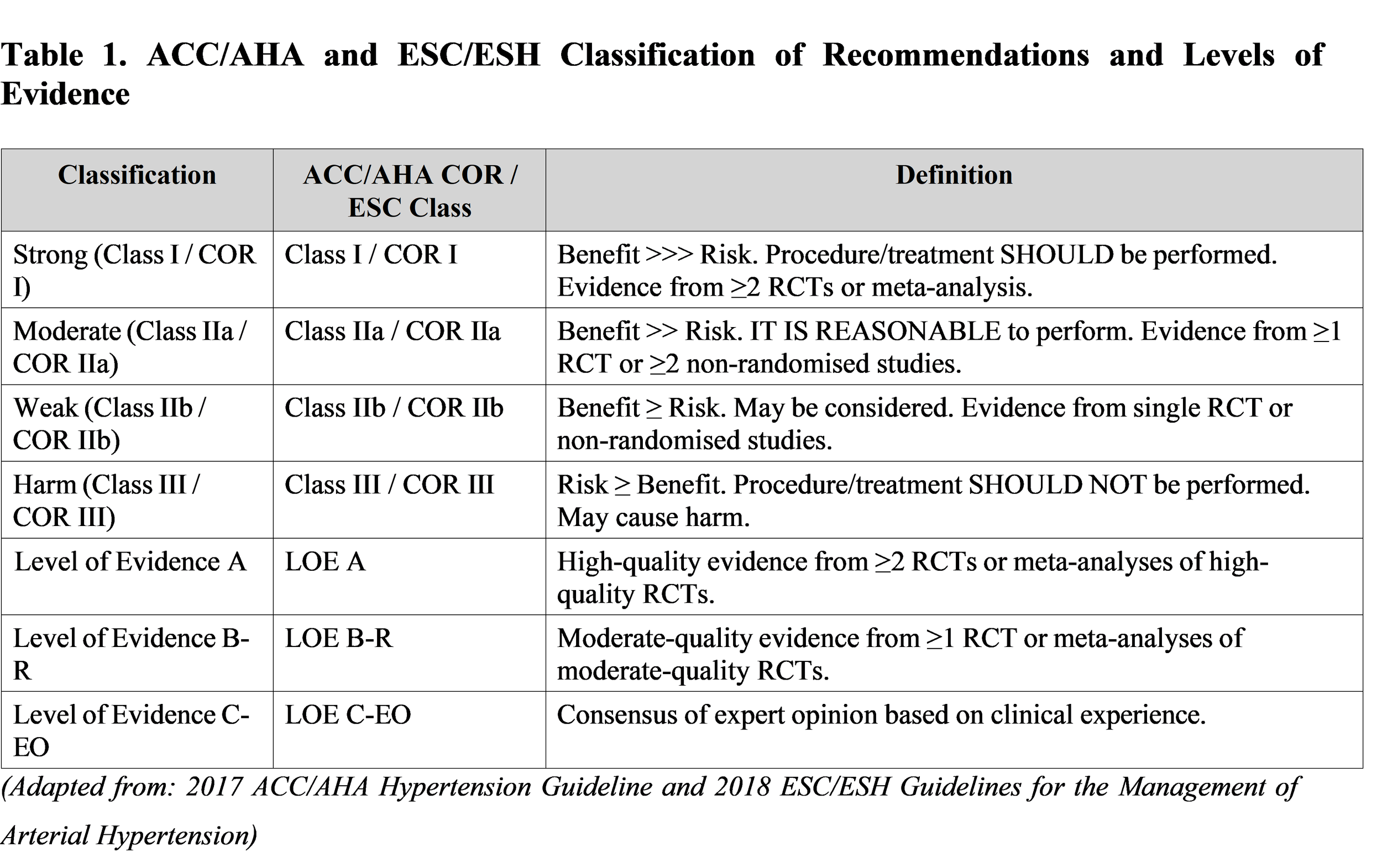
Clinical practice guidelines translate the evidence hierarchy into actionable recommendations through a structured, transparent process. Both the ACC/AHA and ESC/ESH employ a Class of Recommendation (COR) and Level of Evidence (LOE) grading system that explicitly communicates the strength of each recommendation [2, 3]:
2.3 Critical Appraisal of Hypertension Trials
The critical appraisal of clinical trials for application to hypertension management requires systematic evaluation of internal validity (freedom from bias), statistical precision (confidence intervals, p-values), clinical significance (absolute risk reduction, number needed to treat), generalisability (external validity), and potential conflicts of interest. Key methodological considerations unique to antihypertensive trials include the choice of blood pressure target, the use of active-comparator versus placebo designs, the adequacy of blinding given the physiological effects of drug classes, and the duration of follow-up required to capture hard cardiovascular endpoints such as stroke, myocardial infarction, and death [4, 5].
3. Definition and Classification of Arterial Hypertension
3.1 Diagnostic Thresholds: Guideline Divergence and Rationale
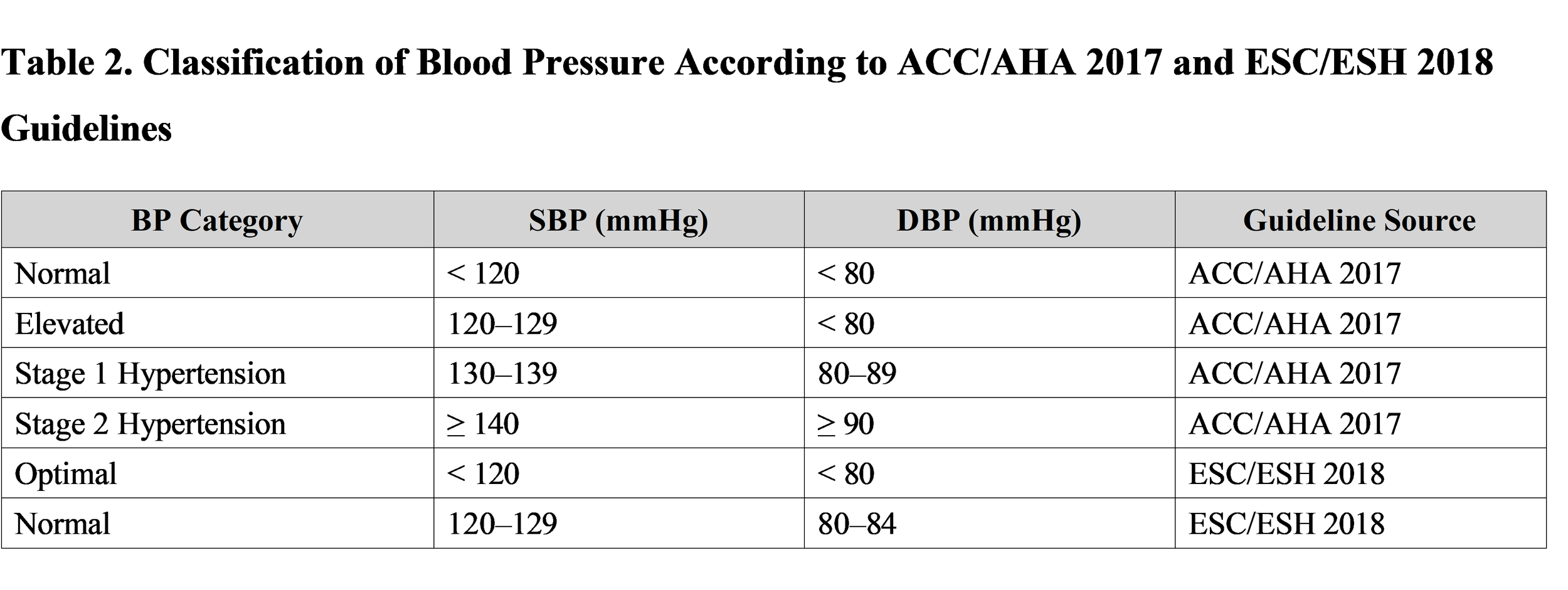
The definition of hypertension has been a subject of significant guideline divergence, with meaningful implications for the proportion of the population classified as hypertensive and therefore eligible for treatment. The 2017 ACC/AHA guideline, informed principally by the landmark SPRINT trial, lowered the diagnostic threshold to SBP ≥ 130 mmHg and/or DBP ≥ 80 mmHg, replacing the previous 140/90 mmHg threshold [2]. This reclassification increased the estimated prevalence of hypertension in the United States from 32% to 46% of adults. The 2018 ESC/ESH guideline retained the 140/90 mmHg threshold as the definition of hypertension, citing concerns about the generalisation of SPRINT methodology (using unattended automated office blood pressure measurement) and differences in the European cardiovascular risk landscape [3].

3.2 Measurement Standards
Accurate blood pressure measurement is the cornerstone of hypertension diagnosis and monitoring. Both ACC/AHA and ESC/ESH guidelines emphasise that office blood pressure (OBP) readings should be obtained under standardised conditions: the patient seated for ≥5 minutes, arm at heart level, using a validated electronic device with an appropriately sized cuff, with the average of ≥2 readings taken on ≥2 separate visits used for diagnosis. Out-of-office blood pressure assessment through ambulatory blood pressure monitoring (ABPM) or home blood pressure monitoring (HBPM)—is strongly recommended for the detection of white-coat hypertension, masked hypertension, and nocturnal hypertension [3, 5].
ABPM remains the gold standard for blood pressure assessment: it provides 24-hour mean blood pressure, diurnal patterns (dipping vs. non-dipping), and blood pressure variability—all of which carry independent prognostic information beyond office readings. The ESC/ESH guideline assigns a Class I, Level A recommendation to ABPM for confirming hypertension before treatment initiation in most patients [3].
4. Cardiovascular Risk Stratification
4.1 The ESC/ESH Risk Stratification Model
The ESC/ESH 2018 guideline employs a composite cardiovascular risk stratification framework that integrates blood pressure grade with the presence of additional cardiovascular risk factors, evidence of hypertensive target organ damage (TOD), and established cardiovascular or renal disease. This model stratifies patients into Low, Moderate, High, and Very High cardiovascular risk categories, which in turn determine treatment urgency and blood pressure targets [3].
Major cardiovascular risk factors incorporated into ESC/ESH stratification include: age (≥55 years in men, ≥65 years in women), current tobacco use, dyslipidaemia (LDL-C ≥ 4.9 mmol/L or total cholesterol ≥ 6.2 mmol/L), impaired fasting glucose (5.6–6.9 mmol/L), obesity (BMI ≥30 kg/m²), family history of premature cardiovascular disease, and uric acid elevation. Evidence of TOD—encompassing left ventricular hypertrophy, increased carotid intima-media thickness, microalbuminuria, and reduced eGFR—upgrades risk to the High or Very High category regardless of blood pressure grade [3, 6].
4.2 The ACC/AHA 10-Year ASCVD Risk Calculator
The ACC/AHA guideline employs the Pooled Cohort Equations (PCE) to estimate the 10-year risk of atherosclerotic cardiovascular disease (ASCVD)—defined as fatal or non-fatal coronary heart disease or stroke. The PCE incorporates age, sex, race, total and HDL cholesterol, systolic blood pressure, antihypertensive treatment status, diabetes status, and smoking history. Patients with Stage 1 hypertension (SBP 130–139 or DBP 80–89 mmHg) and 10-year ASCVD risk ≥ 10% are recommended pharmacological treatment, while those with lower risk are managed initially with lifestyle interventions alone [2, 7].
5. Diagnostic Evaluation: Guideline-Recommended Standards
5.1 Laboratory Investigations
Both ACC/AHA and ESC/ESH guidelines recommend a standardised baseline laboratory workup at the time of hypertension diagnosis to identify secondary causes, assess cardiovascular risk factors, screen for target organ damage, and establish baseline values for drug safety monitoring. Recommended investigations include fasting plasma glucose and HbA1c (diabetes screening), full fasting lipid profile (total cholesterol, LDL-C, HDL-C, triglycerides), serum electrolytes (sodium, potassium) with creatinine and eGFR (CKD detection and RAAS drug safety), urine dipstick and/or urine albumin-to-creatinine ratio (UACR) for proteinuria, thyroid-stimulating hormone (TSH) for hypothyroidism exclusion, and 12-lead electrocardiogram for LVH detection and arrhythmia screening [3, 5].
5.2 Screening for Secondary Hypertension
Secondary hypertension—accounting for approximately 5–10% of all hypertension cases—should be suspected in patients with onset before age 30, resistant hypertension despite three-drug therapy, acute blood pressure elevation superimposed on previously stable hypertension, or clinical/laboratory clues suggesting specific aetiologies. The most common causes and their guideline-recommended screening tests include: primary aldosteronism (plasma aldosterone-to-renin ratio), renal parenchymal disease (serum creatinine, eGFR, UACR), renovascular hypertension (renal duplex Doppler ultrasonography, CT angiography), obstructive sleep apnoea (Epworth Sleepiness Scale, polysomnography), and phaeochromocytoma (24-hour urinary catecholamines and metanephrines) [3, 6].
5.3 Assessment of Target Organ Damage
Systematic evaluation for subclinical TOD is mandated by guidelines as it significantly upgrades cardiovascular risk, may influence treatment intensity, and allows monitoring of treatment response. Recommended TOD assessments include echocardiography (left ventricular mass index — LVMI, diastolic function, ejection fraction), carotid ultrasound (intima-media thickness, plaque detection), urine UACR (microalbuminuria — UACR 30–300 mg/g), serum creatinine and eGFR, and fundoscopy (hypertensive retinopathy grading) in Grade 2–3 hypertension or suspected hypertensive emergency [3, 6].
6. Landmark Clinical Trials Shaping Hypertension Guidelines
6.1 The SPRINT Trial (2015)
The Systolic Blood Pressure Intervention Trial (SPRINT) randomised 9,361 high-risk hypertensive adults (excluding diabetes and prior stroke) to an intensive blood pressure target of SBP < 120 mmHg versus a standard target of SBP < 140 mmHg. The trial demonstrated a 25% relative risk reduction in the primary composite cardiovascular outcome and a 27% reduction in all-cause mortality in the intensive-treatment group, at the cost of a higher incidence of hypotension, syncope, and acute kidney injury [2]. SPRINT provided the pivotal Level 1b evidence for the ACC/AHA’s 2017 decision to lower the hypertension diagnostic threshold and adopt a universal SBP target of < 130 mmHg for most high-risk patients.
6.2 The ALLHAT Trial (2002)
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)—the largest antihypertensive RCT ever conducted (n = 33,357)—compared a thiazide-like diuretic (chlorthalidone) against an ACE inhibitor (lisinopril) and a calcium channel blocker (amlodipine) as first-line therapy. The trial found no significant difference in the primary outcome (fatal coronary heart disease + non-fatal MI) between treatment arms, but chlorthalidone demonstrated superiority in preventing heart failure and stroke versus the comparators [7, 8]. ALLHAT cemented thiazide-type diuretics as essential components of first-line antihypertensive therapy, particularly chlorthalidone over hydrochlorothiazide.
6.3 The HOPE and ONTARGET Trials
The Heart Outcomes Prevention Evaluation (HOPE) trial demonstrated that Ramipril (10 mg/day) reduced the composite outcome of myocardial infarction, stroke, and cardiovascular death by 22% relative risk in high-risk patients, establishing ACE inhibitors as cornerstone agents in cardiovascular risk reduction beyond their blood pressure-lowering effect [9]. The subsequent ONTARGET trial (n = 25,620) showed that Telmisartan was non-inferior to Ramipril for cardiovascular outcomes, while combination RAAS blockade (Ramipril + Telmisartan) offered no incremental benefit but significantly increased adverse effects, establishing the principle that dual RAAS blockade is contraindicated.
6.4 The PROGRESS Trial
The Perindopril Protection Against Recurrent Stroke Study (PROGRESS) randomised 6,105 patients with prior stroke or TIA to a regimen of Perindopril ± Indapamide versus placebo. Active treatment reduced the risk of recurrent stroke by 28% and the combination of stroke and major vascular events by 26%, establishing ACE inhibitor + thiazide-like diuretic combination as the evidence-based standard for secondary stroke prevention in hypertensive patients [10].
7. Evidence-Based Treatment Standards
7.1 Non-Pharmacological Interventions: First-Line for All Patients
Both ACC/AHA and ESC/ESH guidelines assign Class I recommendations to lifestyle modifications as the foundation of hypertension management for all patients, irrespective of blood pressure severity or pharmacotherapy status. The evidence base for lifestyle interventions, while derived primarily from shorter-duration RCTs and meta-analyses rather than long-term outcomes trials, is robust for blood pressure-lowering efficacy [2, 3]. Key evidence-based interventions include:
Dietary sodium restriction: A meta-analysis of 34 trials demonstrated that reducing sodium intake to < 2 g/day (5 g salt/day) reduces SBP by 5.1 mmHg and DBP by 2.7 mmHg. The DASH (Dietary Approaches to Stop Hypertension) diet combining low sodium, high potassium, and high fruit/vegetable intake reduces SBP by 8–14 mmHg.
Regular aerobic exercise: 150–300 minutes per week of moderate-intensity aerobic activity (brisk walking, cycling) reduces SBP by 4ₓ10 mmHg. Dynamic resistance training provides additional but lesser benefit.
Weight reduction: Every 1 kg reduction in body weight is associated with approximately 1 mmHg reduction in SBP. A 10 kg weight loss reduces SBP by 6 mmHg on average.
Alcohol moderation: Limiting consumption to ≤2 standard drinks/day in men and ≤1/day in women reduces SBP by 4–6 mmHg in hypertensive patients.
Tobacco cessation: While smoking cessation does not lower blood pressure per se, it substantially reduces overall cardiovascular risk and is therefore an essential component of the hypertension management plan.
7.2 Pharmacological Therapy: First-Line Drug Classes
Five major drug classes carry Class I recommendations as initial pharmacotherapy for hypertension in the absence of compelling indications for specific agents: ACE inhibitors (ACEi), Angiotensin Receptor Blockers (ARBs), Calcium Channel Blockers (CCBs), Thiazide-type diuretics (particularly chlorthalidone and indapamide), and—in selected patients—beta-blockers [2, 3]. The 2018 ESC/ESH guideline and the ACC/AHA guideline both recommend initiation with a two-drug combination (preferably as a single-pill combination for adherence optimisation) for most patients with Grade 2+ hypertension, based on evidence from the ACCOMPLISH and VALUE trials demonstrating superior blood pressure control and outcomes with combination versus monotherapy.
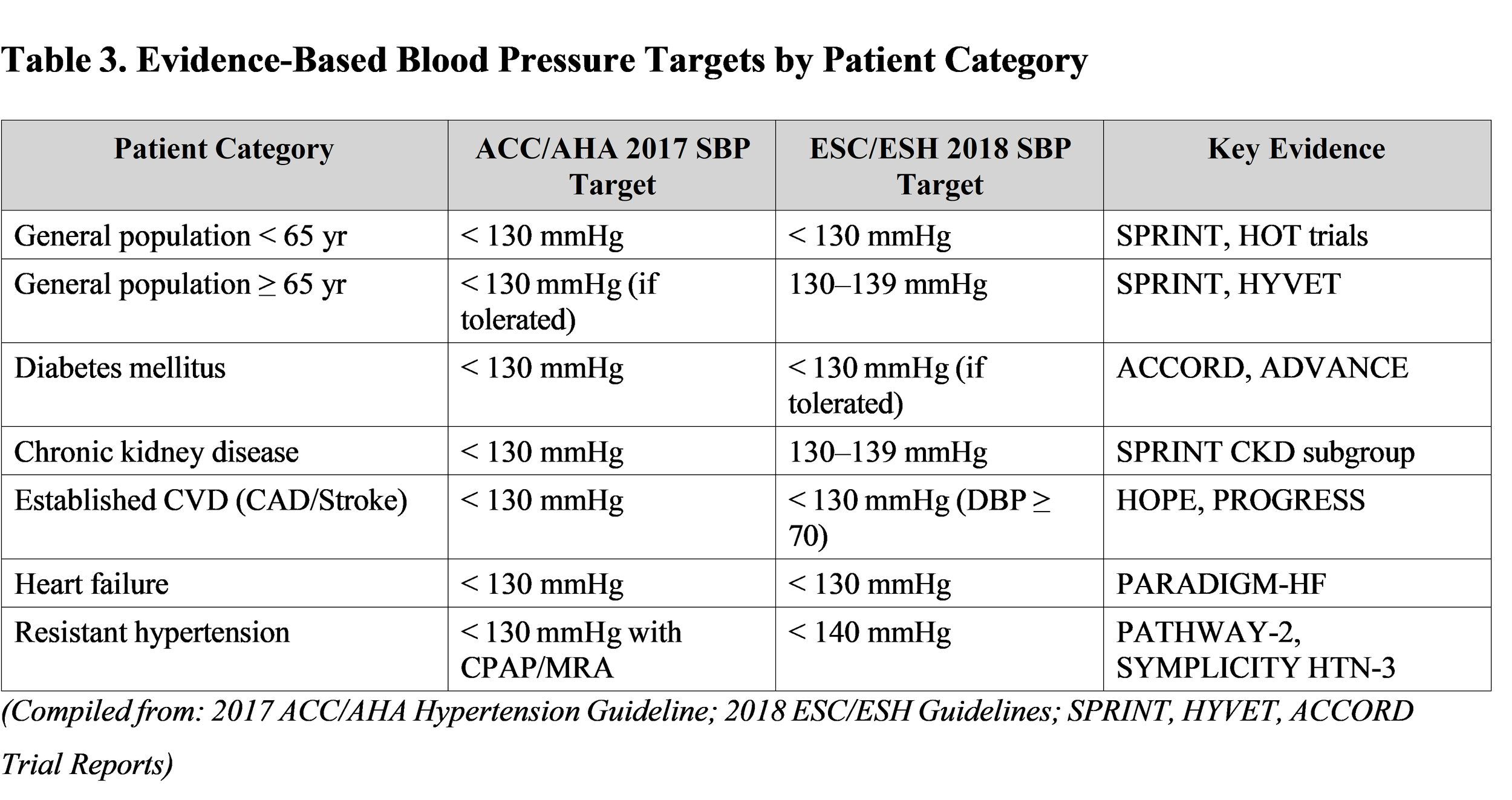
7.3 Blood Pressure Targets: Evidence and Guideline Recommendations
The optimal blood pressure target remains one of the most intensely debated issues in hypertension management. The J-curve hypothesis—suggesting excessive BP lowering may paradoxically increase cardiovascular risk through coronary hypoperfusion—has been refuted for SBP targets by SPRINT and ACCORD, but remains relevant for DBP targets, particularly in patients with CAD (DBP ≥ 60 mmHg recommended). Evidence-based targets are summarised below [2, 3, 8]:
7.4 Combination Therapy Algorithms
The STEP and PATHWAY-2 trials have validated a stepwise combination approach for uncontrolled hypertension. The preferred evidence-based combination backbone is an ACEi or ARB (RAAS blocker) combined with either a CCB or a thiazide-type diuretic as initial two-drug therapy. For patients requiring triple therapy, the ACC/AHA and ESC/ESH both recommend RAAS blocker CCB + thiazide-type diuretic. Mineralocorticoid receptor antagonists (spironolactone 25–50 mg) are the preferred fourth agent for resistant hypertension based on PATHWAY-2 trial evidence, while alpha-1 blockers and beta-blockers serve as alternative add-on agents [3, 11].
8. Evidence-Based Management in Special Populations
8.1 Hypertension in Older Adults
The HYVET trial (n = 3,845) provided the first definitive evidence from an RCT that antihypertensive treatment of patients aged ≥80 years significantly reduces fatal and non-fatal stroke (by 30%), cardiovascular events, and all-cause mortality, dispelling therapeutic nihilism toward treating the oldest patients. A SBP target of 130–145 mmHg is recommended for patients ≥80 years, contingent on frailty assessment and tolerability, as excessive BP lowering in frail older adults increases the risk of falls, syncope, and acute kidney injury [3, 12].
8.3 Hypertension in Diabetes Mellitus
Diabetic patients with hypertension represent an extremely high-risk subgroup requiring a dual strategy of RAAS blockade for both antihypertensive effect and diabetic nephropathy prevention, alongside optimal glycaemic control and statin therapy. The ACCORD-BP trial failed to show benefit for SBP < 120 mmHg versus < 140 mmHg in diabetic patients for the composite primary endpoint, though significant stroke reduction was observed in the intensive arm. Both ACC/AHA and ESC/ESH recommend a SBP target of < 130 mmHg (if tolerated) in diabetic patients, with an ACEi or ARB as mandatory first-line agents due to their proven renoprotective effect beyond blood pressure lowering [2, 3].
8.3 Hypertensive Emergencies
A hypertensive emergency—defined as severely elevated blood pressure (typically ≥ 180/120 mmHg) with acute progressive target organ damage—requires immediate hospitalisation and intravenous antihypertensive therapy. Guideline-recommended initial management mandates reducing mean arterial pressure by no more than 25% within the first hour to avoid critical organ hypoperfusion, followed by gradual titration to 160/100 mmHg over 2–6 hours. Parenteral agents of choice include Nicardipine (5–15 mg/hr IV) for most emergencies, Labetalol (20–80 mg bolus or 0.5–2 mg/min infusion) for hypertensive emergency with acute coronary syndrome or aortic dissection, and Sodium Nitroprusside (0.25–10 mcg/kg/min) for hypertensive encephalopathy with careful cyanide toxicity monitoring [3, 11].
9. Therapeutic Inertia and Implementation of Evidence in Clinical Practice
Despite the robust evidence base for hypertension treatment and the clarity of major guidelines, global blood pressure control rates remain critically suboptimal. The May Measurement Month 2019 global screening initiative found that fewer than 50% of hypertensive patients were on antihypertensive treatment, and only 22% had controlled blood pressure [3]. Therapeutic inertia—defined as failure of healthcare providers to initiate or intensify therapy when treatment goals are not met—is a recognised and quantifiable contributor to this gap. Studies have demonstrated that physicians fail to intensify therapy at up to 87% of clinical encounters where blood pressure is uncontrolled [13].
Evidence-based strategies to overcome therapeutic inertia include the use of standardised single-pill combination formulations (improving adherence by 20–40%), electronic health record-based decision support systems with automatic guideline alerts, pharmacist-led blood pressure titration protocols, and telemedicine-based hypertension management programmes. The ACC/AHA and WHO have emphasised that a system-wide approach—encompassing patient education, healthcare provider training, and health system infrastructure—is required to translate the extraordinary evidence base for hypertension treatment into population-level reductions in cardiovascular mortality [2, 13].
10. Conclusion
Evidence-based medicine has provided cardiology—and the management of arterial hypertension in particular—with a rigorous, reproducible, and patient-centred framework for clinical decision-making. Six decades of landmark randomised controlled trials, from the Veterans Administration Cooperative Study of the 1960s to the SPRINT trial of 2015, have progressively refined our understanding of hypertension diagnosis, risk stratification, blood pressure targets, and pharmacotherapy. The synthesis of this evidence into actionable standards by the ACC/AHA and ESC/ESH guidelines provides clinicians with clear, graded recommendations that translate the best available evidence into individualised patient care. The paramount challenge of the current era is not the generation of further evidence—which is substantial—but the consistent and equitable implementation of existing guideline-concordant care across all healthcare settings globally, with a particular emphasis on overcoming therapeutic inertia and addressing the multifactorial determinants of poor blood pressure control. Achievement of guideline-recommended targets in hypertensive patients represents the single most impactful intervention available to reduce the global burden of cardiovascular disease.
Disclosure of Funding Sources
The authors declare that no specific funding was received for the preparation of this review article. No granting agencies, institutional support, or non-material project frameworks contributed to this work.
10. References
[1] Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: what it is and what it isn’t. British Medical Journal, 312(7023), 71–72. https://doi.org/10.1136/bmj.312.7023.71
[2] Whelton, P. K., Carey, R. M., Aronow, W. S., et al. (2018). 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Journal of the American College of Cardiology, 71(19), e127–e248. https://doi.org/10.1016/j.jacc.2017.11.006
[3] Williams, B., Mancia, G., Spiering, W., et al. (2018). 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal, 39(33), 3021–3104. https://doi.org/10.1093/eurheartj/ehy339
[4] OCEBM Levels of Evidence Working Group. (2011). The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. https://www.cebm.ox.ac.uk/resources/levels-of-evidence
[5] Pickering, T. G., Hall, J. E., Appel, L. J., et al. (2005). Recommendations for Blood Pressure Measurement in Humans and Experimental Animals. Hypertension, 45(1), 142–161. https://doi.org/10.1161/01.HYP.0000150859.47929.8e
[6] Sehestedt, T., Jeppesen, J., Hansen, T. W., et al. (2010). Risk stratification with the ESH/ESC cardiovascular risk stratification tool and the SCORE in the general population. Journal of Hypertension, 28(8), 1700–1709. https://doi.org/10.1097/HJH.0b013e32833b3f2b
[7] ALLHAT Officers and Coordinators. (2002). Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic. JAMA, 288(23), 2981–2997. https://doi.org/10.1001/jama.288.23.2981
[8] Wright, J. T., Williamson, J. D., Whelton, P. K., et al. (2015). A Randomized Trial of Intensive versus Standard Blood-Pressure Control (SPRINT). New England Journal of Medicine, 373(22), 2103–2116. https://doi.org/10.1056/NEJMoa1511939
[9] Yusuf, S., Sleight, P., Pogue, J., et al. (2000). Effects of an Angiotensin-Converting–Enzyme Inhibitor, Ramipril, on Cardiovascular Events in High-Risk Patients (HOPE). New England Journal of Medicine, 342(3), 145–153. https://doi.org/10.1056/NEJM200001203420301
[10] PROGRESS Collaborative Group. (2001). Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. The Lancet, 358(9287), 1033–1041. https://doi.org/10.1016/S0140-6736(01)06178-5
[11] Carey, R. M., Calhoun, D. A., Bakris, G. L., et al. (2018). Resistant Hypertension: Detection, Evaluation, and Management. Hypertension, 72(5), e53–e90. https://doi.org/10.1161/HYP.0000000000000084
[12] Beckett, N. S., Peters, R., Fletcher, A. E., et al. (2008). Treatment of Hypertension in Patients 80 Years of Age or Older (HYVET). New England Journal of Medicine, 358(18), 1887–1898. https://doi.org/10.1056/NEJMoa0801369
[13] Mancia, G., Kreutz, R., Brunström, M., et al. (2023). 2023 ESH Guidelines for the management of arterial hypertension. Journal of Hypertension, 41(12), 1874–2071. https://doi.org/10.1097/HJH.0000000000003480