Epidemiology in Public Health: Basic Principles and Methods
1. Kalybekova K.D.
2. Rishikesh Kumar
Faizan Ul Haq
Pranavkumar Purushottam
(1. Teacher, Public Health Dept., International Medical Faculty, Osh State University, Osh, Kyrgyzstan.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyzstan.)
Abstract
Epidemiology constitutes the foundational science of public health, providing the conceptual and methodological framework necessary to understand the distribution, determinants, and control of health-related events in human populations. This article presents a comprehensive review of the basic principles and methods of epidemiology as they apply to public health practice. Drawing upon authoritative sources including the World Health Organization (WHO), the U.S. Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), and peer-reviewed literature indexed in PubMed, the article covers epidemiological definitions, core measures of disease frequency, major study designs, concepts of causation, the Bradford Hill criteria, bias and confounding, public health surveillance, and the contemporary global burden of disease. The noncommunicable disease crisis — responsible for at least 43 million deaths in 2021, equivalent to 75% of non-pandemic-related deaths globally (WHO, 2024) — underscores the urgency of rigorous epidemiological inquiry. This review is intended as a reference for students, researchers, public health professionals, and policymakers.
Keywords: Epidemiology, Public Health, Disease Surveillance, Study Design, Causation, Incidence, Prevalence, Bradford Hill Criteria, Global Burden of Disease
1. Introduction
Epidemiology is widely regarded as the cornerstone of public health. The discipline provides the scientific tools and conceptual logic required to investigate the origins, distribution, and prevention of disease in human populations. As described in the WHO publication Basic Epidemiology (2nd ed.), epidemiology enables health professionals to describe the common causes of death, disease, and disability in a community; to outline appropriate study designs for specific research questions; and to critically evaluate the scientific literature.
The word "epidemiology" derives from three Greek roots: epi (upon), demos (people), and logos (study). In its modern usage, epidemiology is defined as the study of the distribution and determinants of health-related states or events in specified populations, and the application of this knowledge to the control of health problems (CDC, Principles of Epidemiology in Public Health Practice, 3rd Edition, SS1978).
Epidemiology is both a science and a practice. As a science, it relies on quantitative methods, probability, and biostatistics. As a public health discipline, it is animated by a commitment to action — the translation of data into policies, programs, and interventions that protect and promote population health. The CDC defines this applied dimension as "applied epidemiology," reflecting the deployment of epidemiological principles to address real-world public health problems.
The relevance of epidemiology has never been greater. According to WHO (2024), noncommunicable diseases (NCDs) killed at least 43 million people in 2021, equivalent to 75% of all non-pandemic-related deaths globally. The Global Burden of Disease Study 2021 (GBD 2021) further documents that cardiovascular diseases, neoplasms, chronic respiratory diseases, and diabetes collectively accounted for 43.8 million deaths (64.5% of total deaths) in 2021, generating 1.73 billion disability-adjusted life years (DALYs). These staggering figures affirm that sound epidemiological investigation is a prerequisite for effective public health response.
2. Definition and Scope of Epidemiology
The most widely cited definition of epidemiology, endorsed by the CDC, is: "Epidemiology is the study of the distribution and determinants of health-related states or events in specified populations, and the application of this knowledge to the control of health problems." Each element of this definition is meaningful and warrants elaboration.
2.1 Distribution
Epidemiology is concerned with the frequency and pattern of health events in a population. Frequency includes not only the number of events (cases of disease, deaths, injuries) but also the rate or risk of disease, which allows valid comparisons across populations of different sizes. Pattern refers to the occurrence of health events by person, place, and time — the epidemiological triad of descriptive analysis.
2.2 Determinants
Epidemiology seeks to identify the causes and factors that influence the occurrence of disease. Determinants may be biological (genetic susceptibility, pathogen virulence), behavioral (tobacco use, physical inactivity, dietary habits), social (poverty, education, housing), environmental (air quality, water sanitation), or healthcare-related. Understanding determinants guides the development of interventions.
2.3 Specified Populations
Unlike clinical medicine — which focuses on the individual patient — epidemiology focuses on the population as its unit of analysis. This perspective enables the identification of at-risk groups, the quantification of disease burden across communities, and the design of population-level preventive strategies.
2.4 Application to Disease Control
The ultimate purpose of epidemiology is action. Epidemiological data inform public health surveillance, outbreak investigation, disease control policies, vaccination programs, screening recommendations, and health resource allocation. As the WHO Basic Epidemiology text states, epidemiology "shows how good clinical practice is informed by clinical epidemiology" and prepares health professionals "to ensure that health resources are used to the best possible effect."
3. Historical Background
The intellectual history of epidemiology is rich and stretches across centuries, though the formal discipline emerged during the 19th century. Several landmark contributions are essential to understanding modern epidemiological practice.
John Snow (1813–1858) is often celebrated as the father of modern epidemiology for his systematic investigation of the 1854 cholera outbreak in London's Soho district. By mapping cases and identifying the contaminated Broad Street pump as the source, Snow demonstrated the power of geographic analysis and the removal of a source to interrupt disease transmission — decades before the germ theory of disease was established.
Ignaz Semmelweis (1818–1865) demonstrated through systematic observation that handwashing by physicians dramatically reduced puerperal (childbed) fever mortality in Vienna maternity wards, foreshadowing modern infection control principles. John Graunt (1620–1674) laid the foundation for vital statistics by analyzing London's Bills of Mortality, introducing the concept of quantitative analysis of population health data.
In the 20th century, the Framingham Heart Study (commenced 1948) pioneered the cohort study design and identified major risk factors for cardiovascular disease, including hypertension, hypercholesterolemia, and smoking — findings that continue to shape cardiology and public health practice globally. The landmark work of Sir Richard Doll and Austin Bradford Hill in the 1950s, establishing the causal link between cigarette smoking and lung cancer through rigorous epidemiological methods, set a methodological standard that endures.
Austin Bradford Hill's 1965 Presidential Address to the Royal Society of Medicine, in which he articulated nine criteria for establishing causality, remains one of the most cited frameworks in epidemiological literature and is referenced by agencies including the EPA, FDA, and CDC to this day.
4. Measures of Disease Frequency
Quantifying the occurrence of disease in populations is a primary function of epidemiology. As noted by the NIH National Library of Medicine (NLM), incidence and prevalence are the most fundamental measures of morbidity, and both are essential for understanding the burden of disease in a community. The CDC's Principles of Epidemiology in Public Health Practice identifies incidence, prevalence, and mortality rates as the three core frequency measures used to characterize health events in populations.
4.1 Incidence
Incidence refers to the number of new cases of a disease that arise in a specific population during a defined time period. It measures the rate at which disease is developing in a population and is fundamental for risk assessment, disease tracking, and the evaluation of public health interventions.
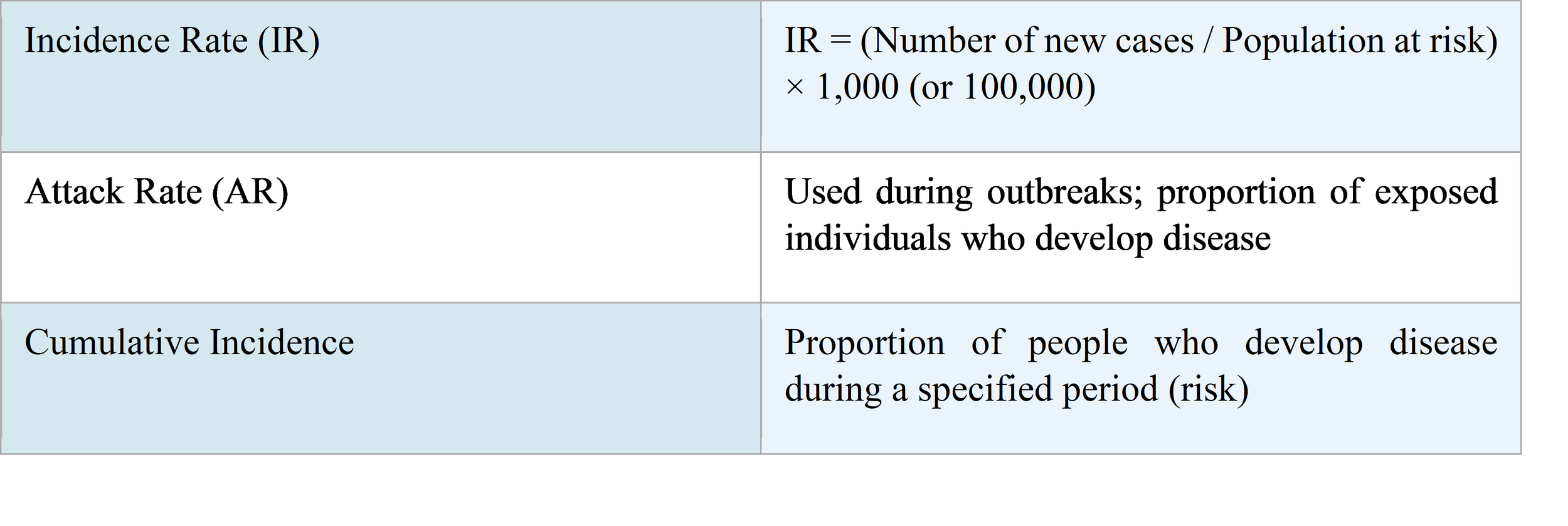
Example (NIH/NLM): The incidence rate of prostate cancer in the United States from 2015 to 2019 was 112.7 cases per 100,000 men per year, while the mortality rate for the same period was 18.9 per 100,000 per year. Reporting these separately provides a more complete picture of disease burden than either measure alone.
4.2 Prevalence
Prevalence measures the total number of existing cases (new and old) of a disease in a population at a specified point in time (point prevalence) or over a defined period (period prevalence). According to NIH StatPearls (updated 2023), prevalence increases when new cases are identified (via incidence) and decreases when patients are cured or die. Prevalence is essential for estimating the burden placed on healthcare systems and for resource planning.
The relationship between incidence and prevalence is expressed conceptually as: Prevalence ≈ Incidence Rate × Average Duration of Disease. An increase in cancer prevalence, for example, may reflect improving survival rather than increasing disease occurrence — a distinction with critical implications for healthcare planning.
4.3 Mortality Rates
Mortality rates quantify the frequency of death in a population. The crude mortality rate is the total number of deaths divided by the total population within a given time frame. Age-standardized mortality rates allow meaningful comparison across populations with different age structures. The case-fatality rate (CFR) — the proportion of diagnosed cases that result in death — measures disease lethality and is particularly important during epidemics and outbreak investigations.
Formula: Mortality Rate = (Total deaths during a given time interval) / (Total population) × 1,000 (or 100,000).
4.4 Disability-Adjusted Life Years (DALYs)
DALYs represent the standard metric used by WHO and the Global Burden of Disease Study to measure combined mortality and morbidity. One DALY represents one year of healthy life lost due to premature death or to living with disability from disease or injury. According to GBD 2021 data, NCDs accounted for 1.73 billion DALYs in 2021, representing 59.9% of the global total. This metric is crucial for health systems planning, international comparisons, and priority-setting.
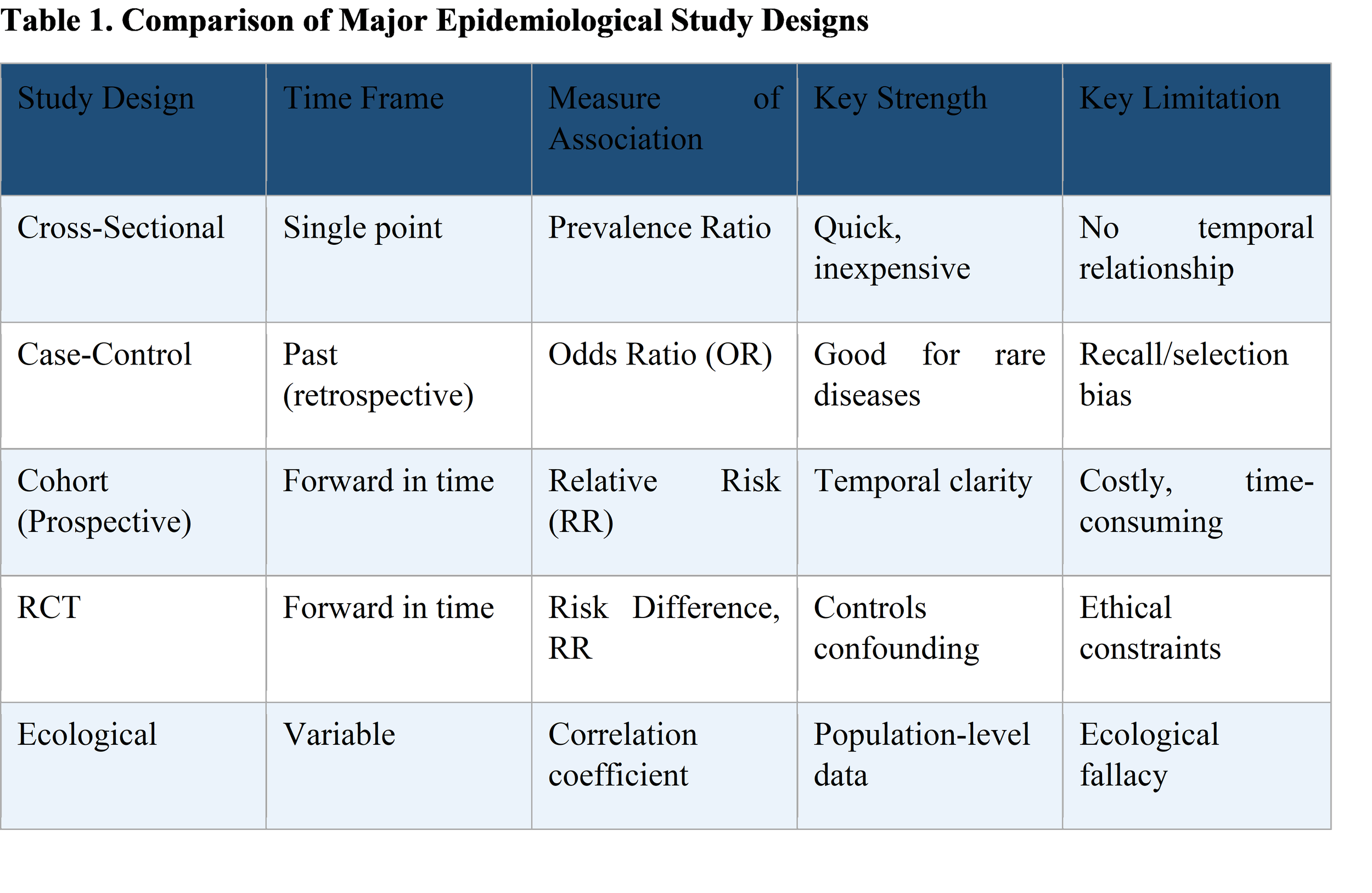
5. Epidemiological Study Designs
The validity and utility of epidemiological evidence depend critically on the choice of study design. As stated in a 2024 PubMed-indexed review published in the Journal of Clinical Medicine (Pérez-Guerrero et al., J Clin Med. 2024;13(14):4005; PMID: 39064045), epidemiological studies are essential in medicine and public health as they help identify risk factors and causes of diseases, and are key to planning, implementing, and evaluating health interventions aimed at preventing and controlling the spread of diseases.
Epidemiological studies are broadly classified as observational or experimental.
5.1 Descriptive Epidemiology
Descriptive studies characterize the occurrence of diseases and enable the determination of prevalence, incidence, and temporal patterns without making comparisons between groups to infer causality. They describe the distribution of disease by person, place, and time and generate hypotheses to be tested in analytical studies. Descriptive studies include case reports, case series, and cross-sectional surveys.
5.2 Analytical Observational Studies
5.2.1 Cross-Sectional Studies
Cross-sectional studies assess the prevalence of an outcome or exposure at a single point in time, providing a snapshot of a population's health status. They are efficient and cost-effective but are limited by their inability to establish causality due to the lack of temporal information (Setia, 2016). They are valuable for informing public health policies and resource allocation. A cross-sectional survey might, for example, determine the prevalence of tobacco use and its association with hypertension in an urban population.
5.2.2 Case-Control Studies
Case-control studies compare the exposure history of individuals who have developed a specific disease (cases) with those who have not (controls). They are particularly well-suited to the investigation of rare diseases and produce an odds ratio (OR) as the primary measure of association. A classic example is investigating risk factors for lung cancer by comparing the smoking history of lung cancer patients to that of healthy controls. Case-control studies are relatively inexpensive and efficient but are susceptible to recall bias and selection bias.
5.2.3 Cohort Studies
Cohort studies follow a defined group of individuals — initially free of the disease of interest — over time to observe who develops the outcome. They can be prospective (following subjects forward in time from exposure to outcome) or retrospective (reconstructing past exposure from historical records). Cohort studies provide incidence data and relative risks (RR). They are the design of choice when investigating the effects of uncommon exposures and when temporal relationships are critical. The landmark Framingham Heart Study exemplifies this design. Their main limitations are cost, time, and potential for loss to follow-up.
5.2.4 Ecological Studies
Ecological studies examine associations between exposures and outcomes at the population or group level rather than the individual level. They are useful for generating hypotheses and are often used when individual-level data are unavailable. However, the ecological fallacy — the erroneous inference that associations observed at the group level apply to individuals — limits causal inference.
5.3 Experimental Studies
5.3.1 Randomized Controlled Trials (RCTs)
The randomized controlled trial is considered the gold standard for evaluating the efficacy of interventions. Participants are randomly allocated to receive either the intervention or a control (placebo or standard care), and outcomes are compared. Randomization minimizes confounding by ensuring that known and unknown confounders are distributed equally across groups. RCTs provide the strongest evidence for causation but raise ethical concerns when withholding potentially beneficial treatments.
5.3.2 Field Trials and Community Trials
Field trials are conducted on disease-free individuals in natural settings to assess preventive interventions (e.g., vaccine trials). Community trials randomize entire communities rather than individuals. The 1954 Salk poliomyelitis vaccine trial — one of the largest field trials ever conducted — enrolled approximately 1.8 million children and demonstrated the vaccine's efficacy, ultimately leading to the near-elimination of polio globally.
6. Measures of Association
Analytical epidemiology employs statistical measures to quantify the relationship between exposures and health outcomes. According to a PubMed-indexed publication on measurement in epidemiology (PMID: 28188717), the three principal groups of measures are: frequency measures, association measures, and potential impact measures.
6.1 Relative Risk (RR) / Risk Ratio
The relative risk compares the incidence of disease in an exposed group to the incidence in an unexposed group. An RR of 1.0 indicates no association; an RR greater than 1.0 indicates increased risk in the exposed group; an RR less than 1.0 suggests a protective effect. RR is the preferred measure in cohort studies and RCTs.
Formula: RR = (Incidence in exposed group) / (Incidence in unexposed group).
6.2 Odds Ratio (OR)
The odds ratio compares the odds of exposure in cases to the odds of exposure in controls. It is the standard measure of association in case-control studies. When disease prevalence is low (under 10%), the OR approximates the RR and may be interpreted similarly. The OR is also the effect measure produced by logistic regression, the most widely used analytical method in epidemiological research.
6.3 Attributable Risk and Population-Attributable Risk
Attributable risk (risk difference) measures the absolute excess risk in the exposed group compared to the unexposed group. Population-attributable risk (PAR) estimates the proportion of disease in the entire population that is attributable to a given exposure — a crucial measure for prioritizing public health interventions. For example, if heavy smoking confers a 20-fold increased risk of lung cancer (as documented in the Framingham Heart Study), the PAR for smoking in a high-prevalence society would be substantial.
7. Causation in Epidemiology
Establishing causality — rather than mere association — is one of the most important and challenging tasks in epidemiology. The mere observation that two variables are statistically associated does not prove that one causes the other. Associations can arise from chance, bias, confounding, or genuine causality.
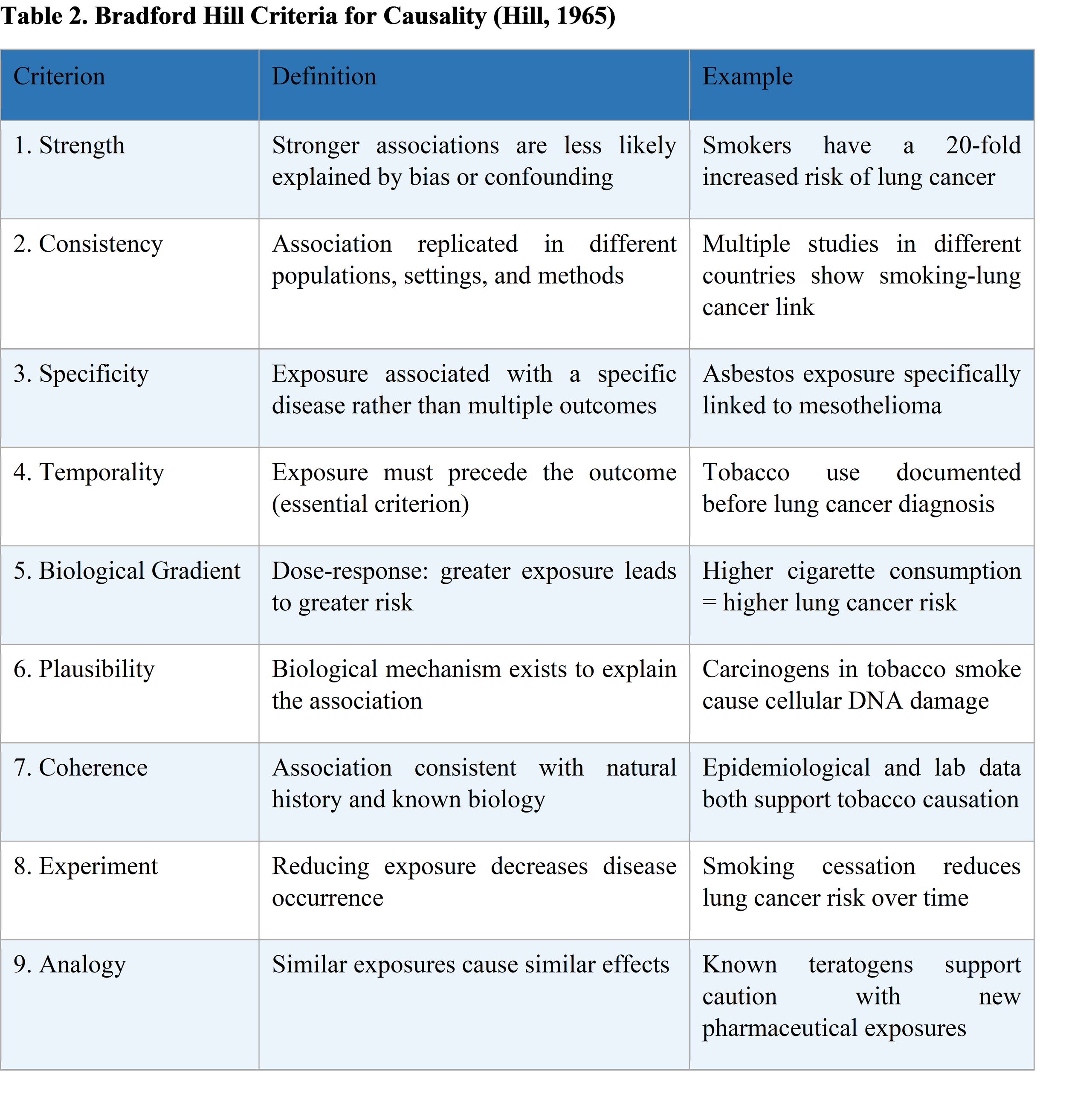
7.1 The Bradford Hill Criteria
In 1965, Sir Austin Bradford Hill proposed nine criteria to help evaluate whether an observed association between an exposure and a disease is likely to be causal. These criteria, originally developed from evidence linking tobacco smoking to lung cancer, remain the cornerstone of causal inference in epidemiological research and are cited by the EPA, CDC, and FDA in regulatory and public health contexts (JoVE Science Education, 2025; PMID: 44-1).
It is important to note that these nine criteria are not a definitive checklist; no single criterion is either necessary or sufficient for establishing causation. Temporality is the only criterion that is considered indispensable — the cause must always precede the effect. Evidence must be evaluated collectively, in light of the totality of available data. A 2021 PMC-indexed systematic review (PMC8206235) emphasizes that Bradford Hill criteria should be applied alongside modern tools such as directed acyclic graphs (DAGs) to control for confounding.
8. Bias and Confounding
Two of the most significant threats to the internal validity of epidemiological studies are bias and confounding. Understanding and controlling for these sources of error is essential for the correct interpretation of study findings.
8.1 Bias
Bias is any systematic error in the design, conduct, or analysis of a study that produces results that consistently deviate from the true value. Unlike random error, bias is directional and cannot be corrected by increasing sample size. Three major types of bias are recognized:
Selection Bias: Arises when study participants are not representative of the target population. Volunteer bias — where people who enroll in studies tend to be healthier than non-participants — is a well-documented example.
Information Bias: Occurs when data on exposure or outcome are inaccurately measured. Recall bias — where individuals with a disease (cases) remember past exposures differently from healthy controls — is particularly common in retrospective case-control studies.
Reporting Bias: Results from selective reporting of outcomes or exposures, including publication bias (the tendency for positive results to be published more than null findings).
8.2 Confounding
Confounding occurs when the relationship between an exposure and an outcome is distorted by a third variable (the confounder) that is associated with both the exposure and the outcome but is not on the causal pathway. For example, the apparent association between coffee drinking and cardiovascular disease may be confounded by cigarette smoking if smokers drink more coffee. Confounders may be controlled at the design stage (through restriction, matching, or randomization) or at the analysis stage (through stratification or multivariable regression).
The 2024 PubMed-indexed review (Pérez-Guerrero et al., PMID: 39064045) highlights that errors in the selection of methodological design and statistical tests are common in epidemiological observational studies and provides recommendations to improve accuracy and validity in cross-sectional, case-control, and cohort studies.
9. Public Health Surveillance
Epidemiology provides the foundation for public health surveillance — the systematic monitoring of the health status of populations. As defined by the WHO Western Pacific Regional Office, public health surveillance is "the continuous, systematic collection, analysis and interpretation of health-related data for action." Surveillance data serve as the basis for early detection of outbreaks, monitoring of disease trends, evaluation of interventions, and policy formulation.
9.1 Purpose and Functions of Surveillance
Early warning: Detection of potential outbreaks before they become public health emergencies.
Disease burden estimation: Tracking incidence, prevalence, and mortality trends across populations.
Programme evaluation: Monitoring the impact of vaccination campaigns, screening programmes, and health interventions.
Policy development: Providing the evidence base for public health decisions and resource allocation.
Epidemiology clarification: Clarifying risk factors, high-risk populations, and geographic patterns of disease.
9.2 Types of Surveillance
Passive surveillance relies on routine reporting by healthcare providers and laboratories to public health authorities. Active surveillance involves public health officials directly collecting data from providers and is more sensitive but resource-intensive. Sentinel surveillance uses a selected network of reporting sites to monitor disease trends. Syndromic surveillance tracks clinical syndromes or indicators (e.g., influenza-like illness) rather than confirmed diagnoses, enabling earlier detection of outbreaks.
9.3 Surveillance in Humanitarian Settings
The WHO emphasizes that humanitarian emergencies increase the risk of transmission of infectious diseases and other health conditions, such as severe malnutrition. Effective disease surveillance systems are essential for detecting disease outbreaks quickly in emergency settings. The WHO African Regional Office's transition from Epi Info to DHIS2 (District Health Information Software 2) for vaccine-preventable disease surveillance (2019–2024) exemplifies ongoing efforts to strengthen surveillance infrastructure in resource-limited settings (MMWR, 2024;73(23)).
10. The Global Burden of Disease and Epidemiological Transition
The epidemiological transition — first theorized by Abdel Omran in 1971 — describes the shift in mortality patterns from infectious and parasitic diseases to chronic noncommunicable diseases as populations develop economically and demographically. This transition is characterized by falling death rates, increasing life expectancy, and a rising burden of NCDs.
10.1 The Contemporary NCD Crisis
According to the WHO (2024 Fact Sheet), noncommunicable diseases kill more than 40 million people each year. Specifically, NCDs killed at least 43 million people in 2021, equivalent to 75% of all non-pandemic-related deaths globally. A 2025 PubMed-indexed systematic analysis (Freihat et al., PLoS ONE, DOI:10.1371/journal.pone.0336036) using GBD 2021 data reported the following:
NCDs accounted for 12.4 billion incident cases in 2021 (rate: 156,680 per 100,000).
NCDs caused 43.8 million deaths (64.5% of total deaths) with an age-standardized rate of 554.63 per 100,000.
NCDs generated 1.73 billion DALYs (59.9% of total), at a rate of 21,887 per 100,000.
Cardiovascular diseases led with 19.4 million deaths (28.6% of total), followed by neoplasms (9.9 million, 14.6%) and chronic respiratory diseases (4.4 million).
10.2 Leading Causes of NCD Mortality
Based on GBD 2021 data, cardiovascular diseases account for approximately one-half of all NCD deaths, and the majority of these deaths occur in low- and middle-income countries (LMIC). Diabetes and chronic kidney disease represent some of the fastest-growing NCDs, with diabetes and kidney disease showing a 49.4% increase in incidence in the Eastern Mediterranean region. Substance use disorders have exhibited a 138% increase in mortality rates among women in the Americas.
10.3 Communicable Diseases and Dual Burden
While NCDs dominate the global disease burden in high-income countries, many LMICs face a dual burden of communicable and noncommunicable diseases — often referred to as a protracted epidemiological transition. HIV/AIDS, tuberculosis, malaria, and vaccine-preventable diseases continue to claim millions of lives, particularly in sub-Saharan Africa and South Asia. This epidemiological complexity demands integrated surveillance and healthcare delivery systems capable of addressing both acute infectious conditions and chronic diseases simultaneously.
11. Outbreak Investigation
One of the most operationally significant applications of epidemiology is the investigation of disease outbreaks. The CDC defines an outbreak (or epidemic) as the occurrence of more cases of disease than would be expected in a given area or among a specific group of people over a particular period of time. In some instances — particularly for rare diseases with high public health impact, such as botulism — even a single case may constitute an outbreak.
11.1 Steps in Outbreak Investigation
The CDC's field epidemiology guidelines describe a systematic step-by-step approach to outbreak investigation, which includes:
Prepare for field work: Confirm the outbreak and assemble the investigation team.
Establish case definitions: Define cases by clinical criteria, time, place, and person characteristics.
Find cases systematically: Conduct active case-finding to identify all affected individuals.
Describe and orient data (person, place, time): Construct epidemic curves, spot maps, and attack rate tables.
Develop hypotheses: Based on descriptive data, generate hypotheses about the source and mode of transmission.
Evaluate hypotheses analytically: Test hypotheses using case-control or cohort study designs.
Implement control and prevention measures: Apply control measures based on findings and may not await study completion.
Communicate findings: Report results to public health authorities, healthcare providers, and the public.
Epidemiological concepts — including attack rates, epidemic curves, incubation periods, and reproductive numbers (R0) — are indispensable tools in outbreak investigation. The COVID-19 pandemic (2020–2023) demonstrated on a global scale both the power of epidemiological methods (contact tracing, R0 estimation, vaccine effectiveness studies) and the catastrophic consequences when epidemiological intelligence is delayed or misapplied.
12. Ethics in Epidemiological Research
Epidemiological research involves human subjects and generates data with profound policy implications. Accordingly, ethical principles govern its conduct. The core ethical principles in epidemiology — derived from broader bioethical frameworks — include respect for persons (autonomy and informed consent), beneficence (maximizing benefit), non-maleficence (avoiding harm), and justice (fair distribution of research burdens and benefits).
Key ethical considerations in epidemiology include: protecting the privacy and confidentiality of participants; ensuring that research benefits are not restricted to high-income populations; balancing individual interests with the public good; and addressing conflicts of interest, particularly in industry-funded research. The ethics of public health surveillance — where individual data may be collected without explicit consent in the interest of population protection — requires particularly careful consideration of the public health justification and proportionality of data collection.
13. Future Directions in Epidemiology
The field of epidemiology is evolving rapidly in response to technological advances, the complexity of contemporary health challenges, and the globalization of disease. Several emerging areas merit particular attention:
Molecular and Genetic Epidemiology: The integration of genomics, epigenomics, and microbiomics into epidemiological studies is enabling the identification of genetic determinants of disease susceptibility and the mechanisms linking environmental exposures to health outcomes.
Digital Epidemiology and Big Data: The availability of electronic health records, mobile health data, social media, and real-time surveillance platforms is expanding the scope and speed of epidemiological analysis. Machine learning algorithms are increasingly applied to identify disease patterns and risk factors from large datasets.
Climate Change and Planetary Health Epidemiology: Climate change is altering the distribution and intensity of infectious diseases (e.g., malaria, dengue, cholera) and increasing the frequency of heat-related illness and extreme weather events. Epidemiologists are at the forefront of quantifying and communicating these health risks.
One Health Epidemiology: Recognizing that human, animal, and environmental health are interconnected, the One Health framework integrates epidemiological surveillance and research across these domains — critical for the prevention of zoonotic diseases, antimicrobial resistance, and food safety threats.
Equity and Social Epidemiology: Growing recognition of the social determinants of health — including poverty, racism, housing insecurity, and educational inequality — is driving an expansion of epidemiological methods to measure and address health disparities.
14. Conclusion
Epidemiology is, and will remain, the foundational science of public health. Its principles — the systematic quantification of disease frequency, the rigorous design of studies to identify causal determinants, the continuous surveillance of population health, and the application of evidence to public health action — are indispensable for confronting the health challenges of the 21st century.
The global burden of noncommunicable diseases — responsible for 43 million deaths and 1.73 billion DALYs in 2021 alone — as well as the persistent threat of communicable diseases, humanitarian emergencies, and emerging pandemics, demands an ever more sophisticated and equitable application of epidemiological science. From John Snow's cholera map to the genomic surveillance of SARS-CoV-2 variants, epidemiology has repeatedly demonstrated its capacity to protect human health through rigorous inquiry.
For students, researchers, clinicians, and policymakers alike, a thorough grounding in the basic principles and methods of epidemiology is not merely an academic exercise — it is a prerequisite for effective, evidence-based engagement with the most pressing health challenges facing humanity.
References
1. World Health Organization. (2006). Basic Epidemiology (2nd ed.). Bonita R, Beaglehole R, Kjellström T. WHO Press, Geneva. ISBN: 92-4-154707-3. https://www.who.int/publications/b/31231
2. Dicker R, Coronado F, Koo D, Parrish RG. (2012). Principles of Epidemiology in Public Health Practice: An Introduction to Applied Epidemiology and Biostatistics (3rd ed., Self-Study Course SS1978). Centers for Disease Control and Prevention. https://stacks.cdc.gov/view/cdc/6914
3. World Health Organization. (2024). Noncommunicable Diseases Fact Sheet. WHO, Geneva. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
4. GBD 2021 Causes of Death Collaborators. (2025). Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990–2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet. 406(10513):1811-1872. doi:10.1016/S0140-6736(24)02369-3.
5. Pérez-Guerrero EE, et al. (2024). Methodological and Statistical Considerations for Cross-Sectional, Case–Control, and Cohort Studies. J Clin Med. 13(14):4005. doi:10.3390/jcm13144005. PMID: 39064045. PMC: PMC11277135.
6. Freihat O, Sipos D, Aamir M, et al. (2025). Global burden and future projections of non-communicable diseases (2000–2050): Progress toward SDG 3.4 and disparities across regions and risk factors. PLoS ONE. doi:10.1371/journal.pone.0336036.
7. National Library of Medicine (NIH). (2022). Finding and Using Health Statistics: Incidence Rate. NLM, Bethesda, MD. https://www.nlm.nih.gov/oet/ed/stats/01-200.html
8. Merkin SS. (2023). Prevalence. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. NCBI Bookshelf NBK430867. https://www.ncbi.nlm.nih.gov/books/NBK430867/
9. Hill AB. (1965). The Environment and Disease: Association or Causation? Proc R Soc Med. 58(5):295–300. PMID: 14283879.
10. Hammoud MZ, et al. (2021). Assessing causality in epidemiology: revisiting Bradford Hill to incorporate developments in causal thinking. Eur J Epidemiol. 36:873–887. doi:10.1007/s10654-020-00703-7. PMC8206235.
11. World Health Organization Western Pacific Regional Office. (2023). Disease Surveillance. WHO WPRO. https://www.who.int/westernpacific/emergencies/surveillance
12. Adegoke OJ, et al. (2024). Migration from Epi Info to District Health Information Software 2 for Vaccine-Preventable Disease Surveillance — WHO African Region, 2019–2023. MMWR Morb Mortal Wkly Rep. 73(23). doi:10.15585/mmwr.mm7323a2. PMC11199014.
13. CDC. (2012). Principles of Epidemiology: Lesson 3 — Measures of Risk. SS1978 Self-Study Course. Atlanta: CDC. https://archive.cdc.gov/www_cdc_gov/csels/dsepd/ss1978/lesson3/index.html
14. Belbasis L, Bellou V. (2018). Introduction to Epidemiological Studies. Methods Mol Biol. 1793:1-6. doi:10.1007/978-1-4939-7868-7_1. PMID: 29876887.
15. Pan American Health Organization / WHO. (2025). The Burden of Noncommunicable Diseases in the Region of the Americas, 2000–2021. ENLACE Data Portal. Washington, D.C.: PAHO. https://www.paho.org/en/enlace/burden-noncommunicable-diseases
16. Omran AR. (2005). The epidemiologic transition: A theory of the epidemiology of population change. Milbank Q. 83(4):731–757. doi:10.1111/j.1468-0009.2005.00398.x. PMC2690264.
17. Putter RJ, et al. (2015). A new relation between prevalence and incidence of a chronic disease. Math Biosci. 270(Pt A):113-7. doi:10.1016/j.mbs.2015.10.003. PMC4684690.