
TB Treatment (Literature Review)
1. Kurmanaliev Nurlanbek Kambaralyevich
https://orcid.org/0000-0002-5952-1463
2. Ali Asraf
Shaik Manusha
Sheshma Kanchan
Eashwarnath N
(1. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
ABSTRACT
Treatment for tuberculosis is still difficult since individual and societal health must be taken into account. Furthermore, it has been demonstrated that social and economic factors must be taken into account when evaluating the efficacy of treatment. In order to provide health care professionals with recommendations based on the circumstances in Brazil and to better inform decision-making regarding tuberculosis patients in order to reduce morbidity and stop disease transmission, we critically reviewed the national and international literature on the treatment of tuberculosis in recent years.
Keywords: Tuberculosis/drug therapy; Tuberculosis/prevention & control; Tuberculosis/surgery; Tuberculosis/classification
INTRODUCTION
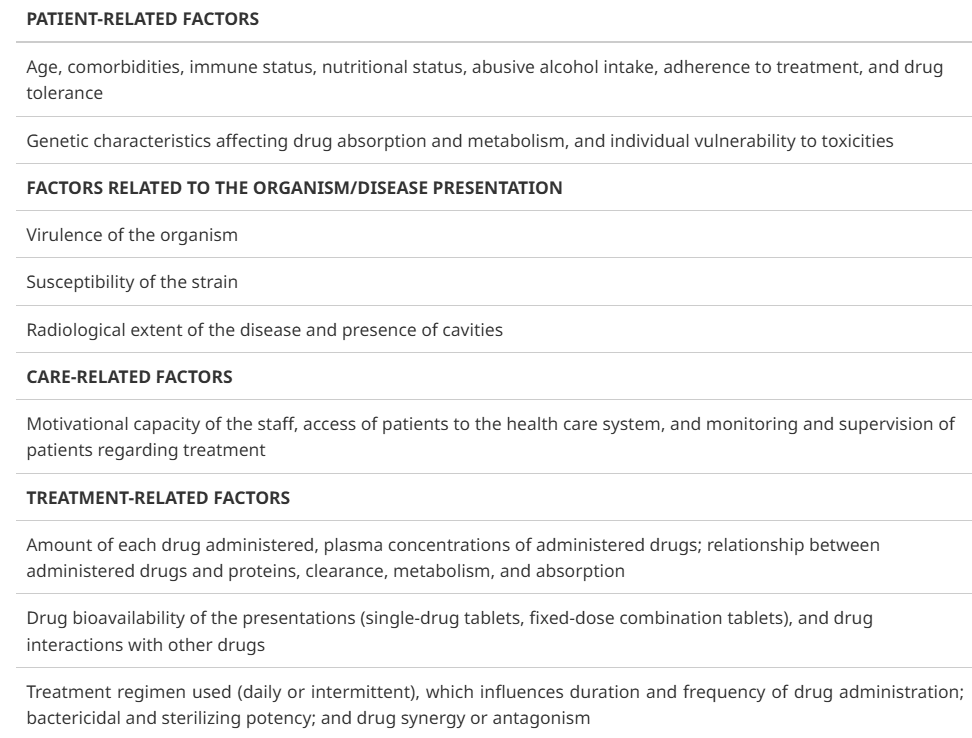
The goal of tuberculosis treatment is to cure the illness and quickly stop its spread. In order for this to happen, the medications must be able to sterilise the lesion (preventing disease return), stop the selection of naturally resistant strains (preventing the establishment of drug resistance during therapy), and quickly reduce the bacillary population (interrupting transmission). Treatment success (patients who are cured at the end of treatment under normal conditions) varies substantially by area, with the national average being about 70% (50-90%), despite the fact that antituberculosis regimens have an efficacy of up to 95%. Nonadherence, which can happen at three levels, is one of the reasons for low efficacy.
· Treatment default (patients stop using all medications) or
· Incorrect medication use (patients use some of the prescribed medications) and/or
· Irregular medication use (patients take the medications some days of the week but not every day of the week)
Medication failure, the selection of resistant organisms, and illness recurrence are all caused by issues with medication adherence. Since the early 1990s, the World Health Organization (WHO) has advocated for the implementation of the directly observed treatment, short course (DOTS) method in order to promote adherence to tuberculosis treatment and reorganise healthcare facilities. There are five components to the DOTS approach:
1. Political commitment and financial support to maintain tuberculosis control activities
2. Identification of tuberculosis cases on the basis of sputum smear microscopy among patients with respiratory symptoms
3. A standardized antituberculosis drug regimen administered as directly observed treatment (DOT) for at least the first 2 months of treatment
4. Guarantee of a regular supply of antituberculosis drugs
5. A system for reporting and assessment of treatment results for each patient and for the tuberculosis control program as a whole
Systematic reviews have not shown that DOT is more successful than self-administered treatment, despite the fact that monitored medication-taking through DOT promotes treatment adherence and permits frequent communication between patients and the health care system. This is likely due to the fact that medication-taking, a characteristic associated with patient care, is not the sole factor that affects treatment success.
However, because DOT seems to be strongly linked to sputum smear conversion (from positive to negative) during treatment, it continues to be the standard procedure of the majority of tuberculosis control programs in the USA and Europe. DOT is therefore advised for all kinds of tuberculosis in both the USA and Europe. DOT was introduced in Brazil in 1998 by the Program Nacional de Controle da Tuberculosis (PNCT, Brazilian National Tuberculosis Control Program). Since 2000, decentralisation measures have been implemented, such as integrating tuberculosis control into primary health care and proposing to provide DOT for at least 80% of patients with active tuberculosis in priority cities, but this has not happened.
However, there are circumstances where self-administered treatment is not feasible, in which case DOT should be the focus of all efforts. Patients with drug-resistant tuberculosis or those who are at a high risk of developing drug resistance include those who are homeless, drink, use illegal drugs, have mental, emotional, or physical disabilities that prevent them from taking their medications on their own, are children or adolescents, are deprived of their freedom, or have a history of treatment nonadherence.
TUBERCULOSIS TREATMENT
TUBERCULOSIS TREATMENT IN ADULTS
When the Brazilian National Campaign against Tuberculosis began in the 1940s, two antituberculosis medications were used: para-amino salicylic acid and streptomycin. Brazil decided to administer isoniazid and streptomycin twice a week in the 1950s. Treatment plans started to become standardised in the 1960s due to bacterial resistance and the rise in tuberculosis mortality. The HSZ regimen, which consists of isoniazid (H), streptomycin (S), and pyrazinamide (Z) for 18 months, was adopted. The RHZ regimen, which consists of rifampin (R), isoniazid (H), and pyrazinamide (Z) for six months, was developed as a short-term antituberculosis treatment in the mid-1970s. Brazil was the first nation in the world to introduce the 6-month regimen into the public health care system; all medications were given out for free and taken orally. Combination RH capsules were first used in the 1980s with the goal of preventing acquired bacterial resistance. Based on the preliminary results of the Second National Survey on Antituberculosis Drug Resistance, which revealed an increase in primary resistance to isoniazid (from 4.4% to 6.0%), Brazil implemented fixed-dose combination (FDC) tablets and added ethambutol (E) to the RHZ regimen, as defined by the PNCT, in 2009.
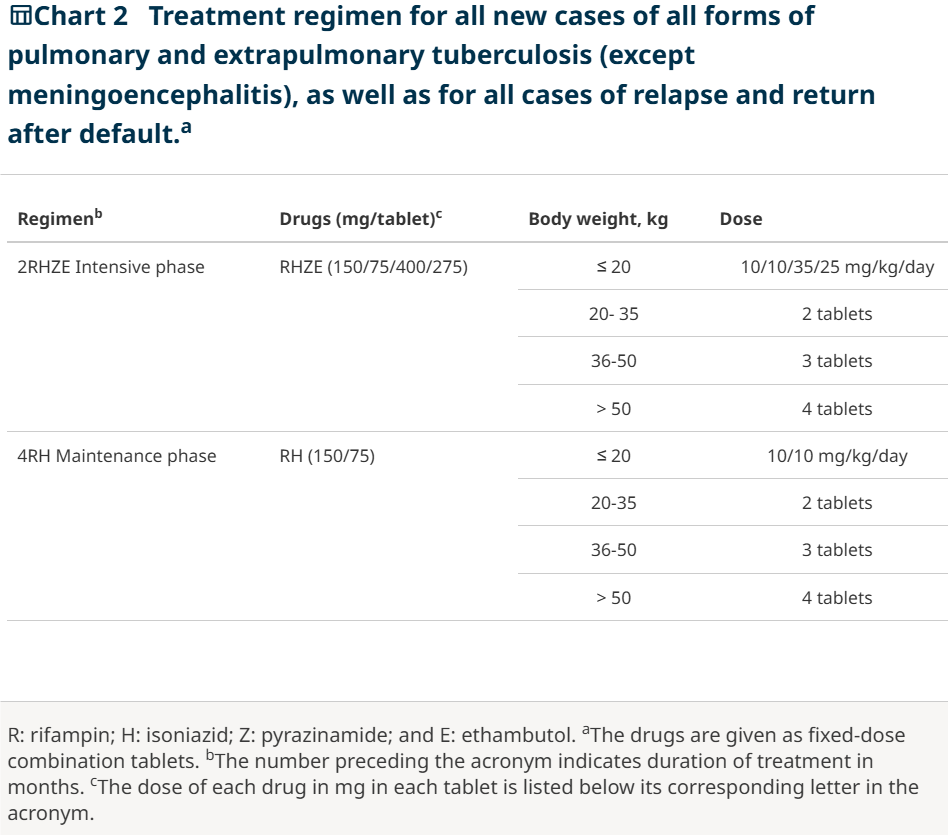
Furthermore, without conducting bioavailability or bioequivalence studies, the dosages of isoniazid and pyrazinamide in the tablets were decreased in the treatment change (from 400 mg to 300 mg and from 2,000 mg to 1,600 mg, respectively), in addition to the shift in presentation to FDC. Chart 2 shows the basic treatment plan currently in use in Brazil for people with tuberculosis who do not have a clinical suspicion of medication resistance. It is used for all kinds of the condition in patients over the age of ten and consists of a two-month intensive phase with the FDC RHZE regimen, followed by a four-month maintenance phase with the FDC RH regimen. Patients with tuberculosis-related meningitis are an exception; during the maintenance phase, they receive treatment for seven months with either an intravenous or oral corticosteroid (prednisone, at a rate of 1-2 mg/kg/day for four weeks).v. corticosteroid (dexamethasone, administered daily for four to eight weeks at a dose of 0.3–0.4 mg/kg). The drugs come in FDC tablet form. Each pill has 275 mg of ethambutol, 400 mg of pyrazinamide, 75 mg of isoniazid, and 150 mg of rifampin.
According to the PNCT tuberculosis guide, following consultation with a referral facility, the second phase of therapy may be prolonged for an additional seven months in the following circumstances:
· Patients with HIV/AIDS
· Patients whose direct smears show few organisms at 5 or 6 months of treatment, alone, as long as there is clinical and radiological improvement-treatment can be extended for an additional 3 months, at which period cases should be redefined or closed
· Patients with negative direct smears and an unsatisfactory clinical and radiological course
· Patients with cavitary forms who remain smear-positive at the end of the second month of treatment-in such cases, culture and drug susceptibility testing are mandatory
· Patients with monoresistance to rifampin or isoniazid, identified in the maintenance phase of treatment-a careful assessment of the clinical, bacteriological, and radiological course, as well as of adherence and previous tuberculosis treatment, should be performed at or under the guidance of a tertiary referral center
The literature indicates that smokers, patients with insulin-dependent diabetes, HIV infection, or other immunosuppressive conditions, and those whose weight is less than 10% of the ideal weight and whose weight gain is less than or equal to 5% during the intensive phase of treatment are among the people most at risk of relapse of tuberculosis (due to lack of sterilisation of the lesion). Extension of the maintenance phase of treatment should be taken into consideration for these people. Additionally, due to the increased risk of relapse, the maintenance phase of treatment may be prolonged for an extra three months in patients who had cavitation (total diameter ≥ 2 cm) on the initial chest X-ray and are culture positive for M. tuberculosis at the end of the first eight weeks of treatment (completion of the intensive phase of treatment). Sadly, drug susceptibility testing and sputum culture are only performed on 15–20% of pulmonary tuberculosis infections in Brazil.
A multidrug-resistant tuberculosis (MDR-TB) regimen is recommended when the basic regimen cannot be used due to intolerance to two or more medications. The use of the basic regimen should be continued until culture and drug susceptibility test results are available in cases of treatment failure (as defined by the PNCT: individuals who remain sputum smear-positive at the end of treatment; individuals who are positive and remain so until the fourth month of treatment; and individuals who have initial smear-positivity followed by smear-negativity and then smear-positivity again for two consecutive months, starting from the fourth month of treatment). Medication dosage errors, irregular medication use, and insufficient drug absorption should all be taken into account, as should the potential for nontuberculous mycobacterial infection. All medications used to treat tuberculosis, with the exception of rifapentine, have a higher bioavailability when administered on an empty stomach (the bioavailability of rifapentine increases by up to 86% with high-fat meals). Foods high in glucose or lactose should be avoided if the drugs must be taken with foods or beverages since these substances decrease the absorption of isoniazid. Medications used to treat tuberculosis frequently result in clinically significant changes in the concentrations of other medications, however few drug interactions can significantly alter the concentrations of these medications.
TUBERCULOSIS TREATMENT IN CHILDREN
Three drugs are used to treat patients under the age of ten in Brazil: pyrazinamide (35 mg/kg), isoniazid (10 mg/kg), and rifampin (10 mg/kg). This choice is based on the danger of ethambutol-related visual impairment, which can be challenging to diagnose in children, and the decreased chance of isoniazid resistance in patients with a low bacterial load, which is more common in children with tuberculosis.
The American Academy of Pediatrics27 recommends the four-drug treatment with ethambutol added during the intensive phase of treatment, along with monitoring of visual acuity and the capacity to distinguish between red and green colours, based on systematic reviews of the literature. The risk-benefit ratio of ethambutol use should be taken into account in children whose visual acuity cannot be checked. It should be noted that ethambutol can be routinely used to treat active tuberculosis in infants and children unless there is another contraindication. The WHO advises treating HIV-negative children with pulmonary tuberculosis who reside in regions with low rates of both HIV infection and isoniazid resistance with a three-drug regimen (RHZ regimen) during the induction phase without the inclusion of ethambutol. Ethambutol should be added to the regimen during the induction phase for children who reside in locations with high rates of HIV infection and/or isoniazid resistance.
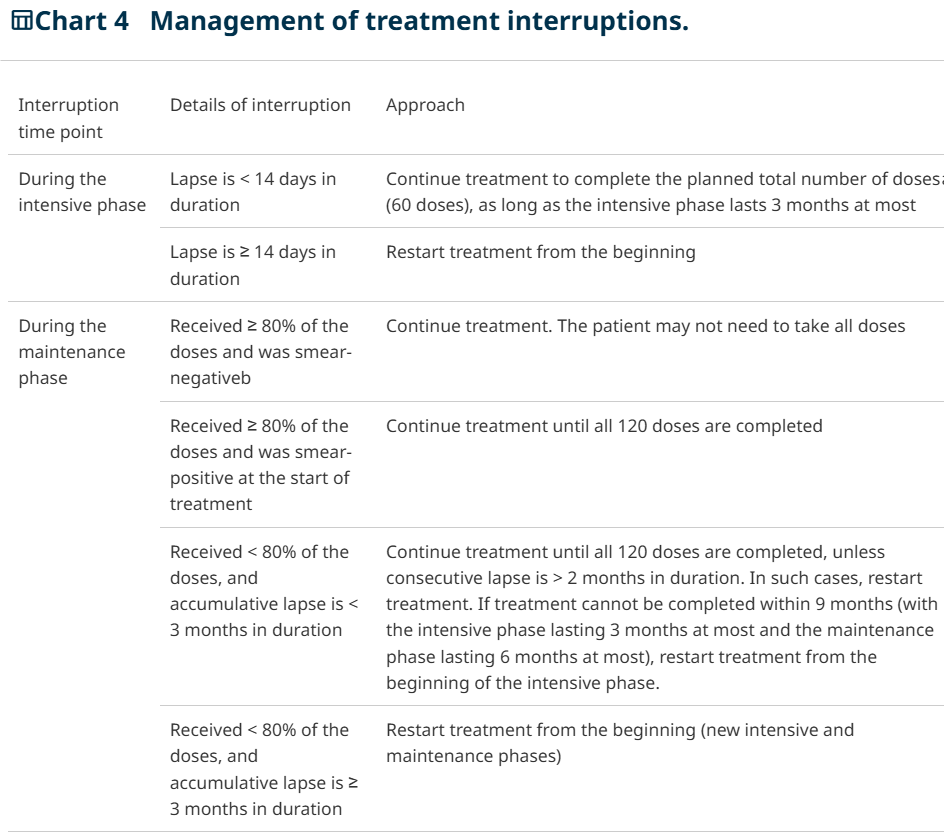
TUBRECULOSIS TREATMENT: APPROACHMENT IN CASE OF INTERRUPTIONS
Occasionally, patients interrupt drug therapy during treatment. Management of such cases in each of six circumstances
TUBERCULOSIS TREATMENT OUTCOMES
Similar to how tuberculosis cases must be reported for treatment beginning, treatment completion (result) must also be reported. The definitions of treatment result are listed below. In instances of tuberculosis that were bacteriologically proven at the beginning of treatment, cure is defined as a negative sputum smear or culture in the final month of treatment and at least once prior. A positive sputum smear or culture at five months or later while treatment is considered a failure. The term "default" refers to a tuberculosis treatment interruption that occurs at least 30 days after the anticipated date of return (for self-administered treatment) or 30 days after the last drug intake (DOT; see Chart 4 for treatment interruption management). A death brought on by tuberculosis that happens while receiving treatment is referred to as a death from tuberculosis. A death from a cause other than tuberculosis that happens while receiving treatment is referred to as a death from another cause.
DRUG-RESISTANT TUBERCULOSIS
The susceptibility of M. tuberculosis to first- and second-line medications used in the pharmacological treatment of this illness determines the classification of drug-resistant tuberculosis cases. The key terminology used in discussions about drug-resistant TB cases are defined here. Tuberculosis caused by organisms resistant to a single first-line antituberculosis medication is known as monodrug-resistant tuberculosis. Tuberculosis produced by organisms resistant to more than one first-line antituberculosis medication is known as polydrug-resistant TB (with the exception of isoniazid and rifampin, where resistance to both is referred to as multidrug resistance). Tuberculosis caused by organisms resistant to both isoniazid and rifampin is known as multidrug resistant tuberculosis (MDR-TB). Tuberculosis produced by organisms resistant to rifampin, isoniazid, a fluoroquinolone, and at least one of three injectable second-line medications (amikacin, kanamycin, or capreomycin) is known as extensively drug-resistant tuberculosis. The term "rifampin-resistant tuberculosis" refers to tuberculosis caused by organisms that have been found to be resistant to rifampin through rapid molecular testing for tuberculosis drug resistance. Since a significant percentage of cases found to be resistant to rifampin also have resistance to isoniazid, it is possible that other resistances are still unknown.
Mycobacterial resistance can be categorised as either primary or acquired, in addition to the classification of tuberculosis based on the organisms' treatment susceptibility. A bacillary population that is predominantly resistant to an antituberculosis medication causes primary resistance in tuberculosis. In these situations, the patients have never taken an antituberculosis medication and are infected with a strain of the disease that is already resistant, most likely due to acquired resistance. A bacillary population that is initially responsive to antituberculosis medications but later develops resistance to some of them is said to have acquired resistance. This kind of resistance is most likely the consequence of irregular or insufficient treatment because the frequency of spontaneous mutations is low and the use of an appropriate combination of drugs in the pharmacological treatment of tuberculosis makes the occurrence of clinically significant resistance unlikely.
DRUG-RESISTANT TUBERCULOSIS TREATMENT
Drug-resistant tuberculosis treatment depends on the type of resistance identified. The approaches in cases of monoresistance and polyresistance are described.
The MDR-TB treatment regimen should be used if multidrug resistance (resistance to RH or to RH and another first-line medication) is present. When drug susceptibility testing reveals ethambutol resistance, ethionamide is substituted for ethambutol; levofloxacin is used (in compliance with WHO recommendations); and capreomycin is added to the MDR-TB treatment regimen (as the injectable drug of choice because it produces fewer side effects and less cross-resistance with other injectable drugs). Because there are limitations to interpreting drug susceptibility testing findings, pyrazinamide should always be taken during the intensive period of therapy (do not use pyrazinamide just in situations of hepatotoxicity or severe adverse effects).
Then a quick molecular test for tuberculosis drug resistance indicates that a patient has rifampin-resistant tuberculosis, start treatment with the prescribed regimen and wait for the results of the drug susceptibility test. Determine the possibility of resistance on an individual basis if drug susceptibility testing reveals sensitivity to all medications. Regardless of how long the MDR-TB regimen is used, low-risk individuals should begin the basic regimen, which should be given for six months. Maintain the MDR-TB regimen in high-risk individuals (such as retreatment cases, contacts of MRD-TB patients, or alcohol and drug users).
Amikacin can be used as a substitute for capreomycin in individuals who have previously received treatment and do not have drug susceptibility testing-determined streptomycin resistance. Based on the drugs used and the findings of drug susceptibility tests, evaluate each case separately. A tertiary healthcare facility that specialises in treating drug-resistant tuberculosis is the best place to treat extensively drug-resistant tuberculosis. Salvage medications and customised regimens are employed.
CONCLUSION
Despite the availability of efficient treatment and prevention strategies, tuberculosis remains a significant global public health concern. Effective treatment of tuberculosis is crucial for both treating the afflicted person and stopping the infection from spreading across the community. Early diagnosis, proper anti-tubercular medication selection, rigorous adherence to the recommended regimen, and routine monitoring during the course of treatment are all critical to the effectiveness of TB treatment. When used correctly and consistently, standard first-line drugs including isoniazid, rifampicin, pyrazinamide, and ethambutol have demonstrated high efficacy.
Treatment compliance has significantly increased and the likelihood of treatment failure and relapse has decreased with the use of techniques like Directly Observed Treatment Short-course (DOTS). However, issues like drug toxicity, societal stigma, poor patient adherence, multidrug-resistant tuberculosis, and restricted access to healthcare continue to impact TB control initiatives globally. Thus, nutritional assistance, counselling, patient education, and routine follow-up are crucial elements of all-encompassing TB care.
To lessen the incidence of tuberculosis, public health systems must be strengthened, awareness must be raised, living circumstances must be improved, and access to high-quality healthcare services must be guaranteed. There is also potential for improved disease control in the future thanks to developments in diagnostic techniques and novel therapeutic strategies. All things considered, effective disease control and the eventual eradication of tuberculosis as a threat to world health depend on concerted efforts from medical professionals, patients, communities, and governments.
REFERENCE
1. A controlled trial of 6 months' chemotherapy in pulmonary tuberculosis. Final report: results during the 36 months after the end of chemotherapy and beyond. British Thoracic Society. Br J Dis Chest 1984;78(4):330-6. https://doi.org/10.1016/0007-0971(84)90165-7 » https://doi.org/10.1016/0007-0971(84)90165-7
2. Ahmad Khan F, Minion J, Al-Motairi A, Benedetti A, Harries AD, Menzies D. An updated systematic review and meta-analysis on the treatment of active tuberculosis in patients with HIV infection. Clin Infect Dis. 2012;55(8):1154-63. https://doi.org/10.1093/cid/cis630 » https://doi.org/10.1093/cid/cis630
3. Ai JW, Ruan QL, Liu QH, Zhang WH. Updates on the risk factors for latent tuberculosis reactivation and their managements. Emerg Microbes Infect. 2016;5:e10. https://doi.org/10.1038/emi.2016.10 » https://doi.org/10.1038/emi.2016.10
4. Alipanah N, Cattamanchi A, Menzies R, Hopewell PC, Chaisson RE, Nahid P. Treatment of non-cavitary pulmonary tuberculosis with shortened fluoroquinolone-based regimens: a meta-analysis. Int J Tuberc Lung Dis. 2016;20(11):1522-1528. https://doi.org/10.5588/ijtld.16.0217 » https://doi.org/10.5588/ijtld.16.0217
5. American Academy of Pediatrics. Committee on Infectious Diseases. 2015 Red Book: Report of the Committee on Infectious Diseases. 30th ed. Elk Grove Village, IL: AAP; 2015.
6. Baghaei P, Marjani M, Tabarsi P, Moniri A, Rashidfarrokhi F, Ahmadi F, et al. Impact of chronic renal failure on anti-tuberculosis treatment outcomes. Int J Tuberc Lung Dis. 2014;18(3):352-6. https://doi.org/10.5588/ijtld.13.0726 » https://doi.org/10.5588/ijtld.13.0726
7. Baker MA, Harries AD, Jeon CY, Hart JE, Kapur A, Lönnroth K, et al. The impact of diabetes on tuberculosis treatment outcomes: a systematic review. BMC Med. 2011;9:81. https://doi.org/10.1186/1741-7015-9-81 » https://doi.org/10.1186/1741-7015-9-81
8. Brasil. Ministério da Saúde. Departamento de Vigilância em Doenças Transmissíveis. Novas recomendações para tratamento da tuberculose multidrogarresistente e com resistência à rifampicina diagnosticada por meio do Teste Rápido Molecular para Tuberculose no Brasil. Nota informativa 8. Brasília: Ministério da Saúde; 2016.
9. Brasil. Ministério da Saúde. Departamento de Vigilância em Doenças Transmissíveis. Recomendações para controle de contatos e tratamento da infecção latente da tuberculose na indisponibilidade transitória do Derivado Proteico Purificado. Nota informativa 8. Brasília: Ministério da Saúde; 2014.
10. Brasil. Ministério da Saúde. Departamento de Vigilância Epidemiológica. Coordenação Geral de Doenças Endêmicas. Programa Nacional de Controle da Tuberculose. Plano Estratégico para o Controle da Tuberculose, Brasil 2007-2015. Brasília: Ministério da Saúde; 2006.
11. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Manual de recomendações para o controle da tuberculose no Brasil. Brasília: Ministério da Saúde; 2011.
12. Brasil. Ministério da Saúde. Sistema de Informação de Agravos de Notificação [homepage on the Internet]. Brasília: Ministério da Saúde [cited 2016 Oct 1]. Available from: http://www2.datasus.gov.br/DATASUS/index.php?area=0203&id=31009407&VObj=http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinannet/cnv/tuberc » http://www2.datasus.gov.br/DATASUS/index.php?area=0203&id=31009407&VObj=http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinannet/cnv/tuberc
13. Campbell J, Krot J, Marra F. Latent tuberculosis diagnostic tests to predict longitudinal tuberculosis during dialysis: a meta-analysis. Int J Tuberc Lung Dis. 2016;20(6):764-70. https://doi.org/10.5588/ijtld.15.0825 » https://doi.org/10.5588/ijtld.15.0825
14. Centers for Disease Control and Prevention. Managing tuberculosis patients and improving adherence. Atlanta, GA: CDC; 2014.
15. Chang KC, Leung CC, Yew WW, Ho SC, Tam CM. A nested case-control study on treatment-related risk factors for early relapse of tuberculosis. Am J Respir Crit Care Med. 2004;170(10):1124-30. https://doi.org/10.1164/rccm.200407-905OC » https://doi.org/10.1164/rccm.200407-905OC
16. Chien JY, Huang RM, Wang JY, Ruan SY, Chien YJ, Yu CJ, et al. Hepatitis C virus infection increases hepatitis risk during anti-tuberculosis treatment. Int J Tuberc Lung Dis. 2010;14(5):616-21.
17. Combs DL, O'Brien RJ, Geiter LJ. USPHS Tuberculosis Short-Course Chemotherapy Trial 21: effectiveness, toxicity, and acceptability. The report of final results. Ann Intern Med; 1990;112(6):397-406. https://doi.org/10.7326/0003-4819-76-3-112-6-397 » https://doi.org/10.7326/0003-4819-76-3-112-6-397
18. Conde MB, Efron A, Loredo C, De Souza GR, Graça NP, Cezar MC, et al. Moxifloxacin versus ethambutol in the initial treatment of tuberculosis: a double-blind, randomised, controlled phase II trial. Lancet. 2009;373(9670):1183-9. https://doi.org/10.1016/S0140-6736(09)60333-0 » https://doi.org/10.1016/S0140-6736(09)60333-0
19. Conde MB, Mello FC, Duarte RS, Cavalcante SC, Rolla V, Dalcolmo M, et al. A Phase 2 Randomized Trial of a Rifapentine plus Moxifloxacin-Based Regimen for Treatment of Pulmonary Tuberculosis. PLoS One. 2016;11(5):e0154778. https://doi.org/10.1371/journal.pone.0154778 » https://doi.org/10.1371/journal.pone.0154778
20. Conde MB, Melo FA, Marques AM, Cardoso NC, Pinheiro VG, Dalcin Pde T, et al. III Brazilian Thoracic Association Guidelines on tuberculosis. J Bras Pneumol. 2009;35(10):1018-48. https://doi.org/10.1590/S1806-37132009001000011 » https://doi.org/10.1590/S1806-37132009001000011
21. Conde MB, Souza MG. Pneumologia e tisiologia: uma abordagem prática. São Paulo: Atheneu; 2009.
22. Cruz MM, Cardoso GC, Abreu DM, Decotelli PV, Chrispim PP, Borenstein JS, et al. Adesão ao tratamento diretamente observado da tuberculose - o sentido atribuído pelos usuários e profissionais de saúde em duas regiões administrativas do município do Rio de Janeiro. Cad Saude Colet. 2012;20(2),217-24.
23. Czeizel AE, Rockenbauer M, Olsen J, Sørensen HT. A population-based case-control study of the safety of oral anti-tuberculosis drug treatment during pregnancy. Int J Tuberc Lung Dis. 2001;5(6):564-8.
24. Ferreira AC, Silva Júnior JL, Conde MB, Rabahi MF. Clinical treatment outcomes of tuberculosis treated with the basic regimen recommended by the Brazilian National Ministry of Health using fixed-dose combination tablets in the greater metropolitan area of Goiânia, Brazil. J Bras Pneumol. 2013;39(1):76-83. https://doi.org/10.1590/S1806-37132013000100011 » https://doi.org/10.1590/S1806-37132013000100011
25. Getahun H, Matteelli A, Abubakar I, Aziz MA, Baddeley A, Barreira D, et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur Respir J. 2015;46(6):1563-76. https://doi.org/10.1183/13993003.01245-2015 » https://doi.org/10.1183/13993003.01245-2015
26. GRADE working group [homepage on the Internet]. c2004-2017 [cited 2016 Oct 1]. Available from: http://www.gradeworkinggroup.org/ » http://www.gradeworkinggroup.org
27. Hijjar MA, Gerhardt G, Teixeira GM, Procópio MJ. Retrospect of tuberculosis control in Brazil. Rev Saude Publica. 2007;41(Suppl 1):50-8. https://doi.org/10.1590/S0034-89102007000800008 » https://doi.org/10.1590/S0034-89102007000800008
28. Horne DJ, Royce SE, Gooze L, Narita M, Hopewell PC, Nahid P, et al. Sputum monitoring during tuberculosis treatment for predicting outcome: systematic review and meta-analysis. Lancet Infect Dis. 2010;10(6):387-94. https://doi.org/10.1016/S1473-3099(10)70071-2 » https://doi.org/10.1016/S1473-3099(10)70071-2
29. Interrante JD, Haddad MB, Kim L, Gandhi NR. Exogenous Reinfection as a Cause of Late Recurrent Tuberculosis in the United States. Ann Am Thorac Soc. 2015;12(11):1619-26.
30. Jo KW, Yoo JW, Hong Y, Lee JS, Lee SD, Kim WS, et al. Risk factors for 1-year relapse of pulmonary tuberculosis treated with a 6-month daily regimen. Respir Med. 2014;108(4):654-9. https://doi.org/10.1016/j.rmed.2014.01.010 » https://doi.org/10.1016/j.rmed.2014.01.010
31. Karumbi J, Garner P. Directly observed therapy for treating tuberculosis. Cochrane Database Syst Rev. 2015;(5):CD003343. https://doi.org/10.1002/14651858.CD003343.pub4 » https://doi.org/10.1002/14651858.CD003343.pub4
32. Keane J, Gershon S, Wise RP, Mirabile-Levens E, Kasznica J, Schwieterman WD, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. N Engl J Med. 2001;345(15):1098-104. https://doi.org/10.1056/NEJMoa011110 » https://doi.org/10.1056/NEJMoa011110
33. Leung CC, Yew WW, Chan CK, Chang KC, Law WS, Lee SN, et al. Smoking adversely affects treatment response, outcome and relapse in tuberculosis. Eur Respir J. 2015;45(3):738-45. https://doi.org/10.1183/09031936.00114214 » https://doi.org/10.1183/09031936.00114214
34. Lienhardt C, Ogden JA. Tuberculosis control in resource-poor countries: have we reached the limits of the universal paradigm? Trop Med Int Health. 2004;9(7):833-41. https://doi.org/10.1111/j.1365-3156.2004.01273.x » https://doi.org/10.1111/j.1365-3156.2004.01273.x
35. Lomtadze N, Kupreishvili L, Salakaia A, Vashakidze S, Sharvadze L, Kempker RR, et al. Hepatitis C virus co-infection increases the risk of anti-tuberculosis drug-induced hepatotoxicity among patients with pulmonary tuberculosis. PLoS One. 2013;8(12):e83892. https://doi.org/10.1371/journal.pone.0083892 » https://doi.org/10.1371/journal.pone.0083892
36. Maciel EL, Guidoni LM, Favero JL, Hadad DJ, Molino LP, Jonhson JL, et al. Adverse effects of the new tuberculosis treatment regimen recommended by the Brazilian Ministry of Health. J Bras Pneumol. 2010;36(2):232-8. https://doi.org/10.1590/S1806-37132010000200012 » https://doi.org/10.1590/S1806-37132010000200012
37. Mack U, Migliori GB, Sester M, Rieder HL, Ehlers S, Goletti D, et al. LTBI: latent tuberculosis infection or lasting immune responses to M. tuberculosis? A TBNET consensus statement. Eur Respir J. 2009;33(5):956-73. https://doi.org/10.1183/09031936.00120908 » https://doi.org/10.1183/09031936.00120908
38. Malone RS, Fish DN, Spiegel DM, Childs JM, Peloquin CA. The effect of hemodialysis on isoniazid, rifampin, pyrazinamide, and ethambutol. Am J Respir Crit Care Med. 1999;159(5 Pt 1):1580-4. https://doi.org/10.1164/ajrccm.159.5.9810034 » https://doi.org/10.1164/ajrccm.159.5.9810034
39. Marais BJ. Twelve-dose drug regimen now also an option for preventing tuberculosis in children and adolescents. JAMA Pediatr. 2015;169(3):208-10. https://doi.org/10.1001/jamapediatrics.2014.3157 » https://doi.org/10.1001/jamapediatrics.2014.3157
40. Mota LM, Cruz BA, Brenol CV, Pollak DF, Pinheiro Gda R, Laurindo IM, et al. Safe use of biological therapies for the treatment of rheumatoid arthritis and spondyloarthritides [Article in Portuguese]. Rev Bras Reumatol. 2015;55(3):281-309. https://doi.org/10.1016/j.rbr.2014.06.006 » https://doi.org/10.1016/j.rbr.2014.06.006
41. Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):e238. https://doi.org/10.1371/journal.pmed.0040238 » https://doi.org/10.1371/journal.pmed.0040238
42. Nahid P, Dorman SE, Alipanah N, Barry PM, Brozek JL, Cattamanchi A, et al. Executive Summary: Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis. 2016;63(7):853-67. https://doi.org/10.1093/cid/ciw566 » https://doi.org/10.1093/cid/ciw566
43. Parida A, Bairy KL, Chogtu B, Magazine R, Vidyasagar S. Comparison of Comparison of Directly Observed Treatment Short Course (DOTS) with Self-Administered Therapy in Pulmonary Tuberculosis in Udupi District of Southern India. J Clin Diagn Res. 2014;8(8):HC29-31.
44. Pasipanodya JG, Gumbo T. A meta-analysis of self-administered vs directly observed therapy effect on microbiologic failure, relapse, and acquired drug resistance in tuberculosis patients. Clin Infect Dis. 2013;57(1):21-31. https://doi.org/10.1093/cid/cit167 » https://doi.org/10.1093/cid/cit167
45. Piccazzo R, Paparo F, Garlaschi G. Diagnostic accuracy of chest radiography for the diagnosis of tuberculosis (TB) and its role in the detection of latent TB infection: a systematic review. J Rheumatol Suppl. 2014;91:32-40. https://doi.org/10.3899/jrheum.140100 » https://doi.org/10.3899/jrheum.140100
46. Ruffino Netto A. Impacto da reforma do setor saúde sobre os serviços de tuberculose no Brasil. Bol Pneumol Sanit. 1999;7(1):7-18. https://doi.org/10.5123/S0103-460X1999000100002 » https://doi.org/10.5123/S0103-460X1999000100002
47. Sant'Anna CC. Childhood tuberculosis. J Pediatr (Rio J). 1998;74 Suppl 1:S69-75. https://doi.org/10.2223/JPED.488 » https://doi.org/10.2223/JPED.488
48. Seaworth BJ, Armitige LY, Griffith DE. First do no harm--adverse events, drug intolerance, and hepatotoxicity: how can we not justify directly observed therapy for treating tuberculosis? Clin Infect Dis. 2013;57(7):1063-4. https://doi.org/10.1093/cid/cit432 » https://doi.org/10.1093/cid/cit432
49. Sester M, Kampmann B. What defines latent infection with Mycobacterium tuberculosis in patients with autoimmune diseases? Thorax. 2016;71(1):3-4. https://doi.org/10.1136/thoraxjnl-2015-207991 » https://doi.org/10.1136/thoraxjnl-2015-207991
50. Singh N, Paterson DL. Mycobacterium tuberculosis infection in solid-organ transplant recipients: impact and implications for management. Clin Infect Dis. 1998;27(5):1266-77. https://doi.org/10.1086/514993 » https://doi.org/10.1086/514993 51. Sotgiu G, Nahid P, Loddenkemper R, Abubakar I, Miravitlles M, Migliori GB. The ERS-endorsed official ATS/CDC/IDSA clinical practice guidelines on treatment of drug-susceptible tuberculosis. Eur Respir J. 2016;48(4):963-71. https://doi.org/10.1183/13993003.01356-2016 » https://doi.org/10.1183/13993003.01356-2016
52. Sterling TR, Villarino ME, Borisov AS, Shang N, Gordin F, Bliven-Sizemore E, et al. Three months of rifapentine and isoniazid for latent tuberculosis infection. N Engl J Med. 2011;365(23):2155-66. https://doi.org/10.1056/NEJMoa1104875 » https://doi.org/10.1056/NEJMoa1104875
53. Sun HY, Chen YJ, Gau CS, Chang SC, Luh KT. A prospective study of hepatitis during antituberculous treatment in Taiwanese patients and a review of the literature. J Formos Med Assoc. 2009;108(2):102-11. https://doi.org/10.1016/S0929-6646(09)60040-1 » https://doi.org/10.1016/S0929-6646(09)60040-1
54. TB CARE I. International Standards for Tuberculosis Care Edition 3. The Hague: TB CARE I; 2014.
55. Verver S, Warren RM, Beyers N, Richardson M, van der Spuy GD, Borgdorff MW, et al. Rate of reinfection tuberculosis after successful treatment is higher than rate of new tuberculosis. Am J Respir Crit Care Med. 2005;171(12):1430-5. https://doi.org/10.1164/rccm.200409-1200OC » https://doi.org/10.1164/rccm.200409-1200OC
56. Villarino ME, Scott NA, Weis SE, Weiner M, Conde MB, Jones B, et al. Treatment for preventing tuberculosis in children and adolescents: a randomized clinical trial of a 3-month, 12-dose regimen of a combination of rifapentine and isoniazid. JAMA Pediatr. 2015;169(3):247-55. Erratum in: JAMA Pediatr. 2015;169(9):878. https://doi.org/10.1001/jamapediatrics.2014.3158 » https://doi.org/10.1001/jamapediatrics.2014.3158
57. Wong SH, Gao Q, Tsoi KK, Wu WK, Tam LS, Lee N, et al. Effect of immunosuppressive therapy on interferon ? release assay for latent tuberculosis screening in patients with autoimmune diseases: a systematic review and meta-analysis. Thorax. 2016;71(1):64-72. https://doi.org/10.1136/thoraxjnl-2015-207811 » https://doi.org/10.1136/thoraxjnl-2015-207811
58. World Health Organization [homepage on the Internet]. Geneva: WHO [updated 2014; cited 2016 Oct 1]. Guidance for national tuberculosis programmes on the management of tuberculosis in children. 2nd ed. [Adobe Acrobat document, 146p.]. Available from: http://apps.who.int/medicinedocs/documents/s21535en/s21535en.pdfn » http://apps.who.int/medicinedocs/documents/s21535en/s21535en.pdf
59. World Health Organization [homepage on the Internet]. Geneva: WHO [updated 2014 Dec; cited 2016 Oct 1]. Definitions and reporting framework for tuberculosis-2013 revision. [Adobe Acrobat document, 47p.]. Available from: http://apps.who.int/iris/bitstream/10665/79199/1/9789241505345_eng.pdf, http://apps.who.int/iris/bitstream/10665/79199/1/9789241505345_eng.pdf
60. Zvada SP, Van Der Walt JS, Smith PJ, Fourie PB, Roscigno G, Mitchison D, et al. Effects of four different meal types on the population pharmacokinetics of single-dose rifapentine in healthy male volunteers. Antimicrob Agents Chemother. 2010;54(8):3390-4. https://doi.org/10.1128/AAC.00345-10 » https://doi.org/10.1128/AAC.00345-10