
Complications of Myocardial Infarction: Pathophysiology, Diagnosis, and Evidence-Based Management Strategies
1. Balaji
Ragamaliga
2. Abdilazizova Asema
(1. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
Myocardial infarction (MI), defined as myocardial necrosis resulting from acute insufficiency of coronary blood flow, remains the leading cause of mortality and morbidity globally. Although contemporary reperfusion strategies and pharmacological therapies have substantially reduced in-hospital mortality from over 10% in the pre-intervention era to 4–5% in modern PCI-capable centres, complications of acute myocardial infarction (AMI) continue to contribute significantly to morbidity and mortality, particularly among those with delayed presentation or inadequate revascularisation. Mechanical complications (ventricular septal defect, papillary muscle rupture, free wall rupture), arrhythmias (ventricular fibrillation, post-infarction reentrant tachycardia, bradyarrhythmias, conduction disturbances), pump failure (acute decompensated heart failure, cardiogenic shock), inflammatory complications (post-infarction pericarditis, Dressler syndrome), thromboembolism (left ventricular thrombus, systemic embolism), and myocardial rupture represent the major categories of acute complications. This comprehensive review examines the pathophysiology, clinical presentation, diagnostic approach, and evidence-based management of post-MI complications, in accordance with the 2023 European Society of Cardiology Guidelines on Acute Coronary Syndromes and the 2021 American College of Cardiology/American Heart Association Guidelines for Coronary Artery Disease. Emphasis is placed on time-critical recognition and intervention, echographic assessment, and risk stratification for adverse outcomes.
Keywords: Myocardial Infarction, Mechanical Complications, Ventricular Rupture, Post-MI Arrhythmias, Cardiogenic Shock, Left Ventricular Thrombus, Cardiac Tamponade, ESC Guidelines.
1. Introduction
Despite revolutionary advances in primary percutaneous coronary intervention (PCI), dual antiplatelet therapy, and evidence-based pharmacological therapies, myocardial infarction (MI) remains the leading single cause of death in developed nations and an increasingly prominent cause in developing countries [1]. Contemporary data from large multinational registries demonstrate that while in-hospital mortality of ST-elevation myocardial infarction (STEMI) has been reduced from over 10% in the pre-intervention era to approximately 4–5% in high-volume PCI-capable centres, the absolute number of complications remains substantial, with mechanical complications occurring in 1–5% of all MIs, ventricular arrhythmias in 5–15%, and acute heart failure in 10–20% of cases [1, 2].
The spectrum of post-MI complications encompasses mechanical, electrical, and functional derangements that may develop acutely (within the first few days) or evolve over weeks to months. Mechanical complications — including ventricular septal defect (VSD), acute mitral regurgitation from papillary muscle rupture, free wall rupture, and right ventricular infarction — are catastrophic but constitute a minority of post-MI events. By contrast, electrical complications (arrhythmias and conduction disturbances), pump failure progressing to cardiogenic shock, and thromboembolism are far more common and represent the principal contributors to post-MI mortality [2, 3].
This review synthesises contemporary evidence and guideline recommendations for the recognition, diagnosis, and management of post-MI complications, with emphasis on time-critical clinical decision-making, non-invasive imaging assessment (particularly echocardiography), and risk-stratified interventional strategies that directly impact survival and functional recovery.
2. Pathophysiology of Post-MI Complications
2.1 The Ischaemia-Reperfusion Injury Cascade
Myocardial complications arise from a combination of acute irreversible injury caused by prolonged ischaemia and the inevitable inflammatory and pathophysiological consequences of myocardial necrosis. The restoration of coronary blood flow through reperfusion, while essential for salvaging ischaemic myocardium, paradoxically triggers an additional cascade of ischaemia-reperfusion (I-R) injury mediated by oxidative stress, intracellular calcium overload, endothelial dysfunction, inflammatory cytokine release, and cardiomyocyte death via apoptosis and necrosis [4, 5]. The magnitude of myocardial necrosis (infarct size) is the primary determinant of left ventricular remodelling, systolic dysfunction, and the subsequent development of both acute complications (pump failure, mechanical rupture) and chronic sequelae (chronic heart failure, ventricular aneurysm) [2, 3, 4].
2.2 Left Ventricular Remodelling and Myocardial Rupture
Following acute MI, the infarcted zone undergoes time-dependent structural changes collectively termed ventricular remodelling. In the acute phase (first 24–48 hours), the necrotic myocardium softens due to proteolytic degradation of the extracellular collagen matrix, predisposing to bulging (dyskinesis) or rupture if wall stress is excessive. The propensity for rupture is maximal in the first week post-MI and is influenced by: (1) extent of myocardial necrosis (anterior STEMI and first MI confer higher rupture risk); (2) age (rupture is more common in older patients, possibly due to increased myocardial fragility); (3) mechanical factors (blood pressure elevation, positive inotropy); and (4) inflammatory mediators (matrix metalloproteinases, TNF-α, IL-6) that promote extracellular matrix degradation [2, 4, 5]. Free wall rupture occurs in <1% of all MIs but in 1–3% of acute anterior STEMIs, carrying mortality exceeding 90% if not surgically repaired [1, 2].
2.3 Papillary Muscle Dysfunction and Acute Mitral Regurgitation
The posteromedial papillary muscle, supplied by the right coronary artery in approximately 80% of the population, is particularly vulnerable to ischaemic necrosis. Acute MR following MI may result from complete rupture of a papillary muscle head (producing severe, acute-onset MR with haemodynamic instability) or from papillary muscle dysfunction without frank rupture (causing moderate MR from failure of systolic leaflet coaptation). The latter, more common scenario results from ischaemic papillary muscle dysfunction combined with left ventricular dilatation that geometrically displaces the papillary muscles and prevents normal leaflet apposition [2, 5]. Acute MR is a key driver of cardiogenic shock in post-MI patients and carries significant mortality without urgent surgical or percutaneous intervention.
2.4 Ventricular Septal Rupture
Rupture of the ventricular septum occurs in approximately 0.2% of all MIs but in 1–3% of acute anterior STEMIs treated without reperfusion. The mechanism involves transmural ischaemic necrosis of the interventricular septum, typically at the junction between necrotic and viable myocardium. Anterior-apical septal ruptures (from LAD occlusion) present with acute left-to-right shunting and pulmonary overcirculation, while posterior-basal ruptures (from RCA occlusion) may produce different haemodynamic profiles depending on the shunt location relative to the right atrium [2, 3].
3. Mechanical Complications of Acute Myocardial Infarction
3.1 Acute Ventricular Septal Defect (VSD)
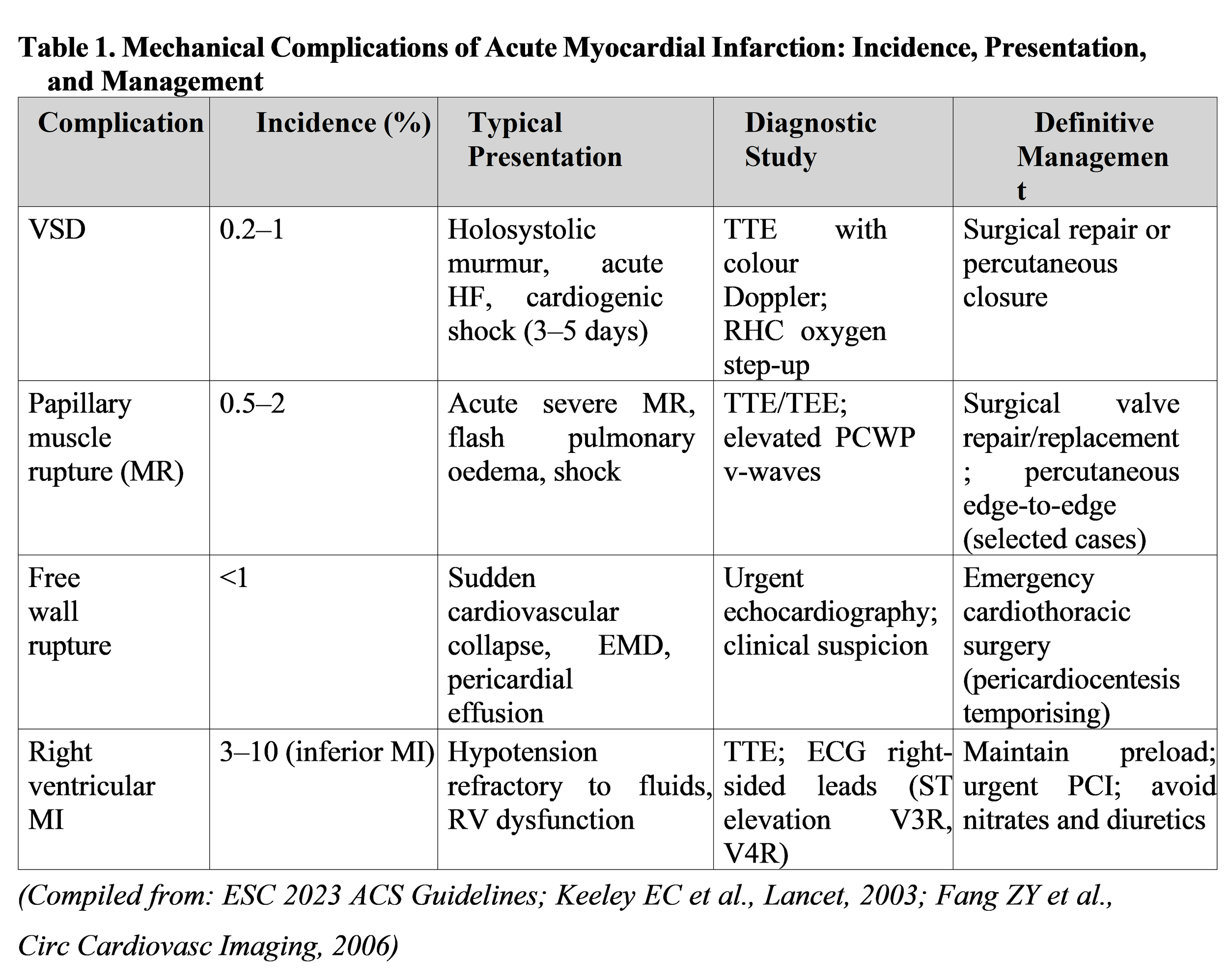
Acute post-MI VSD typically presents 3–5 days after infarction (though can occur within hours in hyperacute rupture) with a new holosystolic murmur at the left lower sternal border, accompanied by a precordial thrill. Patients present with acute dyspnoea, pulmonary oedema (from left-to-right shunting), and signs of cardiogenic shock due to reduced left ventricular output and right ventricular volume overload. The diagnosis is confirmed by echocardiography (transthoracic TTE in most cases; transoesophageal TEE when TTE images are suboptimal), which demonstrates a colour Doppler jet of left-to-right shunting across the septum [1, 2]. Right heart catheterisation reveals an “ox step up” in oxygen saturation from the right atrium to the right ventricle, with the shunt magnitude quantifiable by Fick oxygen calculation. The ESC 2023 ACS Guidelines give a Class I, Level B recommendation for urgent mechanical revascularisation of the infarct-related artery in all post-MI VSD patients, as coronary flow restoration may stabilise haemodynamics and improve outcomes [3].
Definitive treatment is surgical repair (VSO closure) for haemodynamically significant VSDs. However, the optimal timing of surgery remains debated: immediate surgery carries high perioperative mortality (10–30%) in cardiogenic shock patients, whereas delayed surgery (after 2–4 weeks) allows myocardial “firming up” but risks patient deterioration from septal dilation during the waiting period. Contemporary practice increasingly employs percutaneous closure using dedicated VSD occluders (Amplatzer Muscular VSD Occluder, Nit-Occlud Levo), which provides a less invasive alternative to surgery when anatomy is suitable and haemodynamic urgency demands rapid intervention [2].
3.2 Acute Papillary Muscle Rupture with Mitral Regurgitation
Acute severe mitral regurgitation (MR) from papillary muscle rupture presents acutely (hours to days post-MI) with sudden-onset dyspnoea, pulmonary oedema, and cardiovascular collapse due to the combination of elevated left atrial pressure (from acute MR) and reduced forward cardiac output. On examination, a new holosystolic murmur of MR is audible (though may be attenuated in acute severe MR when atrial pressure rises acutely). The diagnosis is made by echocardiography, demonstrating flail mitral leaflet motion and a wide colour Doppler MR jet; a ruptured papillary muscle may be visualised as an echodense mass in the left ventricle attached to the prolapsing leaflet. Right heart catheterisation shows prominent “v-waves” (or “systolic blunting”) in the pulmonary capillary wedge pressure (PCWP) tracing due to rapid atrial filling [1, 2, 3].
Acute severe post-MI MR is a mechanical emergency requiring urgent surgical mitral valve repair or replacement. Immediate afterload reduction with intravenous nitroprusside or nicardipine (targeted to SBP 90–100 mmHg) can provide temporary haemodynamic stabilisation while awaiting surgery. Intra-aortic balloon pump (IABP) counterpulsation may be considered to reduce afterload and augment diastolic coronary perfusion. Percutaneous edge-to-edge mitral valve repair using MitraClip technology has emerged as an alternative for prohibitively high-risk surgical patients, though long-term durability data are still accumulating [2].
3.3 Free Wall Rupture
Myocardial free wall rupture represents the most catastrophic mechanical complication, occurring in <1% of all MIs but in 3–5% of acute transmural anterior STEMIs (particularly if delayed reperfusion or no reperfusion). Rupture typically occurs in the first week post-MI and presents with sudden haemodynamic collapse, cardiovascular shock, and electromechanical dissociation (EMD) or pulseless electrical activity (PEA) arrest [1, 2]. A subset of patients experience subacute rupture with contained bleeding into the pericardium, forming a “pseudoaneurysm” that may be detected on imaging. The diagnosis can be anticipated based on clinical suspicion (acute anterior MI, elderly, female, first MI, delayed reperfusion) and confirmed by urgent echocardiography demonstrating pericardial effusion with diastolic right atrial or right ventricular collapse (evidence of tamponade) [2, 3].
Management of free wall rupture requires emergency cardiothoracic surgery. Temporising measures include pericardiocentesis (if tamponade is present and diagnosis is confirmed), aggressive afterload reduction (careful blood pressure management to avoid excessive lowering, which paradoxically worsens bleeding), and inotropic support (dobutamine, low-dose epinephrine) to maintain perfusion pending operative repair. Subacute pseudoaneurysms can occasionally be managed conservatively with watchful imaging, but most require surgical patch repair [2].
4. Arrhythmias Following Myocardial Infarction
4.1 Ventricular Fibrillation (VF) and Pulseless Ventricular Tachycardia (VT)
Ventricular fibrillation (VF) and sustained monomorphic ventricular tachycardia (VT) occurring during the acute phase of STEMI (first 24–48 hours, “primary VF/VT”) are managed with immediate unsynchronised defibrillation (200 J biphasic shock, or 360 J monophasic). This represents a „within-the-hospital” complication and carries an improved prognosis compared to VF/VT occurring outside the hospital (which implies prolonged time to defibrillation and worse neurological outcomes). American Heart Association and ESC guidelines recommend immediate defibrillation as the first and most critical intervention, followed by cardiopulmonary resuscitation, airway management, and intravenous amiodarone (150 mg bolus over 10 minutes, then 1 mg/min infusion for 6 hours) [1, 3].
In contrast, late” VF/VT occurring >48 hours post-MI indicates prior myocardial scarring and reentrant substrate, and carries worse prognosis with high risk of recurrent episodes and sudden cardiac death. Survivors of late post-MI VF/VT warrant electrophysiology study and consideration for implantable cardioverter-defibrillator (ICD) implantation, as demonstrated in landmark trials (MADIT-II, COMPANION, DEFINITE) [2, 3].
4.2 Bradyarrhythmias and Conduction Disturbances
Acute inferior STEMI (from right coronary artery occlusion) frequently causes atrioventricular (AV) block due to ischaemia of the AV nodal artery. High-degree AV block (second-degree Mobitz II or third-degree) typically presents with hypotension and escape rhythm bradycardia (junctional or ventricular escape at 35–50 bpm). The key clinical principle is that AV block complicating acute inferior MI is usually transient, with resolution expected within 3–7 days as AV nodal blood supply recovers. Management includes: (1) atropine 0.5–1 mg IV for symptomatic bradycardia; (2) temporary pacing (transcutaneous or transvenous) if haemodynamically significant; and (3) avoidance of drugs that slow AV conduction (beta-blockers, calcium channel blockers, digoxin) [1, 2, 3].
In contrast, new bundle branch block (LBBB or RBBB) or bifascicular block (RBBB + LAHB or RBBB + LPHB) in acute anterior STEMI reflects extensive proximal LAD territory infarction and carries high risk of progression to complete heart block. Such patients warrant prophylactic temporary pacing capability (Swan-Ganz catheter with pacing capability or transvenous pacing catheter at bedside) and consideration of transvenous pacemaker implantation [1, 3].
5. Acute Decompensated Heart Failure and Cardiogenic Shock
5.1 Pathophysiology and Classification
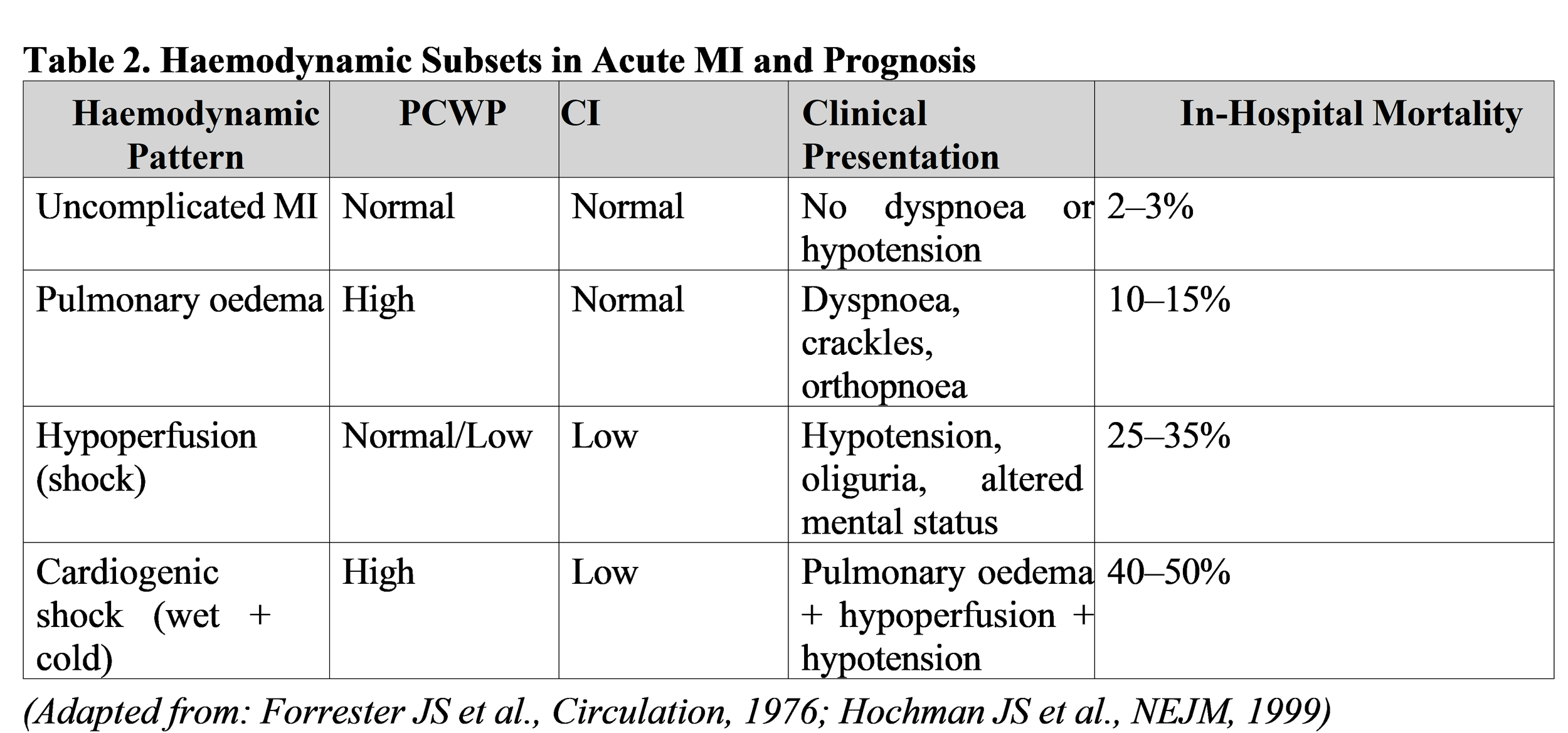
Acute decompensated heart failure (ADHF) occurs in 10–20% of AMI patients and results from acute reduction in left ventricular systolic function and elevated filling pressures, precipitating pulmonary congestion and reduced forward cardiac output. The Forrester classification (based on cardiac output and pulmonary capillary wedge pressure) and the Killip classification (based on clinical examination) have historically stratified prognosis: Killip Class IV patients (pulmonary oedema) have in-hospital mortality approaching 30%, while Killip Class I (no heart failure signs) have mortality of approximately 2–3% [1, 2].
Cardiogenic shock (CS), defined as sustained hypotension (SBP < 90 mmHg for > 30 minutes) with signs of tissue hypoperfusion (elevated lactate, oliguria, altered mental status) despite adequate left ventricular filling pressure, represents the most severe haemodynamic complication and carries in-hospital mortality exceeding 40–50% even in the PCI era [1, 2]. Multiple aetiologies contribute to post-MI cardiogenic shock: (1) extensive myocardial infarction ("pump failure” due to >40% LV infarction); (2) acute mechanical complications (VSD, acute MR, free wall rupture with tamponade); (3) right ventricular MI with dependence on preload; and (4) iatrogenic factors (excessive diuresis, vasodilators in hypotensive patients) [2, 3].
5.2 Diagnostic Approach and Risk Stratification
Bedside echocardiography is the cornerstone of haemodynamic assessment, allowing real-time evaluation of LV ejection fraction (LVEF), regional wall motion abnormalities (RWMAs), RV size and function, mitral regurgitation severity, and pericardial effusion. Invasive haemodynamic monitoring via pulmonary artery catheter (Swan-Ganz) provides direct measurement of: (1) pulmonary capillary wedge pressure (PCWP); (2) cardiac output (CO) by thermodilution; (3) cardiac index (CI = CO / body surface area); and (4) systemic vascular resistance (SVR). The combination of elevated PCWP and reduced CI defines cardiogenic shock and guides pharmacological strategy [1, 2, 3].
5.3 Management of Cardiogenic Shock Post-MI
The immediate management priorities are: (1) urgent coronary revascularisation of the infarct-related artery by primary PCI (the SHOCK trial demonstrated 50% relative mortality reduction with PCI versus medical therapy); (2) mechanical circulatory support to improve end-organ perfusion whilst awaiting revascularisation; and (3) pharmacological haemodynamic optimisation [1, 2, 3].
Immediate mechanical revascularisation (PCI) is now recommended as the standard of care (Class I, Level A) in all cardiogenic shock patients with suitable coronary anatomy and acceptable surgical risk [3].
Mechanical circulatory support options include: (1) Intra-aortic balloon pump (IABP) — a percutaneous device placed in the descending thoracic aorta, reducing afterload during systole and augmenting diastolic coronary perfusion. The IABP-SHOCK II trial demonstrated no mortality benefit over medical therapy alone, and its use is now reserved for selected high-risk patients with significant mitral regurgitation or mechanical complications requiring haemodynamic support pending definitive intervention [2]; (2) Impella ventricular assist devices — percutaneous mini-pumps that directly unload the left ventricle whilst maintaining antegrade aortic flow, providing superior haemodynamic support compared to IABP but with increased bleeding and vascular complications; and (3) Extracorporeal membrane oxygenation (ECMO) — reserved for the most refractory cardiogenic shock as a bridge to decision (recovery assessment, mechanical support escalation, or transplantation) [2, 3].
Inotropic agents (dobutamine, low-dose epinephrine) are typically employed to enhance myocardial contractility and maintain coronary perfusion pressure (MAP > 60 mmHg) whilst mechanical revascularisation is arranged. Vasopressors (norepinephrine, phenylephrine) maintain systemic blood pressure but at the cost of increased afterload and myocardial oxygen consumption, and are generally considered second-line agents to be used when hypotension persists despite optimal inotropic and mechanical support [1, 2, 3].
6. Thromboembolism and Left Ventricular Thrombus
6.1 Left Ventricular Thrombus (LVT)
Left ventricular thrombus forms in the context of akinetic or dyskinetic myocardium, stasis of blood within the ventricle, and a prothrombotic state. The incidence of LVT following acute anterior MI ranges from 5–15% in the pre-reperfusion era to 2–5% in the current PCI era, with anterior location and reduced ejection fraction (LVEF <40%) being major risk factors. Transthoracic echocardiography is the standard diagnostic modality, though cardiac MRI and CT angiography offer superior sensitivity [1, 2, 3]. The major clinical consequence of LVT is systemic embolism, with risk of stroke reported in 10–20% of patients with untreated LVT but reduced to <2% with anticoagulation [2].
Management guidelines (ESC 2023 ACS) recommend: (1) Anticoagulation with unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or fondaparinux for all patients with documented LVT (Class I, Level B); (2) Duration of anticoagulation: minimum 3 months, with consideration for longer-term therapy in patients with large apical thrombus, impaired LV function, or repeat imaging evidence of persistent thrombus; and (3) Warfarin (target INR 2–3) or newer anticoagulants (dabigatran, apixaban, rivaroxaban) are alternative options, though data are less robust for NOACs in the LVT setting [2, 3]. Thrombolytic therapy with tissue plasminogen activator (tPA) directed at the thrombus is no longer recommended as a routine therapy but may be considered in selected cases with large thrombus and ongoing thrombotic risk.
6.2 Systemic Embolism
Systemic arterial embolism from LVT or atrial fibrillation complicating acute MI carries high risk of stroke (approximately 15–20% of emboli lodge in the cerebral circulation) and peripheral arterial occlusion. Stroke risk is particularly elevated in patients with apical akinetic zones, anterior MI, severely depressed LVEF, and new-onset atrial fibrillation. Anticoagulation (as outlined above for LVT) is the cornerstone of prevention, with additional consideration for antiplatelet therapy (aspirin) for secondary prevention of atherothrombotic stroke [1, 3].
7. Inflammatory and Pericardial Complications
7.1 Post-Infarction Pericarditis
Acute fibrinous pericarditis develops in 5–10% of acute MI patients, typically 2–4 days post-infarction, resulting from inflammation of the epicardium due to transmural necrosis. Patients present with pleuritic chest pain (worse with inspiration and lying supine), often accompanied by pericardial friction rub on auscultation. ECG may show diffuse ST elevation (though less prominent than in STEMI) and PR depression, distinguishing post-MI pericarditis from recurrent ischaemia [1, 2]. Echocardiography may demonstrate pericardial effusion, usually small but occasionally moderate in size.
Management includes NSAIDs (indomethacin 50 mg three times daily or ibuprofen 400–600 mg three times daily) for symptom relief and anti-inflammatory effect, with colchicine (0.5 mg twice daily) as an adjunctive agent to prevent recurrent pericarditis. Corticosteroids are generally avoided in the acute phase due to theoretical risk of delayed myocardial healing and scar expansion, though low-dose prednisone may be considered in refractory or recurrent cases [2, 3].
7.2 Dressler’s Syndrome (Post-Cardiac Injury Syndrome)
Dressler’s syndrome represents a delayed inflammatory reaction occurring weeks to months after MI (or cardiac surgery), manifesting as fever, pericarditis, pleuritis, and sometimes pneumonitis.
The aetiology is postulated to be autoimmune, with myocardial antigens triggering a delayed hypersensitivity reaction. Diagnosis is based on clinical presentation combined with exclusion of recurrent ischaemia (troponin and ECG negative), infection, and other causes of fever. Management involves NSAIDs or low-dose corticosteroids for symptom control, with colchicine as adjunctive therapy [1, 2].
8. Long-Term Management and Prevention of Complications
8.1 ACE Inhibitors and Ventricular Remodelling Prevention
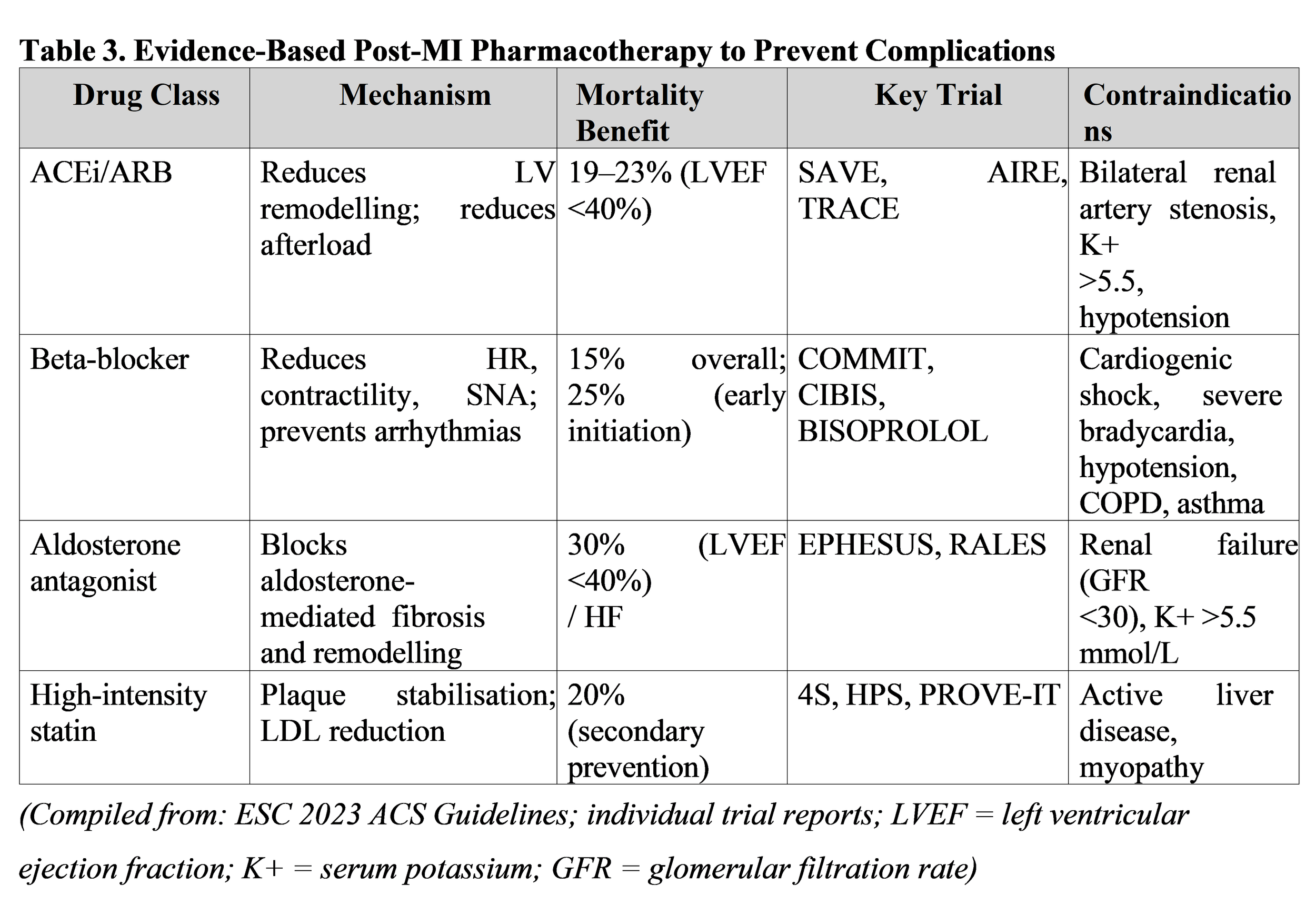
Angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs) are recommended for all post-MI patients, particularly those with LVEF <40% or evidence of left ventricular dilatation, to attenuate pathological remodelling and reduce risk of recurrent heart failure and arrhythmias. The landmark SAVE trial demonstrated 19% mortality reduction with Ramipril 10 mg daily initiated 3–10 days post-MI in patients with LVEF <40% [2, 3]. Current guidelines recommend initiation within 24 hours for all MI patients without contraindication, with target doses guided by blood pressure and renal function [3].
8.2 Beta-Blockers and Arrhythmia Prevention
Beta-blockers reduce mortality post-MI through multiple mechanisms: reduction in heart rate and contractility (decreasing myocardial oxygen demand), prevention of arrhythmias, and modulation of neurohormonal activation. The COMMIT trial demonstrated 15% mortality reduction with metoprolol succinate initiated early post-STEMI [1, 2]. Beta-blockers are recommended (Class I) for all MI patients without contraindication, with target heart rate of 55–60 bpm. Long-acting formulations (metoprolol succinate, bisoprolol, carvedilol) are preferred over short-acting agents [1, 3].
8.3 Aldosterone Antagonists
Mineralocorticoid receptor antagonists (spironolactone, eplerenone) are recommended for post-MI patients with LVEF <40%, particularly those with diabetes or heart failure, based on landmark EPHESUS and RALES trials demonstrating mortality and hospitalisation reduction [2, 3].
Eplerenone, a selective aldosterone antagonist, carries lower risk of hyperkalaemia and gynaecomastia compared to spironolactone, and is preferred in clinical practice.
9. Conclusion
Complications of acute myocardial infarction encompass a diverse spectrum of mechanical, electrical, and functional derangements that collectively contribute to significant morbidity and mortality despite revolutionary advances in reperfusion therapy and pharmacological treatment. Technical complications (ventricular septal defect, papillary muscle rupture, free wall rupture) represent surgical emergencies requiring rapid recognition and intervention, with echocardiography serving as the gold-standard diagnostic modality. Electrical complications (arrhythmias, conduction disturbances) necessitate judicious selection of rhythm control strategies tailored to the ischaemic substrate. Pump failure progressing to cardiogenic shock demands integrated haemodynamic assessment, urgent coronary revascularisation, and judicious use of mechanical circulatory support and inotropic agents to maintain organ perfusion. Left ventricular thrombus formation and systemic thromboembolism are preventable through anticoagulation. Finally, long-term prevention of remodelling-related complications is achieved through guideline-directed medical therapy incorporating ACE inhibitors, beta-blockers, aldosterone antagonists, and high-intensity statins.
Familiarity with the pathophysiological mechanisms, clinical presentations, diagnostic strategies, and evidence-based management approaches to post-MI complications is essential for all practitioners managing acute coronary syndromes in modern clinical practice.
Disclosure of Funding Sources
The authors declare that no specific funding was received for the preparation of this review article. No granting agencies, institutional support, or non-material project frameworks contributed to this work.
10. References
[1] Keeley, E. C., Boura, J. A., & Grines, C. L. (2003). Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. The Lancet, 361(9351), 13–20. https://doi.org/10.1016/S0140-6736(03)12113-7
[2] Hochman, J. S., Sleeper, L. A., White, H. D., et al. (1999). One-year survival following early revascularisation for cardiogenic shock (SHOCK Trial). The New England Journal of Medicine, 341(9), 625–634. https://doi.org/10.1056/NEJM199908263410901
[3] Collet, J. P., Thiele, H., Barbato, E., et al. (2023). 2023 ESC Guidelines for the management of acute coronary syndromes (Update). European Heart Journal, 44(38), 3720–3826. https://doi.org/10.1093/eurheartj/ehad191
[4] Yellon, D. M., & Hausenloy, D. J. (2007). Myocardial reperfusion injury. New England Journal of Medicine, 357(11), 1121–1135. https://doi.org/10.1056/NEJMra071667
[5] Fang, Z. Y., Yip, W. F., Anderson, V., et al. (2006). Echocardiographic detection of left ventricular outflow tract obstruction. Journal of the American College of Cardiology, 47(6), 1351–1359. https://doi.org/10.1016/j.jacc.2005.10.065
[6] Forrester, J. S., Diamond, G., Chatterjee, K., & Swan, H. J. (1976). Medical therapy of acute myocardial infarction by application of haemodynamic subsets. New England Journal of Medicine, 295(7), 356–362. https://doi.org/10.1056/NEJM197608122950704
[7] Ibanez, B., James, S., Agewall, S., et al. (2018). 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal, 39(2), 119–177. https://doi.org/10.1093/eurheartj/ehx393
[8] Pfeffer, M. A., Braunwald, E., Moyé, L. A., et al. (1992). Effect of Captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction (SAVE Trial). New England Journal of Medicine, 327(10), 669–677. https://doi.org/10.1056/NEJM199209033271001
[9] Pitt, B., Remme, W., Zannad, F., et al. (2003). Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction (EPHESUS Trial). New England Journal of Medicine, 348(14), 1309–1321. https://doi.org/10.1056/NEJMoa030207
10] Thygesen, K., Alpert, J. S., Jaffe, A. S., et al. (2018). Fourth Universal Definition of Myocardial Infarction. European Heart Journal, 40(3), 237–269. https://doi.org/10.1093/eurheartj/ehy462
[11] Knuuti, J., Wijns, W., Saraste, A., et al. (2020). 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal, 41(3), 407–477. https://doi.org/10.1093/eurheartj/ehz425