
Methodological Recommendations and Standards for the Diagnosis and Treatment of Chronic Clinical Forms of Coronary Heart Disease: Heart Failure
1. Ahmad Aqeel
Tamomita Nandi
Mohd Nazim
2. A. Esengeldi kyzy
(1. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
Chronic Coronary Heart Disease (CHD) remains the leading global etiology of chronic Heart Failure (HF), culminating in a clinical entity frequently termed ischemic cardiomyopathy. The transition from chronic myocardial ischemia to overt mechanical pump failure represents a complex continuum of maladaptive neurohormonal activation and structural ventricular remodeling. This article reviews the current methodological recommendations and evidence-based standards for the diagnosis and treatment of CHD-induced heart failure. We examine the critical diagnostic pillars, including natriuretic peptide biomarker testing and advanced echocardiography, to stratify patients into Heart Failure with Reduced Ejection Fraction (HFrEF) and Preserved Ejection Fraction (HFpEF). Furthermore, we detail the radical evolution of Guideline-Directed Medical Therapy (GDMT), shifting from sequential step-up approaches to the rapid, simultaneous initiation of the foundational "Fantastic Four" pharmacological pillars: ARNI, Beta-blockers, MRAs, and SGLT2 inhibitors. Finally, the role of structural interventions, including surgical revascularization and device therapy (ICD/CRT), is analyzed within the context of comprehensive, multidisciplinary outpatient management.
Keywords: Chronic Coronary Heart Disease, Ischemic Cardiomyopathy, Heart Failure (HFrEF), Guideline-Directed Medical Therapy (GDMT), Ventricular Remodeling, Echocardiography.
1. Introduction
The intersection of Chronic Coronary Heart Disease (CHD) and Heart Failure (HF) represents one of the most formidable challenges in modern cardiovascular medicine. Heart failure is not a standalone diagnosis; rather, it is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood [1]. In industrialized nations, chronic CHD is the underlying culprit in over 60% of all HF cases.
Historically, the medical approach to ischemic heart failure was primarily palliative, focusing on symptom relief through aggressive diuresis. However, modern methodological recommendations—driven by major bodies such as the American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology (ESC)—have shifted the paradigm towards disease modification [2]. The contemporary standard of care demands early identification of ischemic etiology, aggressive halting of neurohormonal pathways, and strategic revascularization to salvage hibernating myocardium and reverse left ventricular dysfunction.
2. Pathophysiology: Ischemia and Ventricular Remodeling
To effectively manage ischemic heart failure, the clinician must understand the biomechanical and molecular alterations that occur when the myocardium is subjected to chronic hypoperfusion or recurrent micro-infarctions.
2.1 The Concept of Hibernating Myocardium
In the setting of chronic coronary artery stenosis, the heart muscle may downregulate its contractile function to match the severely restricted oxygen supply, a state known as "hibernating myocardium" [3]. While this protects the myocytes from immediate necrosis, it manifests clinically as chronic systolic dysfunction. Crucially, this state is potentially reversible upon restoration of blood flow (revascularization).
2.2 Neurohormonal Activation and Remodeling
When cardiac output falls due to ischemic damage, the body interprets this as a state of volume depletion. The sympathetic nervous system (SNS) and the Renin-Angiotensin-Aldosterone System (RAAS) are heavily activated [1]. While these compensatory mechanisms temporarily maintain blood pressure through vasoconstriction and fluid retention, their chronic activation is profoundly cardiotoxic. High levels of angiotensin II and aldosterone drive myocardial fibrosis, while catecholamines induce myocyte apoptosis [4]. This relentless cycle leads to ventricular remodeling—the left ventricle dilates, becomes spherical, and loses its mechanical efficiency, ultimately transforming compensated ischemia into end-stage pump failure.
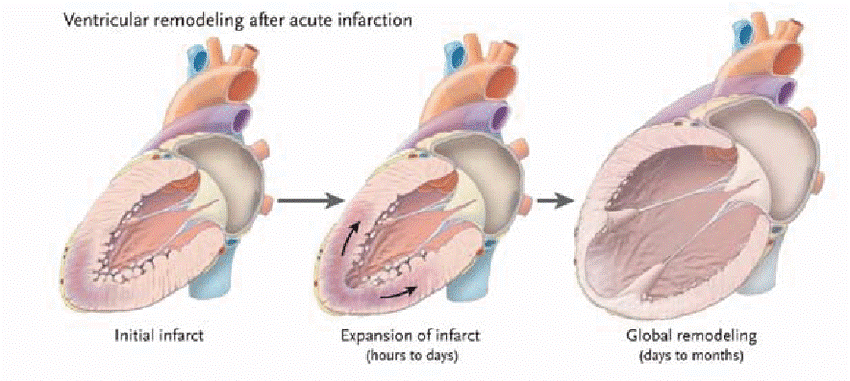
Figure 1. The process of Left Ventricular Remodeling following ischemic injury. The diagram illustrates how an initial ischemic insult (e.g., myocardial infarction or chronic severe ischemia) triggers neurohormonal cascades that cause progressive chamber dilation, wall thinning, and spherical geometric changes, severely compromising mechanical efficiency.
(Source: Zipes, D. P., Libby, P., Bonow, R. O., et al. (2021). Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th ed. Elsevier).
3. Methodological Standards for Diagnosis
The diagnostic protocol for chronic heart failure requires a structured algorithmic approach, combining clinical acumen with high-fidelity imaging and biomarker analysis to determine the precise phenotype and underlying ischemic burden.
3.1 Biomarker Profiling (Natriuretic Peptides)
The methodological standard for the initial biochemical evaluation of suspected HF is the measurement of B-type Natriuretic Peptide (BNP) or N-terminal pro-B-type Natriuretic Peptide (NT-proBNP). These peptides are released by ventricular stretch [2]. Elevated levels (e.g., NT-proBNP > 125 pg/mL in the outpatient setting) establish the diagnosis of HF and correlate directly with disease severity and prognosis. Conversely, a normal level carries a high negative predictive value, effectively ruling out HF as the cause of dyspnea [1].
3.2 Echocardiographic Stratification
Transthoracic Echocardiography (TTE) is the cornerstone of structural diagnosis. The ESC and ACC/AHA guidelines strictly classify HF based on the Left Ventricular Ejection Fraction (LVEF):
Ø HFrEF (Reduced): LVEF ≤ 40%. This is the classic presentation of ischemic cardiomyopathy, characterized by a dilated, poorly contracting ventricle.
Ø HFmrEF (Mildly Reduced): LVEF 41-49%.
Ø HFpEF (Preserved): LVEF ≥ 50%. Often seen in elderly patients with concurrent hypertension and microvascular ischemia, characterized by a stiff, non-compliant ventricle with impaired diastolic filling [5].
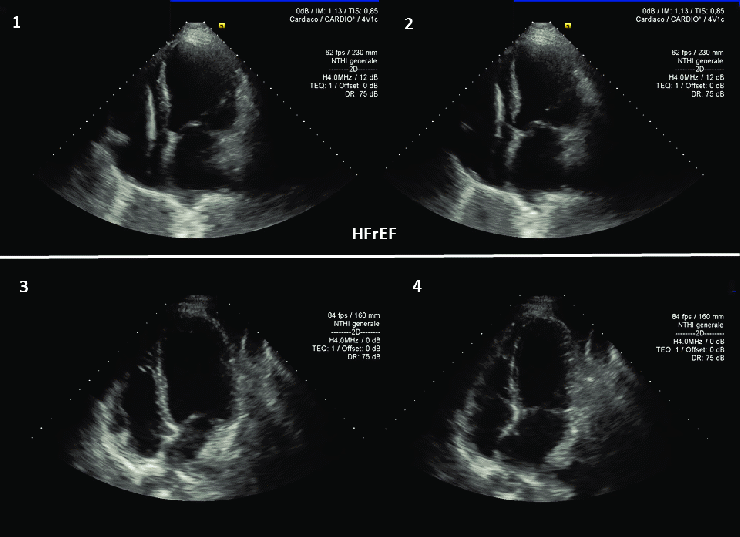
Figure 2. Apical four-chamber view on Transthoracic Echocardiography (TTE) demonstrating a dilated left ventricle characteristic of Heart Failure with Reduced Ejection Fraction (HFrEF) secondary to chronic ischemic disease. TTE is mandatory for assessing LVEF, regional wall motion abnormalities, and secondary valvular pathologies like functional mitral regurgitation.
(Source: Lang, R. M., et al., Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults, JASE, 2015).
3.3 Defining the Ischemic Etiology
Because the presence of CHD radically alters the therapeutic approach, all patients with newly diagnosed HF must undergo evaluation for coronary anatomy. Depending on the patient's pre-test probability, this involves either non-invasive anatomical imaging (Coronary Computed Tomography Angiography - CCTA) or invasive standard Coronary Angiography to identify flow-limiting stenoses amenable to surgical bypass or percutaneous intervention [2].
4. Pharmacological Treatment: Guideline-Directed Medical Therapy (GDMT)
The pharmacological management of HFrEF has undergone a revolutionary shift. Current methodological standards have abandoned the historical "stepwise" introduction of drugs in favor of rapid, simultaneous initiation of four foundational pillars, colloquially termed the "Fantastic Four," to block multiple maladaptive pathways simultaneously.
4.1 Renin-Angiotensin System Inhibition (ARNI/ACEi)
The cornerstone of anti-remodeling therapy is the Angiotensin Receptor-Neprilysin Inhibitor (ARNI, e.g., Sacubitril/Valsartan). ARNIs not only block the cardiotoxic RAAS pathway but simultaneously inhibit the degradation of beneficial natriuretic peptides. Methodological guidelines now recommend ARNIs as a Class I replacement for traditional ACE inhibitors to further reduce cardiovascular mortality and hospitalizations [4].
4.2 Beta-Blockers
Beta-blockers (specifically Carvedilol, Metoprolol Succinate, or Bisoprolol) shield the failing myocardium from the toxic effects of chronic sympathetic overdrive. By lowering heart rate, they increase diastolic filling time and myocardial perfusion, which is exceptionally critical in hearts affected by chronic coronary disease [1].
4.3 Mineralocorticoid Receptor Antagonists (MRAs)
Agents like Spironolactone or Eplerenone block aldosterone receptors. Aldosterone is a primary driver of myocardial fibrosis and ventricular stiffening. By antagonizing this receptor, MRAs halt progressive structural degradation and reduce sudden cardiac death [5].
4.4 SGLT2 Inhibitors
Originally developed as oral antidiabetics, Sodium-Glucose Cotransporter-2 (SGLT2) inhibitors (e.g., Dapagliflozin, Empagliflozin) represent the newest pillar of HF therapy. Independent of their effect on blood sugar, they induce osmotic diuresis, reduce cardiac preload and afterload, and improve myocardial energetics. They are now mandated by ACC/AHA guidelines for all HFrEF patients, regardless of diabetes status, due to their profound mortality benefit [2].
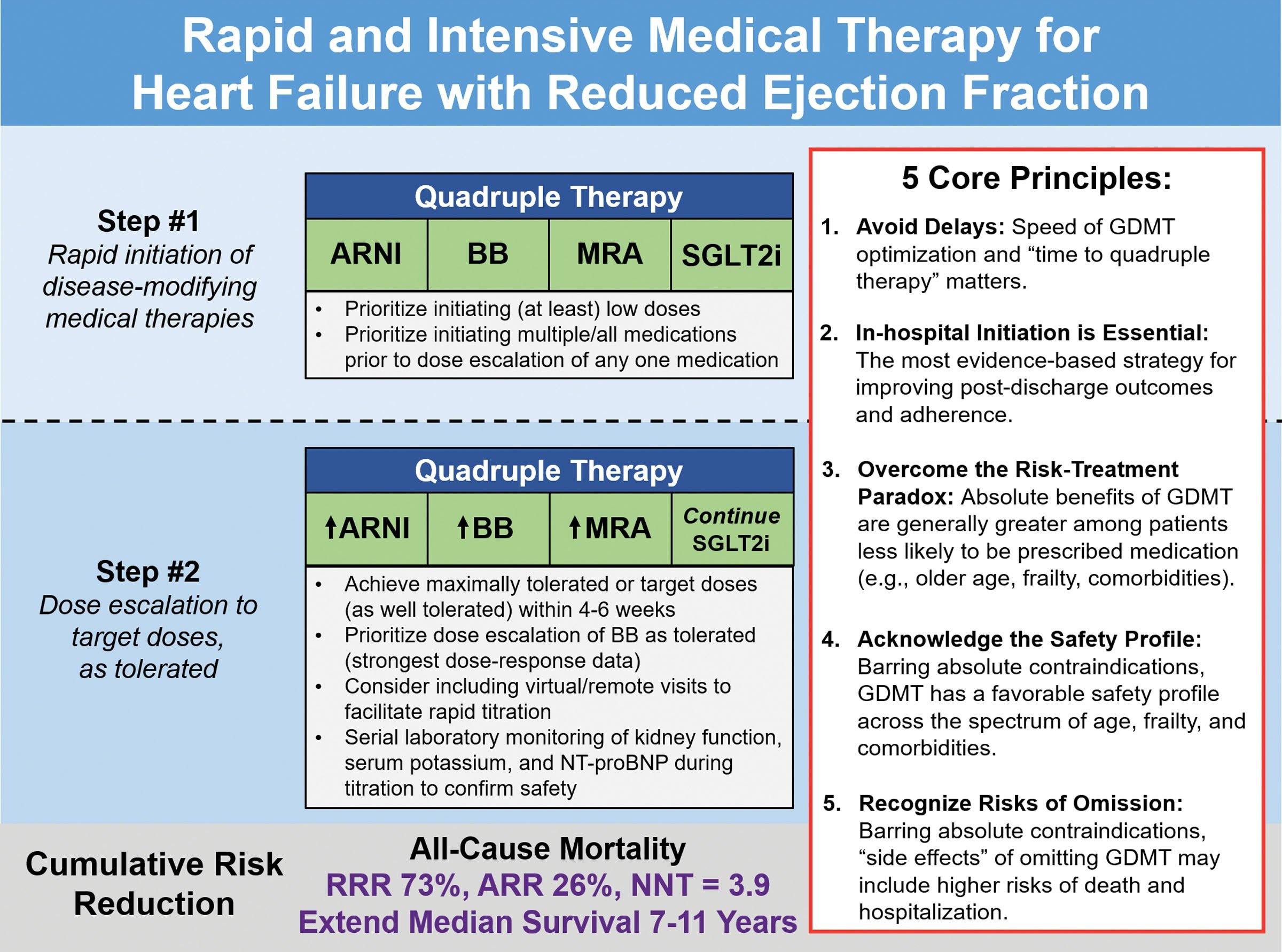
Figure 3. The contemporary Guideline-Directed Medical Therapy (GDMT) algorithm for Heart Failure with Reduced Ejection Fraction (HFrEF). The graphic highlights the mandatory, rapid initiation of the four foundational drug classes (ARNI, Beta-blocker, MRA, SGLT2i) to optimally alter the trajectory of the disease.
(Source: Heidenreich, P. A., et al., 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure, Circulation, 2022).
5. Interventional and Device Therapies
When ischemic heart failure progresses despite optimal medical therapy, or when a clear anatomical target is identified, the standard of care escalates to procedural intervention.
5.1 Surgical Revascularization (CABG)
In patients with ischemic cardiomyopathy (LVEF ≤ 35%) and severe multivessel coronary artery disease, Coronary Artery Bypass Grafting (CABG) is superior to medical therapy alone for long-term survival. The STICH trial definitively proved that revascularizing hibernating myocardium leads to significant reverse remodeling and improved left ventricular function over a 10-year follow-up period [3].
5.2 Implantable Cardioverter-Defibrillators (ICD) and CRT
Patients with chronic ischemic damage are at a phenomenally high risk for lethal ventricular arrhythmias due to scar tissue acting as an arrhythmogenic substrate.
v ICD: Primary prevention with an ICD is indicated for patients whose LVEF remains ≤ 35% despite at least 3 months of maximal GDMT [1].
v Cardiac Resynchronization Therapy (CRT): In advanced HF, the left and right ventricles often contract out of sync (manifesting as a Left Bundle Branch Block on ECG). A CRT device (a biventricular pacemaker) forces the ventricles to contract simultaneously, immediately improving mechanical efficiency, reversing remodeling, and reducing mortality [5].
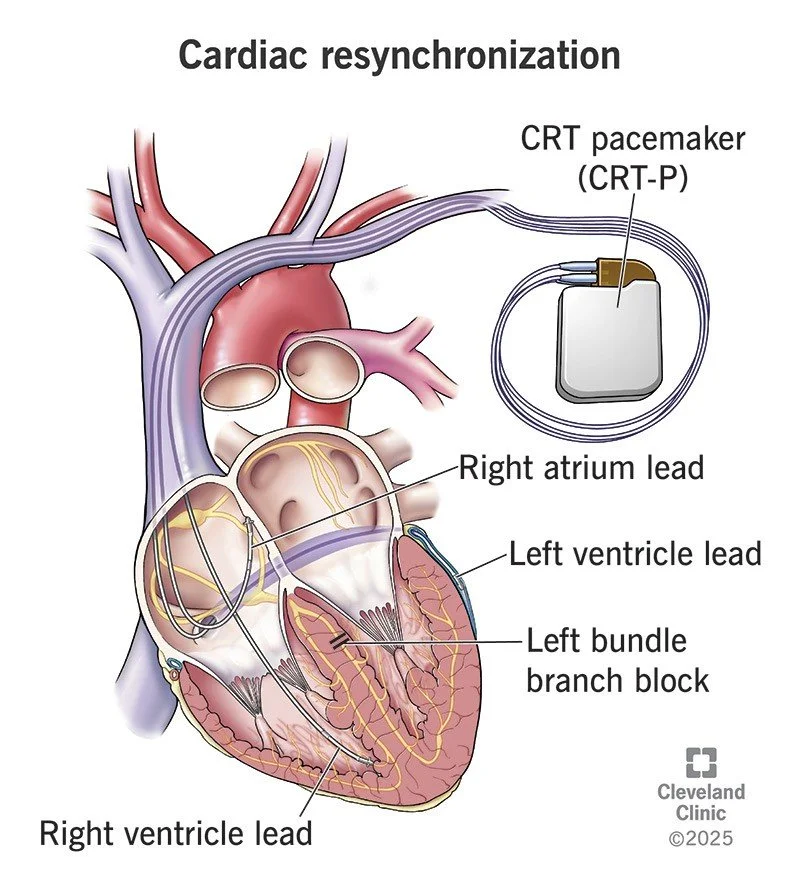
Figure 4. Schematic of a Cardiac Resynchronization Therapy (CRT) system. Unlike a standard pacemaker, CRT utilizes three leads (right atrium, right ventricle, and the coronary sinus to pace the lateral wall of the left ventricle) to restore synchronous mechanical contraction in hearts severely dilated by ischemic disease.
(Source: Jameson, J. L., et al., Harrison’s Principles of Internal Medicine, 21st ed., McGraw Hill, 2022).
6. Conclusion
The management of chronic heart failure secondary to coronary heart disease is a triumph of modern evidence-based medicine. The clinical approach has evolved from simplistic symptomatic relief to targeted molecular and biomechanical intervention. Strict adherence to methodological standards—from precise echocardiographic phenotyping to the rapid deployment of comprehensive, four-pillar Guideline-Directed Medical Therapy—is essential to halt the vicious cycle of ischemic ventricular remodeling. Furthermore, by seamlessly integrating advanced surgical revascularization and electrophysiological device therapy, the modern clinician can fundamentally alter the natural history of the disease, granting patients not only an extension of life, but a restoration of functional capacity.
7. References
[1] Jameson, J. L., Fauci, A. S., Kasper, D. L., Hauser, S. L., Longo, D. L., & Loscalzo, J. (2022). Harrison's Principles of Internal Medicine (21st ed.). McGraw Hill. ISBN: 978-1264268504.
[2] Heidenreich, P. A., Bozkurt, B., Aguilar, D., et al. (2022). 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 145(18), e895-e1032. https://doi.org/10.1161/CIR.0000000000001063
[3] Zipes, D. P., Libby, P., Bonow, R. O., Mann, D. L., & Tomaselli, G. F. (2021). Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (12th ed.). Elsevier. ISBN: 978-0323824675.
[4] McMurray, J. J., Packer, M., Desai, A. S., et al. (2014). Angiotensin-neprilysin inhibition versus enalapril in heart failure. The New England Journal of Medicine, 371(11), 993–1004. https://doi.org/10.1056/NEJMoa1409077
[5] McDonagh, T. A., Metra, M., Adamo, M., et al. (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 42(36), 3599–3726. https://doi.org/10.1093/eurheartj/ehab368