
Challenges of Drug Dosing in Pediatrics
1. Abdieva Begimai Zhumalievna
2. Manir Ansari
3. Alamin Molla
(1. Lecturer, International Medical Faculty, Osh State University, Kyrgyzstan)
(2. Student, International Medical Faculty, Osh State University, Kyrgyzstan)
(3. Student, International Medical Faculty, Osh State University, Kyrgyzstan)
Abstract
Giving medicines to children is far more complicated than simply reducing an adult dose according to body weight. Children experience rapid physical and physiological changes from birth through adolescence, and these developmental differences strongly influence how medicines are absorbed, distributed, metabolized, and eliminated from the body. Because of these changes, pediatric drug dosing remains one of the most difficult areas in clinical medicine. Inappropriate dosing can result in treatment failure, toxicity, adverse drug reactions, or long-term complications. Additional challenges include limited pediatric clinical trials, ethical concerns in research, lack of child-friendly formulations, and wide variation in drug response among children of different ages. This review discusses the major challenges associated with pediatric drug dosing, including developmental pharmacokinetics, pharmacodynamics, off-label prescribing, medication errors, neonatal and critical care dosing, pharmacogenetics, and formulation difficulties. Modern strategies such as therapeutic drug monitoring, population pharmacokinetic modeling, physiologically based pharmacokinetic (PBPK) modeling, and precision medicine are also explored. Improving pediatric drug research and individualized dosing strategies is essential to ensure safe and effective therapy for children.
Keywords: Pediatrics, drug dosing, pharmacokinetics, pharmacodynamics, pediatric pharmacology, precision medicine, therapeutic drug monitoring.
Introduction
The use of medicines in children has always been a major challenge in healthcare. Unlike adults, children are continuously growing and developing, meaning that their bodies handle medicines differently at different ages[1,2]. A premature newborn, a toddler, a school-aged child, and a teenager all respond differently to medications because their organs and body systems mature over time. For this reason, children cannot simply be treated as “small adults” when calculating drug doses.
For many years, pediatric doses were estimated by reducing adult doses according to body weight or body surface area. Although this method is still widely used, it does not fully account for the complex physiological changes that occur during childhood [2,3]. Factors such as immature liver enzymes, reduced kidney function, changes in body water and fat composition, and developing receptor systems all influence how drugs behave in children. As a result, using simplified dosing calculations may sometimes lead to harmful consequences.
Drug dosing becomes even more difficult because many medicines used in children have not been adequately studied in pediatric populations [4]. A large number of drugs prescribed to children are used “off-label,” meaning that they are prescribed outside their officially approved age group or dosing recommendations. This occurs because conducting clinical trials in children presents ethical and practical difficulties. Physicians are therefore often forced to rely on limited evidence or extrapolated adult data [5,6].
Medication safety is another important issue in pediatrics. Drug doses in children are usually calculated individually according to body weight, which increases the risk of mathematical and prescribing errors. Even small mistakes in decimal points or unit conversions can lead to serious overdose or underdose situations [6,7].
In recent decades, advances in pediatric clinical pharmacology have improved our understanding of developmental drug handling [8,9]. Modern approaches such as therapeutic drug monitoring, pharmacogenetic testing, population pharmacokinetic analysis, and physiologically based pharmacokinetic modeling are helping clinicians move toward more individualized and safer therapy for children [10].
Methodology
This review article was prepared using a narrative literature review approach. Relevant scientific articles were collected from PubMed, Google Scholar, and other peer-reviewed medical databases. Search terms included “pediatric drug dosing,” “developmental pharmacology,” “pharmacokinetics in children,” “off-label drug use,” “precision medicine in pediatrics,” and “therapeutic drug monitoring.”
Priority was given to original research articles, systematic reviews, and clinical pharmacology studies published between 2000 and 2026. Studies related to neonatal pharmacology, pediatric intensive care, drug metabolism, and individualized therapy were carefully reviewed. Information from the selected studies was organized into major themes related to challenges in pediatric drug dosing.
Developmental Pharmacokinetics in Children
Pharmacokinetics describes how the body handles a drug through absorption, distribution, metabolism, and excretion. In children, each of these processes changes significantly with growth and development.
Drug Absorption
Drug absorption differs greatly between children and adults. In newborns and infants, the stomach produces less acid, leading to a higher gastric pH. This can increase or decrease the absorption of certain medications depending on their chemical properties.
Gastric emptying and intestinal movement are also slower in neonates. As a result, orally administered drugs may take longer to reach therapeutic levels. Furthermore, blood flow to muscles is less predictable in infants, making intramuscular drug absorption unreliable.
Skin absorption is another important issue. Infants have thinner skin and greater skin hydration, which allows topical medications to be absorbed more easily. This increases the risk of toxicity from creams, ointments, and antiseptics.
Drug Distribution
Drug distribution refers to how medications spread throughout body tissues and fluids. Children have major differences in body composition compared with adults.
Newborns have a much higher percentage of body water and lower body fat. Water-soluble drugs therefore distribute more widely in neonates, often requiring relatively larger doses per kilogram. On the other hand, fat-soluble drugs may have reduced distribution.
Protein binding is also lower in newborns because plasma protein levels are reduced. This increases the amount of free, active drug circulating in the bloodstream, potentially increasing toxicity risk.
Drug Metabolism
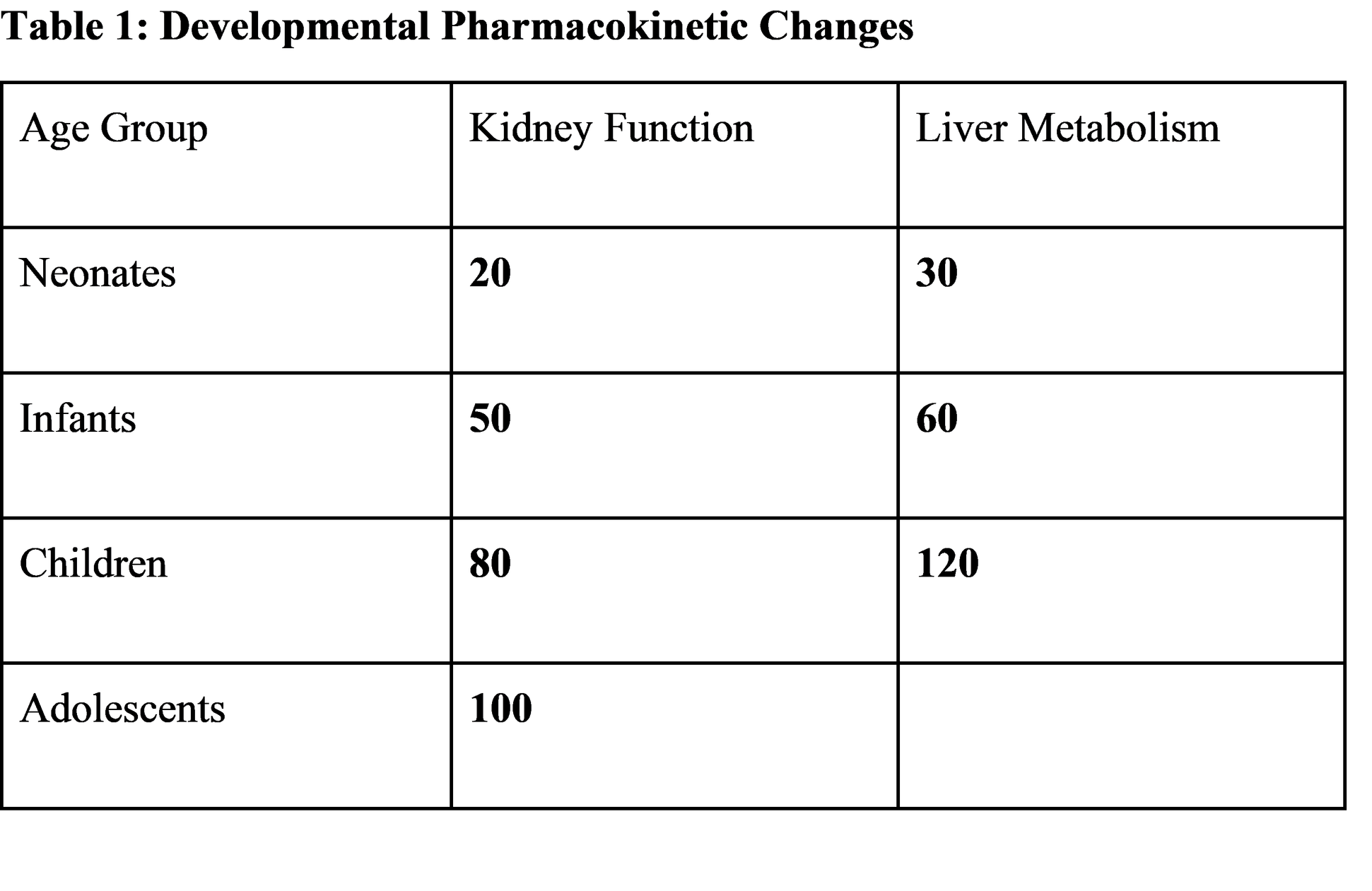
The liver plays a central role in drug metabolism, and hepatic enzyme systems develop gradually after birth.
In neonates, many metabolic enzymes are immature, causing drugs to remain in the body longer. This is why newborns are especially vulnerable to drug toxicity. A classic example is chloramphenicol-induced “gray baby syndrome,” which occurred because newborns could not metabolize the drug effectively.
Interestingly, some metabolic pathways become more active during childhood than in adulthood. As a result, older infants and children may metabolize certain drugs faster than adults, requiring relatively higher doses per kilogram.
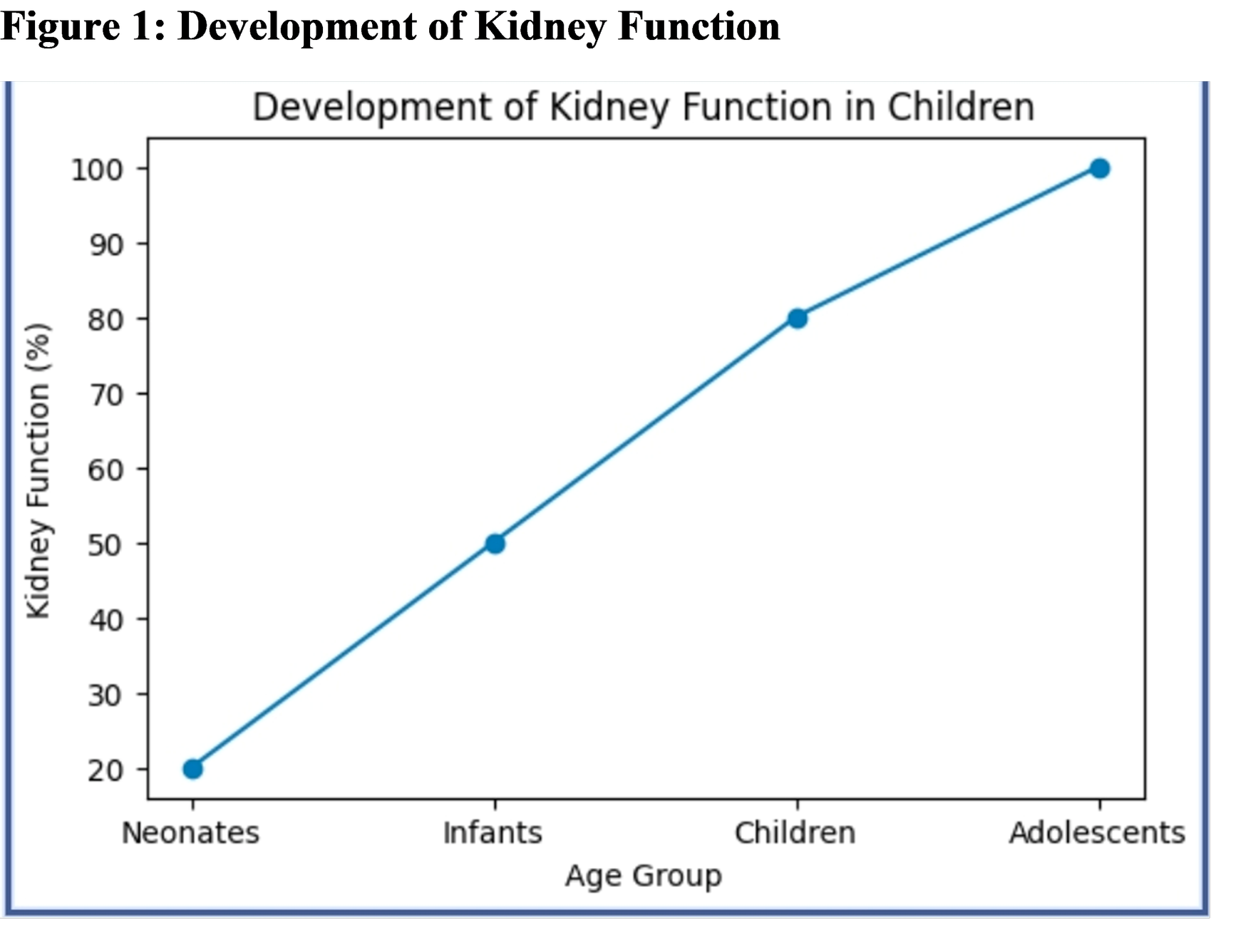
Drug Excretion
Kidney function is immature at birth, especially in premature infants. Glomerular filtration and tubular secretion improve gradually during infancy.
Because many drugs are eliminated through the kidneys, reduced renal function can lead to dangerous drug accumulation. Antibiotics such as gentamicin and vancomycin require careful monitoring in neonates and young infants to avoid toxicity.
Pharmacodynamic Differences
Pharmacodynamics refers to the effects drugs produce on the body. Children may respond differently to medications because receptor systems and organ sensitivity change with age.
For example, neonates are more sensitive to sedatives and opioids because of immature nervous system regulation. Some antihistamines may produce excitement instead of sedation in children. Corticosteroids may interfere with growth and bone development when used for prolonged periods.
Off-Label Drug Use in Pediatrics
One of the biggest challenges in pediatric medicine is the widespread use of off-label medications.
Why Off-Label Use Happens
Many pharmaceutical companies do not perform large pediatric clinical trials because they are expensive, time-consuming, and ethically complex. As a result, medications approved for adults are often prescribed to children without complete pediatric dosing information.
Risks Associated with Off-Label Use
Off-label prescribing increases uncertainty regarding safe dosing, effectiveness, adverse effects, and long-term outcomes. Children receiving off-label medications may have a higher risk of medication-related complications.
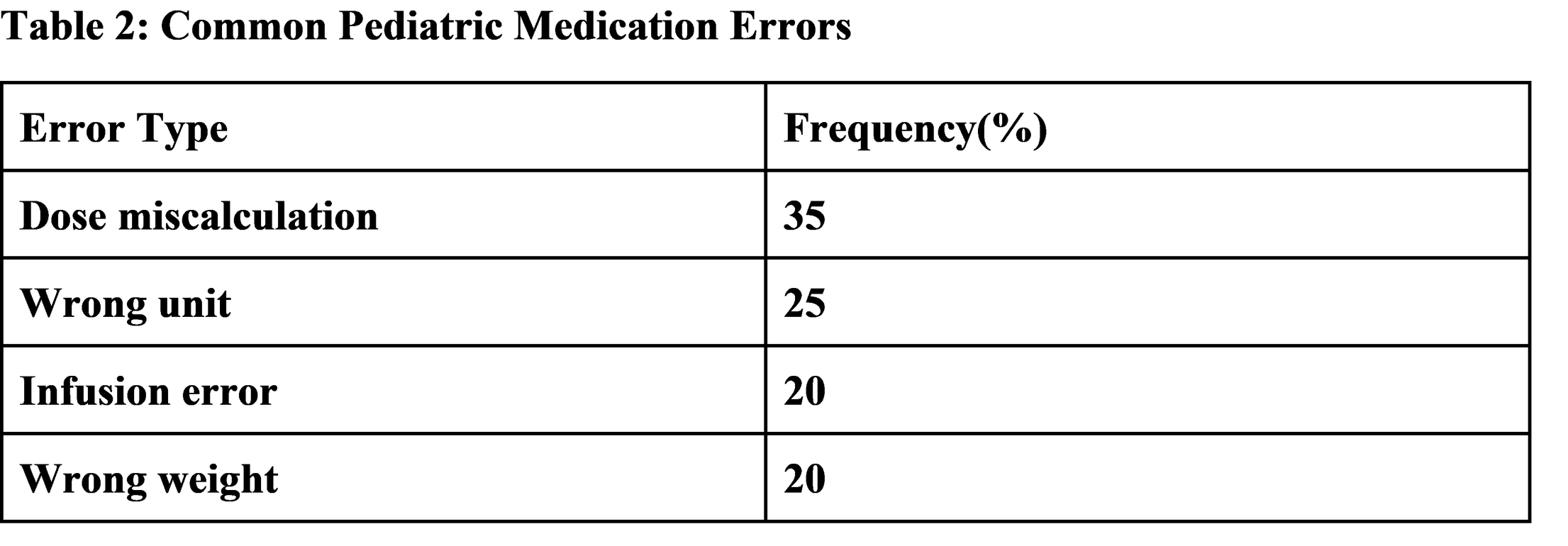
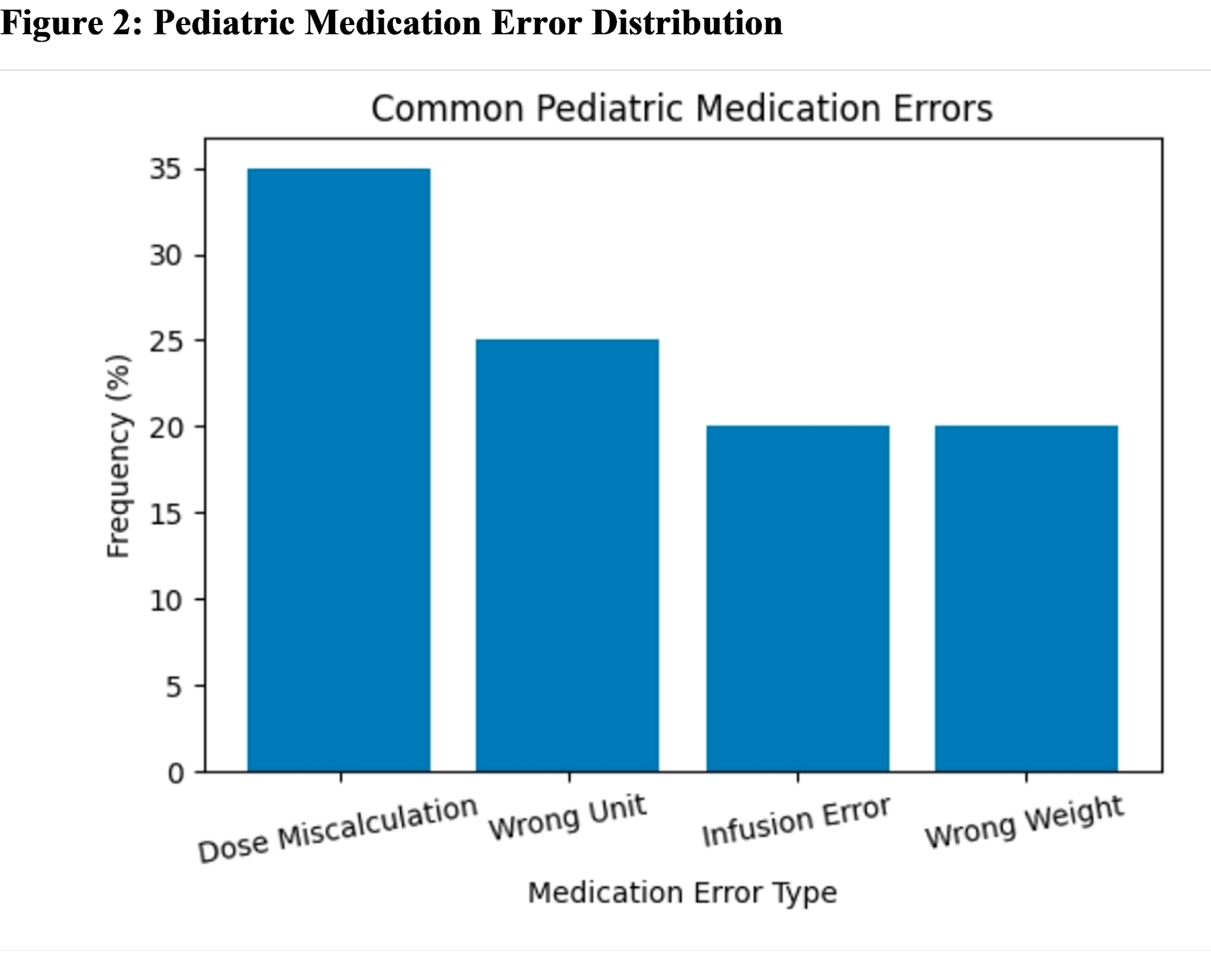
Medication Errors in Children
Medication errors are especially dangerous in pediatrics because doses are individualized according to weight.
Common Causes of Errors
- Incorrect weight measurement.
- Wrong dose calculations.
- Decimal point mistakes.
- Confusion between milligrams and milliliters.
- Incorrect infusion rates.
Prevention Strategies
Several strategies can help reduce medication errors:
- Electronic prescribing systems
- Standardized dosing charts
- Clinical pharmacist involvement
- Double-checking calculations
- Weight-based computerized calculators
Challenges with Pediatric Drug Formulations
Many medicines are designed primarily for adults, creating difficulties for children.
Difficulty Swallowing Tablets
Young children often cannot swallow tablets or capsules. Liquid formulations are preferred, but they are not always available.
Taste and Adherence
Children are highly sensitive to unpleasant tastes. Bitter medications may lead to poor adherence and incomplete treatment.
Manipulation of Adult Dosage Forms
Healthcare providers sometimes crush adult tablets or divide capsules to obtain pediatric doses. However, this may affect drug stability and dosing accuracy.
Neonatal Drug Dosing
Neonates are among the most challenging patients for drug dosing because their organs are still immature.
Premature infants have reduced liver enzyme activity, lower kidney clearance, decreased protein binding, and altered body composition. These factors create large differences in drug response even among infants of similar age.
Drugs commonly requiring close monitoring in neonates include aminoglycosides, vancomycin, morphine, and caffeine.
Drug Dosing in Critically Ill Children
Critical illness significantly alters drug handling in the body.
Factors such as inflammation, fluid overload, organ dysfunction, and reduced blood flow can dramatically change pharmacokinetics in pediatric intensive care patients.
Therapeutic drug monitoring is increasingly used in critically ill children to guide individualized dosing.
Pharmacogenetics and Precision Medicine
Pharmacogenetics studies how genetic differences influence drug response.
Some children metabolize drugs differently because of inherited enzyme variations. For example, certain CYP2D6 gene variants can cause dangerous morphine toxicity when codeine is administered.
Precision medicine aims to tailor therapy according to age, weight, organ function, genetic profile, and disease severity.
Population Pharmacokinetics and PBPK Modeling
Modern pharmacometric techniques are improving pediatric dose optimization.
Population pharmacokinetic analysis evaluates drug behavior across groups of patients while requiring only small blood samples.
PBPK models simulate drug behavior using mathematical representations of organ systems and developmental physiology.
Therapeutic Drug Monitoring
Therapeutic drug monitoring involves measuring drug concentrations in blood to optimize therapy.
This approach is especially useful for drugs with narrow therapeutic ranges, including vancomycin, aminoglycosides, antiepileptics, and immunosuppressants.
Ethical Challenges in Pediatric Research
Conducting clinical research in children raises important ethical concerns.
Children cannot legally provide informed consent, requiring parental permission and age-appropriate assent. Researchers must minimize pain, discomfort, and invasive procedures.
Future Directions
The future of pediatric drug dosing is moving toward personalized medicine.
Emerging developments include artificial intelligence-assisted dosing, genomic medicine, biomarker-guided therapy, improved pediatric formulations, and real-time therapeutic monitoring.
Conclusion
Drug dosing in pediatrics is a highly complex process influenced by growth, development, organ maturation, and genetic variability. Children cannot be treated as miniature adults because their bodies process and respond to medications differently at each stage of development.
Continued investment in pediatric research, child-friendly formulations, and evidence-based dosing guidelines is essential to improve medication safety and therapeutic outcomes in children worldwide.
References
Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL, Leeder JS, Kauffman RE. Developmental pharmacology--drug disposition, action, and therapy in infants and children. N Engl J Med. 2003 Sep 18;349(12):1157-67. doi: 10.1056/NEJMra035092. PMID: 13679531.
Barker CIS, Standing JF, Kelly LE, Hanly Faught L, Needham AC, Rieder MJ, de Wildt SN, Offringa M. Pharmacokinetic studies in children: recommendations for practice and research. Arch Dis Child. 2018 Jul;103(7):695-702. doi: 10.1136/archdischild-2017-314506. Epub 2018 Apr 19. PMID: 29674514; PMCID: PMC6047150.
Rose K. The Challenges of Pediatric Drug Development. Curr Ther Res Clin Exp. 2019 Jan 26;90:128-134. doi: 10.1016/j.curtheres.2019.01.007. PMID: 31388368; PMCID: PMC6677568.
Zajicek A. Creativity in Pediatric Clinical Pharmacology: Study Design and Oral Dosage Forms. J Pediatr Pharmacol Ther. 2024 Dec;29(6):564-569. doi: 10.5863/1551-6776-29.6.564. Epub 2024 Dec 9. PMID: 39659863; PMCID: PMC11627571.
Johnson TN, Small BG, Berglund EG, Rowland Yeo K. A best practice framework for applying physiologically-based pharmacokinetic modeling to pediatric drug development. CPT Pharmacometrics Syst Pharmacol. 2021 Sep;10(9):967-972. doi: 10.1002/psp4.12678. Epub 2021 Jul 20. PMID: 34288581; PMCID: PMC8452294.
Li SC, Ye Q, Xu H, Zhang L, Wang Y. Population Pharmacokinetics and Dosing Optimization of Linezolid in Pediatric Patients. Antimicrob Agents Chemother. 2019 Mar 27;63(4):e02387-18. doi: 10.1128/AAC.02387-18. PMID: 30642929; PMCID: PMC6437496.
Anliker-Ort M, Rodieux F, Ziesenitz VC, Atkinson A, Bielicki JA, Erb TO, Gürtler N, Holland-Cunz S, Duthaler U, Rudin D, Haschke M, van den Anker J, Pfister M, Gotta V. Pharmacokinetics-Based Pediatric Dose Evaluation and Optimization Using Saliva - A Case Study. J Clin Pharmacol. 2024 Jul;64(7):810-819. doi: 10.1002/jcph.2428. Epub 2024 Mar 18. PMID: 38497339.
Läer S, Elshoff JP, Meibohm B, Weil J, Mir TS, Zhang W, Hulpke-Wette M. Development of a safe and effective pediatric dosing regimen for sotalol based on population pharmacokinetics and pharmacodynamics in children with supraventricular tachycardia. J Am Coll Cardiol. 2005 Oct 4;46(7):1322-30. doi: 10.1016/j.jacc.2005.06.061. PMID: 16198851.
Standing JF, Tuleu C. Paediatric formulations--getting to the heart of the problem. Int J Pharm. 2005 Aug 26;300(1-2):56-66. doi: 10.1016/j.ijpharm.2005.05.006. PMID:15979830.
Watanabe H, Nagano N, Tsuji Y, Noto N, Ayusawa M, Morioka I. Challenges of pediatric pharmacotherapy: A narrative review of pharmacokinetics, pharmacodynamics, and pharmacogenetics. Eur J Clin Pharmacol. 2024 Feb;80(2):203-221. doi: 10.1007/s00228-023-03598-x. Epub 2023 Dec 11. PMID: 38078929.