
Methodological recommendations, standards for diagnosis and treatment of Chronic clinical forms of Chronic Forms of Coronary Heart Diseases: Heart Failure
1. Adesh Radheshyam Sharnagat
1. Rahul Ramchandra Mestry
1. Rupesh Chaurasiya
2. Aizhamal Esengeldi kyzy
(1. Students, International Medical Faculty, Osh State University, Kyrgyz Republic)
(2. Associate Professor, International Medical Faculty, Osh State University, Kyrgyz Republic)
Abstract
Chronic coronary syndromes represent a range of cardiovascular disease that frequently culminates in heart failure, one of the most debilitating and prognostically significant complications of atherosclerotic coronary artery disease. The intersection of chronic ischemic heart disease and heart failure presents unique diagnostic and therapeutic challenges that demand a comprehensive, evidence-based approach grounded in contemporary guideline recommendations. This review synthesizes current methodological standards for the diagnosis and treatment of heart failure arising in the context of chronic coronary syndromes, with particular emphasis on the 2024 European Society of Cardiology guidelines for chronic coronary syndrome management, the 2022 American Heart Association-American College of Cardiology-Heart Failure Society of America and 2024 Chinese guidelines for heart failure, and the emerging paradigm of quadruple guideline-directed medical therapy. We examine the diagnostic algorithms that integrate clinical assessment, biomarker evaluation, and multimodal imaging for accurate phenotyping of heart failure with reduced, mildly reduced, and preserved ejection fraction in patients with chronic coronary disease. The review provides detailed analysis of pharmacological strategies including renin-angiotensin system inhibitors, beta-blockers, mineralocorticoid receptor antagonists, and sodium-glucose cotransporter-2 inhibitors as the foundational quadruple therapy, alongside antianginal agents, antithrombotic therapy, and lipid-lowering strategies. Revascularization considerations, device therapy indications, and the management of comorbidities including diabetes, obesity, and iron deficiency are discussed. By integrating recent clinical trial evidence with practical implementation strategies, this article provides a comprehensive framework for clinicians managing the complex interplay between chronic coronary syndromes and heart failure.
1. Introduction
The relationship between chronic coronary artery disease and heart failure represents one of the most clinically significant intersections in cardiovascular medicine, affecting millions of patients worldwide and imposing an enormous burden on healthcare systems. Coronary artery disease remains the predominant etiology of heart failure across all ejection fraction phenotypes, with ischemic cardiomyopathy accounting for more than sixty percent of congestive heart failure cases in Western populations. The pathophysiological link between these conditions is multifaceted, encompassing myocardial infarction with subsequent adverse remodeling, chronic ischemia leading to hibernating and stunned myocardium, repetitive episodes of subclinical ischemic injury, and the progressive accumulation of atherosclerotic burden that compromises coronary flow reserve. Understanding this pathophysiological continuum is essential for clinicians, as the presence of coronary artery disease fundamentally alters both the diagnostic approach and therapeutic strategy in patients presenting with heart failure symptoms.
The clinical landscape of chronic coronary syndromes has evolved considerably since the 2019 European Society of Cardiology guidelines redefined stable coronary artery disease as chronic coronary syndrome, emphasizing the dynamic nature of atherosclerotic disease and its potential for acute transformation. This conceptual shift recognizes that the coronary plaque burden accumulates gradually, producing myocardial ischemia through supply-demand mismatch during physical or emotional stress, while maintaining the ever-present risk of plaque rupture or erosion that precipitates acute coronary syndromes. When chronic coronary syndromes progress to heart failure, the clinical complexity increases substantially, requiring integration of management strategies for both conditions while addressing the unique pathophysiology of ischemic cardiomyopathy. The 2024 ESC guidelines for chronic coronary syndromes and the contemporary heart failure guidelines from major cardiovascular societies provide an evidence-based framework for navigating this complexity, though significant gaps between guideline recommendations and real-world practice persist.
Heart failure in the context of chronic coronary disease presents across the full spectrum of ejection fraction phenotypes, each with distinct pathophysiological mechanisms and therapeutic implications. Heart failure with reduced ejection fraction, defined by a left ventricular ejection fraction of forty percent or less, most directly reflects the consequences of myocardial infarction and adverse remodeling, with extensive evidence supporting neurohormonal antagonism as the cornerstone of therapy. Heart failure with mildly reduced ejection fraction, with ejection fraction between forty-one and forty-nine percent, represents an increasingly recognized intermediate phenotype that shares therapeutic responsiveness with both reduced and preserved ejection fraction categories. Heart failure with preserved ejection fraction, with ejection fraction of fifty percent or greater, is particularly prevalent among patients with chronic coronary disease and multiple comorbidities, and has historically presented the greatest therapeutic challenge, though recent breakthroughs with sodium-glucose cotransporter-2 inhibitors have finally established evidence-based treatment options. The accurate phenotyping of heart failure in patients with chronic coronary syndromes is therefore essential for appropriate therapeutic selection.
The therapeutic armamentarium for heart failure with chronic coronary disease has expanded dramatically in recent years, most notably with the establishment of quadruple guideline-directed medical therapy as the standard of care for heart failure with reduced ejection fraction. This paradigm, comprising renin-angiotensin system inhibitors, evidence-based beta-blockers, mineralocorticoid receptor antagonists, and sodium-glucose cotransporter-2 inhibitors, has been shown to reduce all-cause mortality by approximately seventy-three percent when implemented comprehensively, representing one of the most impactful therapeutic advances in cardiovascular medicine. Yet despite this remarkable efficacy, real-world implementation remains suboptimal, with studies demonstrating that only fifteen percent of eligible patients receive quadruple therapy and that significant gaps exist in both inpatient initiation and outpatient titration of these life-saving medications. Addressing these implementation gaps is as critical as understanding the pharmacological mechanisms themselves.
This review aims to provide a comprehensive synthesis of methodological recommendations and standards for the diagnosis and treatment of heart failure in the context of chronic coronary syndromes, organized according to the IMRAD framework. We begin with the diagnostic approach, integrating clinical assessment, biomarker evaluation, and multimodal imaging strategies. We then examine the pharmacological management of heart failure across ejection fraction phenotypes, with detailed attention to quadruple therapy implementation, antianginal therapy, and antithrombotic strategies. Revascularization considerations, device therapy indications, and the management of acute decompensation are discussed. The review addresses comorbidity management, including diabetes, obesity, iron deficiency, and atrial fibrillation, which frequently complicate the clinical course. Throughout, we emphasize the integration of contemporary guideline recommendations with practical strategies for overcoming barriers to optimal care delivery.
2. Materials and Methods
This review was conducted through a comprehensive and systematic search of the published literature, with particular emphasis on peer-reviewed articles, clinical practice guidelines, systematic reviews, and meta-analyses indexed in PubMed/MEDLINE, the Cochrane Library, and relevant cardiology journals. The search strategy employed a combination of MeSH terms and free-text keywords including "chronic coronary syndrome," "heart failure," "guideline-directed medical therapy," "quadruple therapy," "SGLT2 inhibitors," "ARNI," "sacubitril-valsartan," "beta-blockers," "mineralocorticoid receptor antagonists," "revascularization," "coronary artery bypass grafting," "percutaneous coronary intervention," "heart failure with reduced ejection fraction," "heart failure with preserved ejection fraction," "diagnosis," "natriuretic peptides," "echocardiography," "cardiac MRI," "stress testing," "iron deficiency," "diabetes," "obesity," "atrial fibrillation," and "cardiac resynchronization therapy." The search was restricted to articles published in English, with priority given to publications from 2022 to 2026 to ensure currency, though seminal earlier works were included where essential for foundational concepts.
The selection criteria favored clinical practice guidelines from major cardiovascular societies including the European Society of Cardiology, American Heart Association, American College of Cardiology, Heart Failure Society of America, and the Chinese Society of Cardiology. Landmark randomized controlled trials that have shaped contemporary practice were prioritized, including DAPA-HF, EMPEROR-Reduced, EMPEROR-Preserved, DELIVER, PARADIGM-HF, PARAGON-HF, TOPCAT, STICH, and REVIVED-BCIS2. Systematic reviews and meta-analyses evaluating therapeutic strategies were included where they provided comprehensive synthesis of available evidence. Data extraction focused on diagnostic criteria, therapeutic recommendations with class and level of evidence, outcome measures including mortality and heart failure hospitalization, safety considerations, and implementation strategies. Where conflicting evidence existed between guidelines, we prioritized the most recent recommendations and acknowledged areas of ongoing debate or uncertainty. The synthesis of evidence was organized thematically to construct an integrated narrative highlighting the interconnectedness of diagnostic and therapeutic approaches in this patient population.
3. Results
3.1 Diagnostic Approach to Heart Failure in Chronic Coronary Syndromes
The diagnosis of heart failure in patients with chronic coronary syndromes requires a systematic approach that integrates clinical evaluation, biomarker assessment, and cardiac imaging to establish the presence of heart failure, determine its phenotypic classification, identify underlying etiology, and guide therapeutic decision-making. The clinical presentation of heart failure in patients with chronic coronary disease is often insidious, with symptoms developing gradually as cardiac function deteriorates. Dyspnea on exertion, fatigue, and reduced exercise tolerance are the cardinal symptoms, though patients may also present with angina, palpitations, or symptoms of right heart failure including peripheral edema and abdominal distension. The overlap between symptoms of coronary ischemia and heart failure can complicate clinical assessment, as exertional dyspnea may reflect either angina equivalent or pulmonary congestion, requiring careful differentiation through targeted evaluation.
The initial clinical assessment should include a detailed history focusing on cardiovascular risk factors, prior myocardial infarction or revascularization procedures, symptom progression, and functional capacity. Physical examination should evaluate for signs of congestion including elevated jugular venous pressure, pulmonary rales, hepatomegaly, and peripheral edema, as well as signs of low cardiac output such as cool extremities, narrow pulse pressure, and altered mental status. The presence of a displaced apical impulse, third heart sound, or murmurs of mitral regurgitation or tricuspid regurgitation provides additional diagnostic clues. Blood pressure, heart rate, and oxygen saturation should be measured, as these parameters influence both diagnostic interpretation and therapeutic selection. The New York Heart Association functional classification should be assigned to quantify symptom severity and track therapeutic response.
Biomarker evaluation is essential for the diagnosis and prognostic assessment of heart failure. Natriuretic peptides, including B-type natriuretic peptide and N-terminal pro-B-type natriuretic peptide, are released in response to myocardial wall stress and serve as sensitive markers of heart failure. Elevated levels support the diagnosis, while normal levels have high negative predictive value for excluding heart failure. However, natriuretic peptide levels must be interpreted in context, as they are influenced by age, renal function, body mass index, and atrial fibrillation. The diagnostic thresholds vary across guidelines, with the 2024 Chinese guidelines recommending NT-proBNP levels greater than 125 pg/mL for the diagnosis of heart failure in non-acute settings, while higher thresholds are applied in acute presentations. In patients with chronic coronary syndromes, natriuretic peptide levels provide prognostic information independent of ejection fraction, with higher levels predicting increased risk of cardiovascular death and heart failure hospitalization.
Troponin measurement is important in patients with chronic coronary syndromes and suspected heart failure, as elevated troponin levels may indicate ongoing myocardial injury, whether from recurrent ischemia, microvascular dysfunction, or myocardial strain. Persistent troponin elevation in chronic heart failure is associated with worse prognosis and may guide decisions regarding intensification of anti-ischemic therapy or evaluation for revascularization. Complete blood count, renal function, electrolytes, liver function tests, thyroid function, and lipid profile should be obtained as part of the baseline evaluation, as these parameters influence both heart failure management and coronary risk stratification. Iron studies are increasingly recognized as essential, given the high prevalence of iron deficiency in heart failure and the therapeutic implications for intravenous iron supplementation.
Electrocardiography provides important diagnostic and prognostic information in patients with chronic coronary syndromes and heart failure. The presence of pathological Q waves suggests prior myocardial infarction, while ST-segment and T-wave abnormalities may indicate ongoing ischemia or ventricular strain. Left bundle branch block or prolonged QRS duration identifies candidates for cardiac resynchronization therapy. Atrial fibrillation, present in a substantial proportion of patients with heart failure and chronic coronary disease, influences both therapeutic strategy and anticoagulation decisions. The 2024 ESC guidelines for chronic coronary syndromes emphasize that a twelve-lead electrocardiogram should be obtained in all patients with suspected coronary artery disease, as it can identify arrhythmias, conduction abnormalities, and signs of prior infarction that inform subsequent management.
Echocardiography remains the cornerstone of cardiac imaging in heart failure, providing essential information on left ventricular ejection fraction, chamber dimensions, wall motion abnormalities, valvular function, and hemodynamic parameters. The measurement of left ventricular ejection fraction is critical for phenotypic classification and determines eligibility for many evidence-based therapies. Echocardiographic assessment should include evaluation of left ventricular wall motion to identify territories of prior infarction or ischemia, measurement of left atrial size and function, assessment of right ventricular size and function, estimation of pulmonary artery pressures, and evaluation for intracardiac thrombus. Doppler assessment of mitral inflow patterns, tissue Doppler imaging of the mitral annulus, and measurement of the E/e' ratio provide information on diastolic function that is particularly relevant in heart failure with preserved ejection fraction. The 2024 Chinese heart failure guidelines recommend echocardiography as the initial imaging modality for all patients with suspected heart failure, with additional imaging reserved for cases where diagnosis remains uncertain or further characterization is needed.
Stress echocardiography plays a particularly important role in patients with chronic coronary syndromes and heart failure, as it enables the assessment of myocardial ischemia, viability, and contractile reserve. Exercise stress echocardiography, when feasible, simulates physiological conditions and provides information on functional capacity, hemodynamic response, and ischemia-induced wall motion abnormalities. In patients unable to exercise, pharmacological stress with dobutamine or vasodilators such as adenosine or regadenoson can be employed. Dobutamine stress echocardiography is particularly valuable for assessing myocardial viability, as the biphasic response—improvement in wall motion at low doses followed by deterioration at high doses—identifies hibernating myocardium that may recover function following revascularization. Vasodilator stress echocardiography, combined with myocardial contrast perfusion imaging, enables assessment of coronary flow reserve and microvascular function, which may be particularly relevant in patients with non-obstructive coronary artery disease. The 2024 Chinese guidelines recommend stress echocardiography for patients with heart failure and coronary artery disease to evaluate myocardial ischemia and viability before decisions regarding revascularization.
Coronary computed tomography angiography has emerged as a powerful non-invasive tool for anatomical assessment of coronary artery disease, with high sensitivity for detecting obstructive coronary lesions and the ability to characterize plaque composition. In patients with chronic coronary syndromes and heart failure, CCTA can establish the presence and extent of coronary disease, identify high-risk plaque features such as low attenuation and positive remodeling, and guide decisions regarding invasive angiography and revascularization. The SCOT-HEART trial demonstrated that CCTA-based management reduced coronary events compared to standard care, with a hazard ratio of 0.59. However, CCTA is limited by calcium artifact in heavily calcified vessels, which is common in patients with chronic coronary disease, and by the need for heart rate control and contrast administration. The 2024 ESC guidelines recommend CCTA as a first-line test for ruling out obstructive coronary artery disease in patients with low-to-moderate pre-test probability, while functional testing is preferred for higher-risk patients and those with established coronary disease.
Cardiovascular magnetic resonance imaging provides comprehensive assessment of cardiac structure, function, and tissue characterization without ionizing radiation. Late gadolinium enhancement identifies myocardial scar from prior infarction, with patterns of subendocardial or transmural enhancement corresponding to coronary territories. T1 mapping and extracellular volume quantification enable detection of diffuse myocardial fibrosis, which contributes to diastolic dysfunction in heart failure with preserved ejection fraction. CMR perfusion imaging assesses myocardial ischemia with high diagnostic accuracy, while stress CMR with dobutamine or vasodilators evaluates contractile reserve and perfusion. The 2024 ESC guidelines recognize CMR as a valuable tool for assessing myocardial viability, detecting alternative etiologies of heart failure such as myocarditis or infiltrative disease, and providing prognostic information through scar burden quantification. In patients with chronic coronary syndromes and heart failure, CMR is particularly useful when echocardiographic image quality is suboptimal or when tissue characterization is needed to guide therapeutic decisions.
Invasive coronary angiography remains the gold standard for anatomical assessment of coronary artery disease and is indicated in patients with high pre-test probability of obstructive disease, severe symptoms despite optimal medical therapy, angina at low levels of activity, or high risk of major adverse cardiovascular events. In patients with heart failure and known or suspected coronary artery disease, coronary angiography establishes the extent and severity of coronary lesions, identifies left main or proximal disease that may benefit from revascularization, and guides percutaneous or surgical intervention. The 2024 ESC guidelines recommend invasive angiography when non-invasive testing is inconclusive or when revascularization is being considered, with functional assessment of intermediate stenoses using fractional flow reserve or instantaneous wave-free ratio to guide intervention decisions.
3.2 Phenotypic Classification and Clinical Implications
The classification of heart failure by left ventricular ejection fraction is fundamental to therapeutic decision-making in patients with chronic coronary syndromes. Heart failure with reduced ejection fraction, defined by left ventricular ejection fraction of forty percent or less, is characterized by impaired systolic function and has the most extensive evidence base for neurohormonal antagonism. In patients with chronic coronary disease, HFrEF most commonly results from prior myocardial infarction with adverse left ventricular remodeling, though chronic ischemia and repetitive injury also contribute. The pathophysiology involves activation of the renin-angiotensin-aldosterone system and sympathetic nervous system, leading to vasoconstriction, sodium retention, ventricular hypertrophy, and progressive fibrosis. Neurohormonal antagonism with angiotensin receptor-neprilysin inhibitors, beta-blockers, mineralocorticoid receptor antagonists, and sodium-glucose cotransporter-2 inhibitors directly targets these pathophysiological mechanisms and forms the foundation of therapy.
Heart failure with mildly reduced ejection fraction, with ejection fraction between forty-one and forty-nine percent, represents an intermediate phenotype that has gained increasing recognition. Patients with HFmrEF often have mixed systolic and diastolic dysfunction, with clinical features overlapping both HFrEF and HFpEF. The therapeutic approach to HFmrEF has historically been uncertain, but recent evidence from the DELIVER and EMPEROR-Preserved trials, which included patients with ejection fractions above forty percent, has established the efficacy of sodium-glucose cotransporter-2 inhibitors across the full spectrum of ejection fraction. The 2024 Chinese guidelines and contemporary international guidelines now recommend SGLT2 inhibitors for HFmrEF, with consideration of other therapies based on individual patient characteristics.
Heart failure with preserved ejection fraction, with ejection fraction of fifty percent or greater, is the most prevalent form of heart failure in patients with chronic coronary syndromes, particularly among elderly patients with multiple comorbidities. The pathophysiology of HFpEF is heterogeneous, involving left ventricular diastolic dysfunction, left atrial dysfunction, pulmonary vascular disease, right ventricular dysfunction, and systemic inflammation. In patients with chronic coronary disease, HFpEF may result from ischemic diastolic dysfunction, concentric left ventricular hypertrophy, or microvascular disease. The diagnosis of HFpEF is challenging, requiring demonstration of elevated left ventricular filling pressures, and algorithms such as HFA-PEFF and H2FPEF have been developed to standardize diagnostic evaluation. Until recently, no pharmacotherapy had demonstrated definitive benefit in HFpEF, but the landmark DELIVER and EMPEROR-Preserved trials established SGLT2 inhibitors as the first evidence-based therapy, with dapagliflozin and empagliflozin both demonstrating reductions in the composite endpoint of cardiovascular death or heart failure worsening.
3.3 Guideline-Directed Medical Therapy: The Quadruple Foundation
The pharmacological management of heart failure with reduced ejection fraction in patients with chronic coronary syndromes is anchored by quadruple guideline-directed medical therapy, comprising four drug classes that target distinct pathophysiological pathways and have demonstrated mortality benefit in large randomized controlled trials. The 2022 AHA-ACC-HFSA guidelines, the 2024 Chinese guidelines, and contemporary European guidance all recommend this quadruple therapy as the cornerstone of treatment for HFrEF, unless contraindicated or not tolerated. When implemented comprehensively and titrated to target doses, quadruple therapy has been shown to reduce all-cause mortality by seventy-three percent compared to no treatment, representing one of the most impactful therapeutic advances in cardiovascular medicine.
Renin-angiotensin system inhibitors form the first pillar of quadruple therapy. Angiotensin-converting enzyme inhibitors were the first class to demonstrate mortality benefit in HFrEF, with landmark trials including CONSENSUS and SOLVD establishing their role in reducing mortality and heart failure hospitalization. Angiotensin receptor blockers provide an alternative for patients intolerant to ACE inhibitors, with comparable efficacy in reducing cardiovascular events. The introduction of sacubitril-valsartan, an angiotensin receptor-neprilysin inhibitor, represented a significant advance, with the PARADIGM-HF trial demonstrating superiority over enalapril in reducing cardiovascular death and heart failure hospitalization. Sacubitril-valsartan inhibits neprilysin, increasing levels of natriuretic peptides that promote vasodilation, natriuresis, and antifibrotic effects, while simultaneously blocking angiotensin II receptors to prevent the deleterious effects of renin-angiotensin system activation. The 2024 Chinese guidelines recommend sacubitril-valsartan as a preferred option for HFrEF, with starting doses of 24/26 mg or 49/51 mg twice daily depending on prior ACE inhibitor or ARB exposure, titrated to the target dose of 97/103 mg twice daily as tolerated.
Beta-blockers constitute the second pillar and are essential for all patients with HFrEF unless contraindicated. Three beta-blockers have demonstrated mortality benefit in HFrEF: bisoprolol, carvedilol, and metoprolol succinate. These agents antagonize sympathetic nervous system activation, reduce heart rate, improve ventricular filling, and reverse adverse remodeling. Beta-blockers should be initiated at low doses and titrated gradually to target doses, with monitoring for heart rate, blood pressure, and signs of worsening heart failure. The 2024 Chinese guidelines recommend bisoprolol starting at 1.25 mg daily with titration to 10 mg daily, carvedilol starting at 3.125 mg twice daily with titration to 25 mg twice daily, or metoprolol succinate starting at 23.75 mg daily with titration to 190 mg daily. In patients with chronic coronary syndromes, beta-blockers also provide anti-ischemic benefits by reducing myocardial oxygen demand, making them particularly valuable in patients with concomitant angina.
Mineralocorticoid receptor antagonists form the third pillar and are recommended for all patients with HFrEF unless contraindicated by hyperkalemia or severe renal dysfunction. Spironolactone and eplerenone have demonstrated mortality benefit in HFrEF, with additional benefits in reducing heart failure hospitalization and improving functional status. More recently, finerenone, a nonsteroidal mineralocorticoid receptor antagonist, has been approved for heart failure based on the FINEARTS-HF trial, which demonstrated benefit in patients with heart failure with mildly reduced or preserved ejection fraction. The 2024 Chinese guidelines recommend spironolactone starting at 20 mg daily with titration to the target dose as tolerated, with careful monitoring of potassium and renal function. In patients with chronic coronary disease, mineralocorticoid receptor antagonists may provide additional anti-remodeling benefits and have been shown to reduce sudden cardiac death.
Sodium-glucose cotransporter-2 inhibitors represent the fourth and most recently established pillar of quadruple therapy, with benefit demonstrated across the full spectrum of ejection fraction and irrespective of diabetes status. Dapagliflozin and empagliflozin are the SGLT2 inhibitors currently approved for heart failure, with both demonstrating reductions in cardiovascular death and heart failure hospitalization in HFrEF. The DAPA-HF trial demonstrated that dapagliflozin reduced the composite endpoint of cardiovascular death, heart failure hospitalization, or urgent heart failure visit by twenty-six percent in patients with HFrEF, while the EMPEROR-Reduced trial showed that empagliflozin reduced cardiovascular death or heart failure hospitalization by twenty-five percent. In HFpEF, the DELIVER trial demonstrated that dapagliflozin reduced the composite endpoint of cardiovascular death or worsening heart failure by eighteen percent, while the EMPEROR-Preserved trial showed that empagliflozin reduced cardiovascular death or heart failure hospitalization by twenty-one percent. These benefits are observed early after treatment initiation, within fourteen days for HFrEF and twenty-eight days for HFpEF, supporting prompt initiation during hospitalization or in the outpatient setting. The 2024 Chinese guidelines and international guidelines recommend SGLT2 inhibitors as foundational therapy for all heart failure patients, with a fixed dose of 10 mg daily for both dapagliflozin and empagliflozin, requiring no dose titration or routine laboratory monitoring.
3.4 Implementation Strategies for Quadruple Therapy
Despite the compelling evidence for quadruple therapy, real-world implementation remains suboptimal, with studies demonstrating that only fifteen percent of eligible patients receive all four pillars and that significant gaps exist in both initiation and titration. The 2024 Chinese guidelines emphasize that all patients diagnosed with HFrEF should receive evidence-based pharmacological therapy as early as possible, with quadruple therapy recommended as the cornerstone unless contraindicated or intolerable. For patients presenting with symptoms and signs of congestion, diuretics should be administered initially to alleviate fluid retention, as patients in a congested state exhibit better tolerance to renin-angiotensin system inhibitors, mineralocorticoid receptor antagonists, and SGLT2 inhibitors. Conversely, if there is no significant edema and the resting heart rate is increased, beta-blockers may be better tolerated as initial therapy.
During the optimization phase, medications with different mechanisms of action should be combined for initial therapy and gradually titrated to their target or maximally tolerated doses to maximize patient benefit. Continuous monitoring of symptoms, signs, blood pressure, heart rate, renal function, and electrolytes is essential during titration. The STRONG-HF trial demonstrated that rapid uptitration of guideline-directed medical therapy, with close follow-up in the first six weeks, reduced symptoms, improved quality of life, and decreased the risk of readmission. However, this approach requires robust infrastructure for frequent monitoring and may not be suitable for all patients, particularly those who are frail or have marginal blood pressure or renal function. The 2025 NICE guidelines have moved away from rigid sequencing of medication introduction, instead recommending that clinicians use patient history, clinical assessment, frailty status, prognosis, and preferences to guide decisions on which medications to initiate, in what order, and at what pace.
Following initial treatment, patients should undergo clinical evaluation to determine the need for advanced therapies including implantable cardioverter-defibrillators, cardiac resynchronization therapy, vericiguat, ivabradine, or digoxin based on their clinical status. For patients who progress to end-stage heart failure despite comprehensive medical therapy, options include heart transplantation, palliative care, or left ventricular assist device implantation, tailored to the individual patient's condition, preferences, and goals of care.
3.5 Antianginal and Antithrombotic Therapy in Chronic Coronary Syndromes with Heart Failure
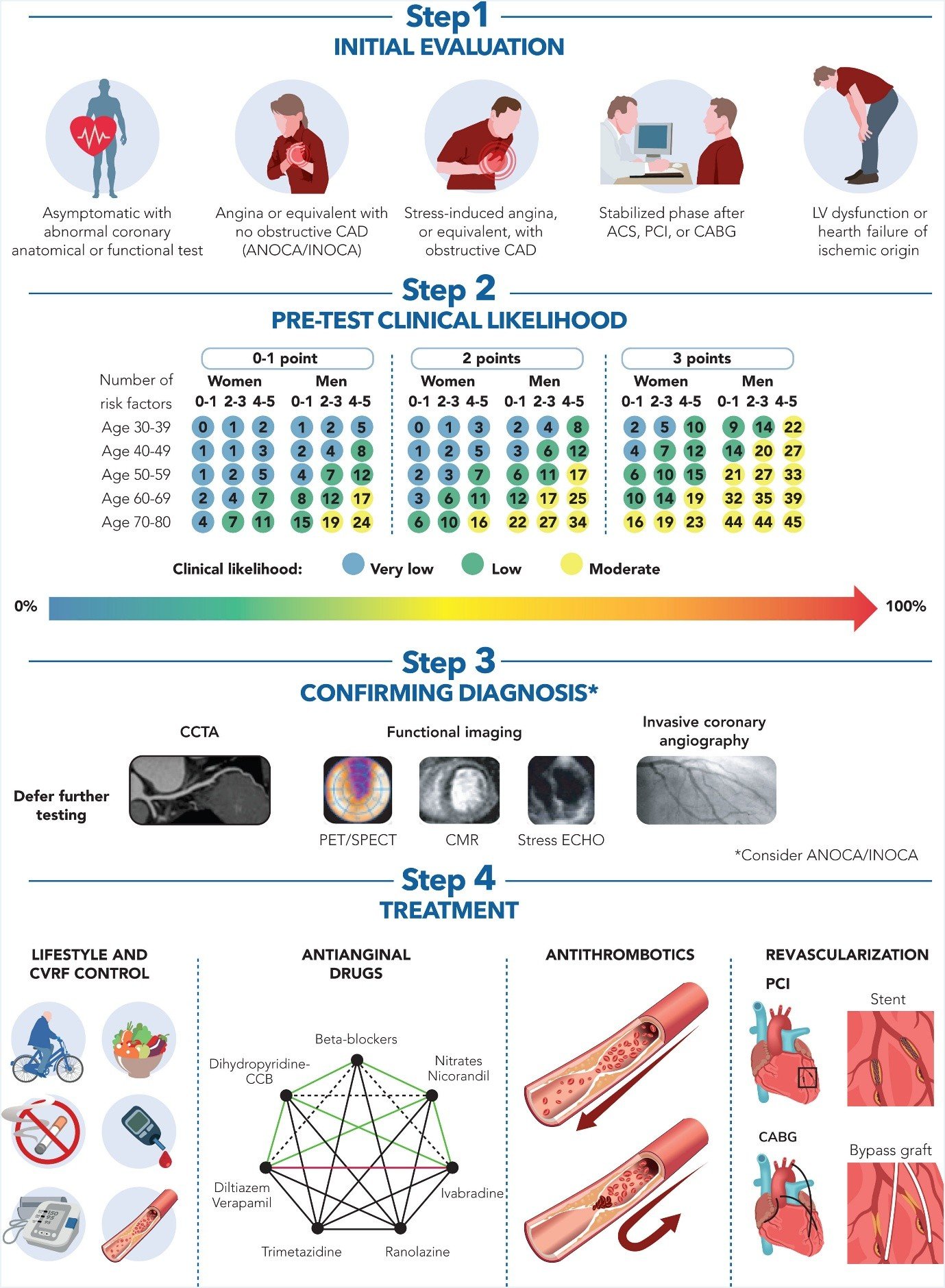
The management of chronic coronary syndromes in patients with heart failure requires attention to both heart failure therapies and antianginal strategies to control ischemic symptoms and prevent cardiovascular events. The 2024 ESC guidelines for chronic coronary syndromes recommend beta-blockers and calcium channel blockers as first-line therapy for angina, with the choice guided by the underlying pathophysiology, comorbidities, and hemodynamic profile. Beta-blockers reduce myocardial oxygen demand by lowering heart rate, blood pressure, and contractility, and are particularly appropriate for patients with HFrEF where they provide dual benefit. Calcium channel blockers, specifically dihydropyridines such as amlodipine, may be added for additional antianginal effect, though non-dihydropyridine calcium channel blockers including diltiazem and verapamil are contraindicated in HFrEF due to their negative inotropic effects.
Long-acting nitrates provide effective antianginal therapy by promoting coronary vasodilation and reducing preload, though tolerance develops with continuous use and a nitrate-free interval is recommended. Ranolazine, which inhibits the late sodium current, reduces angina without significant hemodynamic effects and can be safely used in patients with HFrEF. Ivabradine, which inhibits the funny current in the sinoatrial node, reduces heart rate without affecting blood pressure or contractility, and is indicated for patients in sinus rhythm with heart rate above seventy beats per minute despite maximally tolerated beta-blocker therapy. Trimetazidine, which shifts myocardial metabolism from fatty acids to glucose, improves exercise tolerance and reduces angina episodes, and has been shown to improve left ventricular ejection fraction and functional class in patients with HFrEF and coronary artery disease.
Antithrombotic therapy is essential for secondary prevention in patients with chronic coronary syndromes and heart failure. Aspirin at doses of seventy-five to one hundred milligrams daily is recommended for life in patients with prior myocardial infarction, prior percutaneous coronary intervention, prior coronary artery bypass grafting, or evidence of significant obstructive coronary artery disease regardless of revascularization history. Clopidogrel may be considered as an alternative for patients intolerant to aspirin. In patients with recent acute coronary syndrome or percutaneous coronary intervention, dual antiplatelet therapy with aspirin and a P2Y12 inhibitor is recommended for a duration determined by the bleeding and ischemic risk. The COMPASS trial demonstrated that low-dose rivaroxaban plus aspirin reduced major adverse cardiovascular events compared to aspirin alone in patients with stable coronary artery disease, though with increased bleeding risk. In patients requiring long-term oral anticoagulation for atrial fibrillation, the 2024 ESC guidelines recommend lifelong treatment with a direct oral anticoagulant or vitamin K antagonist, with proton pump inhibitors considered for gastrointestinal protection.
Lipid-lowering therapy with high-intensity statins is recommended for all patients with chronic coronary syndromes and heart failure, with a low-density lipoprotein cholesterol target of less than 1.4 mmol per liter and reduction of at least fifty percent from baseline. Ezetimibe should be added if statin therapy alone does not achieve targets, and proprotein convertase subtilisin-kexin type 9 inhibitors should be considered for very high-risk patients or those with familial hypercholesterolemia. The 2024 ESC guidelines emphasize that lipid-lowering therapy is a cornerstone of secondary prevention and should be initiated promptly and titrated to achieve targets.
3.6 Revascularization in Ischemic Cardiomyopathy
The role of revascularization in patients with chronic coronary syndromes and heart failure has been debated for decades, with the fundamental question being whether restoring blood flow to ischemic or hibernating myocardium improves outcomes beyond optimal medical therapy. The STICH trial randomized 1,012 patients with ischemic cardiomyopathy and left ventricular ejection fraction of thirty-five percent or less to coronary artery bypass grafting plus optimal medical therapy versus optimal medical therapy alone. At the initial follow-up of 4.7 years, no significant difference was observed in the primary endpoint of all-cause mortality, though the CABG group showed lower rates of cardiovascular death and the combined endpoint of death or cardiovascular hospitalization. However, at extended follow-up of 9.8 years, the STICHES analysis demonstrated a significant sixteen percent reduction in all-cause mortality with CABG, with subgroup analyses indicating that patients with three-vessel disease or severely remodeled left ventricles derived the greatest benefit.
The REVIVED-BCIS2 trial, which randomized 700 patients with left ventricular ejection fraction of thirty-five percent or less, extensive coronary disease, and evidence of viability to percutaneous coronary intervention plus optimal medical therapy versus optimal medical therapy alone, found no significant benefit of PCI on the primary endpoint of all-cause death or heart failure hospitalization at 41 months. Quality of life scores improved at six and twelve months in the PCI group but converged with the medical therapy group by twenty-four months. These findings suggest that in patients with stable ischemic cardiomyopathy without severe angina, PCI may not provide incremental benefit over comprehensive medical therapy, challenging the concept that viability alone justifies revascularization.
Contemporary guidelines reflect this nuanced evidence base. The 2024 ESC guidelines recommend coronary artery bypass grafting as first-line revascularization for patients with multivessel or left main disease, heart failure, and acceptable surgical risk, with PCI considered as an alternative in selected patients with one or two-vessel disease or those with anatomy suitable for complete revascularization. The AHA-ACC-HFSA guidelines provide a class one recommendation for surgical revascularization in selected patients with heart failure and ejection fraction of thirty-five percent or less whose coronary anatomy is suitable. NICE guidelines take a more conservative approach, recommending that revascularization not be routinely offered to people with HFrEF and coronary artery disease, reflecting uncertainty about the prognostic benefit. The decision to revascularize should be individualized, considering symptom burden, coronary anatomy, viability assessment, surgical risk, and patient preferences, with discussion in a multidisciplinary heart team.
3.7 Device Therapy and Advanced Interventions
Implantable cardioverter-defibrillators are indicated for primary prevention of sudden cardiac death in patients with HFrEF despite optimal medical therapy. The 2024 Chinese guidelines recommend ICD implantation in patients with ischemic cardiomyopathy, left ventricular ejection fraction of thirty-five percent or less, New York Heart Association class II to III symptoms, and expected survival of more than one year, provided they have been on optimal medical therapy for at least three months. ICD therapy is generally not recommended within forty days of myocardial infarction or ninety days of revascularization, as the risk of arrhythmic death is lower during these periods and the benefit of ICD therapy has not been demonstrated.
Cardiac resynchronization therapy is indicated for patients with HFrEF, left ventricular ejection fraction of thirty-five percent or less, left bundle branch block with QRS duration of at least 150 milliseconds, and New York Heart Association class II to IV symptoms despite optimal medical therapy. CRT improves symptoms, reduces heart failure hospitalization, and reduces mortality by coordinating ventricular contraction and reversing adverse remodeling. In patients with chronic coronary disease, CRT may be particularly beneficial when conduction abnormalities result from prior infarction or ischemic fibrosis. The 2024 guidelines emphasize that CRT should be considered early in the course of heart failure, as delayed implantation may limit the potential for reverse remodeling.
Cardiac contractility modulation represents an emerging therapy for patients with HFrEF who remain symptomatic despite optimal medical therapy and are not candidates for CRT. This device delivers non-excitatory electrical signals during the absolute refractory period, enhancing calcium handling and improving contractility without increasing myocardial oxygen demand. While not yet established as standard therapy, cardiac contractility modulation may provide symptomatic benefit in selected patients with chronic ischemic cardiomyopathy.
For patients with end-stage heart failure despite comprehensive medical and device therapy, mechanical circulatory support and heart transplantation remain options. Left ventricular assist devices are indicated as bridge to transplantation or destination therapy in patients with refractory heart failure, with modern continuous-flow devices achieving two-year survival rates exceeding eighty percent. Heart transplantation remains the definitive treatment for eligible patients, though organ availability limits its application. The 2024 Chinese guidelines provide detailed criteria for LVAD implantation, including left ventricular ejection fraction below twenty-five percent, peak oxygen consumption below twelve milliliters per kilogram per minute, and dependence on intravenous inotropes or short-term mechanical support.
3.8 Management of Acute Decompensation
Acute decompensated heart failure represents a frequent and serious complication in patients with chronic coronary syndromes, requiring prompt recognition and management to prevent progressive organ dysfunction and death. The clinical presentation ranges from gradual worsening of congestion to acute pulmonary edema and cardiogenic shock. Initial assessment should evaluate circulatory and respiratory stability, identify precipitating factors including acute coronary syndrome, arrhythmia, infection, and medication nonadherence, and determine the clinical profile using the wet-warm, wet-cold, dry-warm, and dry-cold classification.
Diuretics are the cornerstone of congestion management in acute decompensated heart failure. Loop diuretics, administered intravenously, promote rapid diuresis and relieve symptoms. The DOSE trial demonstrated no clinically significant difference between bolus and continuous infusion strategies, though continuous infusion may be preferred in patients with marginal renal function. For patients with diuretic resistance, combination therapy with thiazide diuretics or acetazolamide may enhance diuretic efficacy, though monitoring for electrolyte disturbances and renal dysfunction is essential. The ADVOR trial demonstrated that adding acetazolamide to loop diuretics increased successful decongestion within three days compared to placebo.
Vasodilators including nitrates and sodium nitroprusside reduce preload and afterload, improving pulmonary congestion and cardiac output. They are particularly useful in patients with hypertensive emergency and pulmonary edema. Inotropic agents including dobutamine and milrinone are indicated in patients with low output states and evidence of organ hypoperfusion, though they increase myocardial oxygen demand and arrhythmia risk and should be used cautiously. Levosimendan, a calcium sensitizer with vasodilatory properties, improves contractility without increasing oxygen demand and may be particularly beneficial in patients with acute on chronic heart failure.
For patients with acute decompensation superimposed on chronic HFrEF, continuation or initiation of guideline-directed medical therapy is crucial unless hemodynamic instability, severe renal dysfunction, or hyperkalemia precludes its use. The 2024 Chinese guidelines emphasize that continuation of treatment during hospitalization, as opposed to discontinuation, reduces the risk of death and rehospitalization post-discharge. For newly diagnosed patients, initiating guideline-directed therapy after hemodynamic stabilization is essential to improve long-term prognosis.
3.9 Comorbidity Management
The management of comorbidities is integral to the care of patients with chronic coronary syndromes and heart failure, as these conditions frequently coexist and influence both symptoms and outcomes. Diabetes mellitus is present in a substantial proportion of patients and contributes to both coronary disease progression and heart failure pathophysiology. Sodium-glucose cotransporter-2 inhibitors provide dual benefit by improving glycemic control and reducing heart failure events, making them particularly valuable in diabetic patients. Glucagon-like peptide-1 receptor agonists and dual glucose-dependent insulinotropic polypeptide receptor agonists provide additional cardiovascular benefit and weight reduction, and should be considered for patients with type 2 diabetes and obesity.
Obesity is increasingly recognized as a major risk factor for heart failure, particularly HFpEF, and presents unique management challenges. Weight reduction through lifestyle modification, pharmacological therapy with GLP-1 receptor agonists or dual agonists, and bariatric surgery in selected patients can improve cardiac function, symptoms, and quality of life. The 2024 guidelines emphasize that purposeful weight loss may be reasonable in obese patients with heart failure for improving health-related quality of life and managing comorbidities, though weight loss has not been proven to reduce heart failure mortality.
Iron deficiency, defined as ferritin below 100 nanograms per milliliter or ferritin 100 to 300 nanograms per milliliter with transferrin saturation below twenty percent, is present in more than fifty percent of patients with stable chronic heart failure and is associated with reduced quality of life and worse prognosis. Intravenous ferric carboxymaltose has been shown to improve functional status and quality of life in iron-deficient patients with HFrEF, with the 2024 Chinese guidelines and international guidelines providing class two recommendations for its use. The HEART-FID trial, while not meeting its primary endpoint, contributed to the totality of evidence supporting intravenous iron supplementation in heart failure.
Atrial fibrillation is common in patients with chronic coronary syndromes and heart failure and contributes to symptom burden, thromboembolic risk, and adverse remodeling. Rate control with beta-blockers or non-dihydropyridine calcium channel blockers is preferred in HFpEF, while rhythm control strategies including catheter ablation have demonstrated benefit in selected patients with HFrEF and atrial fibrillation. Anticoagulation is indicated based on stroke risk assessment, with direct oral anticoagulants preferred over vitamin K antagonists in most patients.
4. Discussion
The integration of chronic coronary syndrome management with heart failure care represents one of the most challenging yet rewarding domains in cardiovascular medicine. The evidence synthesized in this review establishes a clear framework for diagnosis and treatment, while also highlighting persistent gaps between evidence and practice that demand attention.
Several overarching themes emerge from this synthesis. First, the establishment of quadruple guideline-directed medical therapy as the standard of care for HFrEF represents a transformative advance that has fundamentally altered the prognosis of ischemic cardiomyopathy. The remarkable efficacy of this approach, with approximately seventy-three percent mortality reduction when fully implemented, stands as one of the great achievements of modern cardiovascular therapeutics. Yet the suboptimal real-world implementation, with only fifteen percent of eligible patients receiving all four pillars, represents a critical failure of the healthcare system that demands urgent attention. Strategies to improve implementation, including clinical decision support tools, standardized order sets, pharmacist-led medication optimization, and patient education, must be prioritized.
Second, the expansion of evidence-based therapy to HFpEF and HFmrEF through SGLT2 inhibitors finally addresses a longstanding therapeutic void. For decades, patients with preserved ejection fraction had no proven pharmacological options, despite representing the majority of heart failure cases. The consistent benefit of dapagliflozin and empagliflozin across ejection fraction phenotypes, combined with their favorable safety profile and ease of administration, establishes them as foundational therapy for all heart failure patients. The rapid onset of benefit, within fourteen to twenty-eight days, supports inpatient initiation and early optimization.
Third, the role of revascularization in ischemic cardiomyopathy remains nuanced and individualized. The STICH trial established long-term survival benefit with CABG in selected patients, while REVIVED-BCIS2 challenged the viability hypothesis for PCI. Contemporary guidelines appropriately reflect this evidence, with CABG preferred for multivessel disease and acceptable surgical risk, while PCI is reserved for selected anatomical scenarios or patients unsuitable for surgery. The heart team approach, integrating cardiology, cardiac surgery, and imaging expertise, is essential for optimal revascularization decisions.
Fourth, the management of comorbidities including diabetes, obesity, iron deficiency, and atrial fibrillation is not ancillary but integral to heart failure care in patients with chronic coronary disease. These conditions frequently drive symptoms, limit therapeutic options, and influence prognosis. The recognition of heart failure as part of the broader cardio-kidney-metabolic syndrome encourages a holistic approach that addresses all contributors to cardiovascular risk.
Methodological limitations in the existing evidence warrant acknowledgment. Many landmark trials excluded patients with significant comorbidities or recent revascularization, limiting generalizability to the broad population with chronic coronary syndromes and heart failure. The underrepresentation of elderly patients, women, and racial minorities in clinical trials may not capture the full spectrum of treatment response. Real-world evidence and pragmatic trials are needed to complement the efficacy data from highly selected randomized controlled trials.
5. Conclusion
The diagnosis and treatment of heart failure in patients with chronic coronary syndromes has evolved dramatically, with contemporary guidelines providing a robust, evidence-based framework that integrates diagnostic precision with comprehensive therapeutic strategies. The establishment of quadruple guideline-directed medical therapy as the cornerstone for HFrEF, the expansion of SGLT2 inhibitors across all ejection fraction phenotypes, and the nuanced approach to revascularization represent major advances that have transformed patient outcomes. Yet the full realization of these benefits requires overcoming implementation barriers and ensuring equitable access to guideline-concordant care. Looking forward, the integration of novel therapies including finerenone, emerging device technologies, and personalized approaches based on phenotypic profiling promise to further improve outcomes for this challenging patient population. The clinician managing heart failure in chronic coronary syndromes must maintain expertise across a broad therapeutic landscape while remaining grounded in the fundamental principles of evidence-based medicine and patient-centered care.
References
Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415-3538. doi:10.1093/eurheartj/ehae177
Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895-e1032. doi:10.1161/CIR.0000000000001063
Chinese Society of Cardiology of Chinese Medical Association, Heart Failure Group of Chinese Society of Cardiology of Chinese Medical Association, Editorial Board of Chinese Journal of Cardiology. Chinese guidelines for the diagnosis and treatment of heart failure 2024. Chin J Cardiol. 2024;52(4):235-275. doi:10.3760/cma.j.cn112148-20240126-00045
McDonagh TA, Metra M, Adamo M, et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023;44(37):3627-3639. doi:10.1093/eurheartj/ehad195
Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129-2200. doi:10.1093/eurheartj/ehw128
Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure. J Am Coll Cardiol. 2017;70(6):776-803. doi:10.1016/j.jacc.2017.04.025
McMurray JJV, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004. doi:10.1056/NEJMoa1409077
Solomon SD, McMurray JJV, Claggett B, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387(12):1089-1098. doi:10.1056/NEJMoa2206286
Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451-1461. doi:10.1056/NEJMoa2107038
McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008. doi:10.1056/NEJMoa1911303
Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413-1424. doi:10.1056/NEJMoa2022190
Velazquez EJ, Lee KL, Deja MA, et al. Coronary-artery bypass surgery in patients with left ventricular dysfunction. N Engl J Med. 2011;364(17):1607-1616. doi:10.1056/NEJMoa1100356
Velazquez EJ, Lee KL, Jones RH, et al. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med. 2016;374(16):1511-1520. doi:10.1056/NEJMoa1602001
Perera D, Clayton T, O'Kane PD, et al. Percutaneous revascularization for ischemic left ventricular dysfunction. N Engl J Med. 2022;387(15):1351-1360. doi:10.1056/NEJMoa2206606
Cleland JGF, Bunting KV, Flather MD, et al. Beta-blockers for heart failure with reduced, mid-range, and preserved ejection fraction: an individual patient-level analysis of double-blind randomized trials. Eur Heart J. 2018;39(1):26-35. doi:10.1093/eurheartj/ehx564
Pitt B, Pfeffer MA, Assmann SF, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370(15):1383-1392. doi:10.1056/NEJMoa1313731
Zannad F, Ferreira JP, Pocock SJ, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet. 2020;396(10254):819-829. doi:10.1016/S0140-6736(20)31824-9
Solomon SD, McMurray JJV, Anand IS, et al. Angiotensin-neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med. 2019;381(17):1609-1620. doi:10.1056/NEJMoa1908655
Packer M, Coats AJS, Fowler MB, et al. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med. 2001;344(22):1651-1658. doi:10.1056/NEJM200105313442201
CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353(9146):9-13. doi:10.1016/S0140-6736(98)11181-9
Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353(9169):2001-2007. doi:10.1016/S0140-6736(99)04440-2
Zannad F, McMurray JJV, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21. doi:10.1056/NEJMoa1009492
Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14):1309-1321. doi:10.1056/NEJMoa030207
Solomon SD, Vaduganathan M, Claggett BL, et al. Sacubitril/valsartan across the spectrum of ejection fraction in heart failure. Circulation. 2020;141(5):352-361. doi:10.1161/CIRCULATIONAHA.119.044586
O'Meara E, McDonald M, Chan M, et al. CCS/CHFS Heart Failure Guidelines Update: Defining a New Pharmacologic Standard of Care for Heart Failure With Reduced Ejection Fraction. Can J Cardiol. 2021;37(4):531-546. doi:10.1016/j.cjca.2021.01.017
Tromp J, Ouwerkerk W, van Veldhuisen DJ, et al. A systematic review and network meta-analysis of pharmacological treatment of heart failure with reduced ejection fraction. JACC Heart Fail. 2022;10(2):73-84. doi:10.1016/j.jchf.2021.09.073