
Methodical Recommendations, Standards for Diagnosis and Treatment of Acute Clinical Forms of Coronary Heart Disease: Angina Pectoris, Myocardial Infarction
1. Eswaramoorthy Vignesh
Evansan Jeffrey
2. Abdilazizova Asema
(1. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
Coronary heart disease (CHD) remains the leading single cause of death worldwide, accounting for over 9 million fatalities annually. The acute clinical forms of CHD - encompassing stable and unstable angina pectoris and the full spectrum of acute myocardial infarction (AMI) - are defined by a continuum of myocardial ischaemia ranging from reversible oxygen supply-demand mismatch to irreversible cardiomyocyte necrosis. Timely, accurate diagnosis and evidence-based treatment are paramount, as each hour of untreated coronary occlusion results in the irreversible loss of approximately one billion cardiomyocytes. This review provides comprehensive methodical recommendations and contemporary clinical standards, aligned with the 2023 European Society of Cardiology (ESC) Guidelines on Acute Coronary Syndromes and the 2021 ACC/AHA Guideline for Coronary Artery Disease, for the classification, diagnostic workup, risk stratification, and pharmacological and interventional management of angina pectoris and myocardial infarction.
Special emphasis is placed on the electrocardiographic and biomarker-based diagnostic algorithm, the GRACE and TIMI risk scores, and the time-to-treatment standards for ST-elevation myocardial infarction (STEMI) and non-ST-elevation acute coronary syndrome (NSTE-ACS).
Keywords: Coronary Heart Disease, Angina Pectoris, Myocardial Infarction, Acute Coronary Syndrome, STEMI, NSTE-ACS, Percutaneous Coronary Intervention, ESC Guidelines, GRACE Score, Reperfusion Therapy.
1. Introduction
Coronary heart disease (CHD), also termed ischaemic heart disease (IHD), encompasses a spectrum of clinical syndromes caused by myocardial ischaemia - an imbalance between myocardial oxygen supply and demand - most commonly arising from atherosclerotic narrowing or acute thrombotic occlusion of the coronary arteries. The Global Burden of Disease Study 2019 estimated that CHD affects over 197 million individuals worldwide and is responsible for approximately 9.14 million deaths annually, representing 16.2% of all global mortality [1].
The clinical manifestations of CHD range from the stable, predictable exertional chest pain of chronic stable angina to the life-threatening emergency of acute myocardial infarction (AMI) with cardiogenic shock or malignant arrhythmia. Between these poles lies the pivotal entity of unstable angina - which, together with non-ST-elevation myocardial infarction (NSTEMI), constitutes the non-ST-elevation acute coronary syndrome (NSTE-ACS) - representing a myocardial ischaemic emergency demanding urgent evaluation and risk-stratified management [2]. At the most acute and time-critical end of the spectrum, ST-elevation myocardial infarction (STEMI) demands immediate coronary reperfusion, with evidence-based standards mandating a door-to-balloon time of less than or equal to 90 minutes for primary percutaneous coronary intervention (PCI) or, where PCI is unavailable, fibrinolysis within 10 minutes of ECG diagnosis [3].
The clinical standards governing diagnosis and treatment of these conditions have been transformed by landmark randomised controlled trials - including GUSTO, PLATO, TRITON-TIMI, CURE, HORIZONS-AMI, and ISCHEMIA - which have progressively refined reperfusion strategies, antithrombotic regimens, and risk stratification tools. This article synthesises these standards into methodical recommendations for the practicing clinician.
2. Pathophysiology of Acute Coronary Syndromes
2.1 Atherosclerosis: The Substrate of Coronary Heart Disease
The pathological foundation of CHD is atherosclerosis - a chronic, progressive inflammatory disease of the arterial intima characterised by the accumulation of lipid-laden foam cells, smooth muscle cell proliferation, and extracellular matrix deposition beneath the endothelium. The process begins with endothelial dysfunction triggered by cardiovascular risk factors - including hypertension, dyslipidaemia, diabetes mellitus, tobacco use, and advancing age - which promotes the oxidation of low-density lipoprotein (LDL-C) particles and their subendothelial retention [4].
Oxidised LDL stimulates monocyte recruitment and transformation into macrophage-derived foam cells, forming the fatty streak - the earliest visible atherosclerotic lesion. Over decades, the evolving plaque acquires a fibrous cap, a necrotic lipid core, and inflammatory infiltrates, ultimately developing into a flow-limiting stenosis or a vulnerable plaque susceptible to rupture [1, 4].
2.2 Plaque Rupture and Coronary Thrombosis
The transition from stable to acute CHD is precipitated by plaque disruption - either rupture of the fibrous cap or superficial plaque erosion - which exposes the thrombogenic lipid core and subendothelial collagen to circulating platelets and coagulation factors. Platelet adhesion (mediated by GPIb-von Willebrand factor interaction), activation, and aggregation (mediated by GPIIb/IIIa receptor cross-linking with fibrinogen) rapidly generate a platelet-rich white thrombus.
Simultaneous activation of the coagulation cascade produces a fibrin-rich red thrombus, culminating in partial or complete coronary occlusion [2, 5].
The degree of occlusion and its haemodynamic consequences determine the clinical syndrome: a non-occlusive thrombus with preserved but impaired coronary flow produces the ischaemia of NSTE-ACS (unstable angina or NSTEMI), while complete thrombotic occlusion with transmural ischaemia produces STEMI. Coronary vasospasm (Prinzmetal angina) and spontaneous coronary artery dissection (SCAD) represent alternative mechanisms of ACS not primarily driven by plaque rupture [2].
3. Classification and Diagnostic Standards
3.1 Classification of Acute Coronary Syndromes
The contemporary classification of ACS is grounded in the electrocardiographic and biomarker findings at presentation [2, 3]:
ST-Elevation Myocardial Infarction (STEMI): Complete thrombotic occlusion with new ST elevation in 2 or more contiguous leads (greater than or equal to 1 mm in limb leads; greater than or equal to 2 mm in V2-V3). Immediate reperfusion is mandatory.
Non-ST-Elevation Myocardial Infarction (NSTEMI): Partial coronary occlusion producing subendocardial ischaemia with cardiomyocyte necrosis. High-sensitivity cardiac troponin (hs-cTn) is elevated above the 99th percentile.
Unstable Angina (UA): Ischaemia without myocardial necrosis. New-onset severe angina, rest angina greater than 20 minutes, or crescendo angina. hs-cTn is normal.
Stable Angina Pectoris: Predictable, reproducible exertional chest pain caused by fixed coronary stenosis. Relieved by rest or nitrates within 5 minutes.
Variant Angina (Prinzmetal): Resting angina caused by coronary vasospasm producing transient ST elevation. Associated with near-normal coronary arteries.
3.2 Electrocardiography: The Mandatory First Investigation
A 12-lead ECG must be obtained and interpreted within 10 minutes of first medical contact in all patients with suspected ACS - a Class I, Level B recommendation [2, 3]. The ECG serves as the primary triage tool separating STEMI (requiring immediate reperfusion) from NSTE-ACS (requiring risk stratification). Key ECG findings include:
ST elevation: New ST elevation at the J-point in 2 or more contiguous leads indicates STEMI. New Left Bundle Branch Block (LBBB) with ischaemic symptoms is treated as STEMI equivalent.
ST depression and T-wave changes: Horizontal or down-sloping ST depression greater than or equal to 0.5 mm in 2 or more contiguous leads indicates NSTEMI/UA. Symmetrical T-wave inversion greater than or equal to 2 mm in V1-V4 suggests Wellens syndrome (critical proximal LAD stenosis).
Serial ECG recording: Repeat ECG at 15-30 minute intervals is recommended if the initial ECG is non-diagnostic in patients with high clinical suspicion.
3.3 High-Sensitivity Cardiac Troponin (hs-cTn): Biomarker Standards
High-sensitivity cardiac troponin I or T is the biomarker of choice for myocardial infarction diagnosis. The 2023 ESC ACS Guidelines mandate hs-cTn measurement at presentation (0 h) and at 1-3 hours using validated rapid rule-in/rule-out algorithms [2]. The ESC 0h/1h algorithm (RAPID protocol) classifies patients into three groups based on hs-cTn concentration and change:
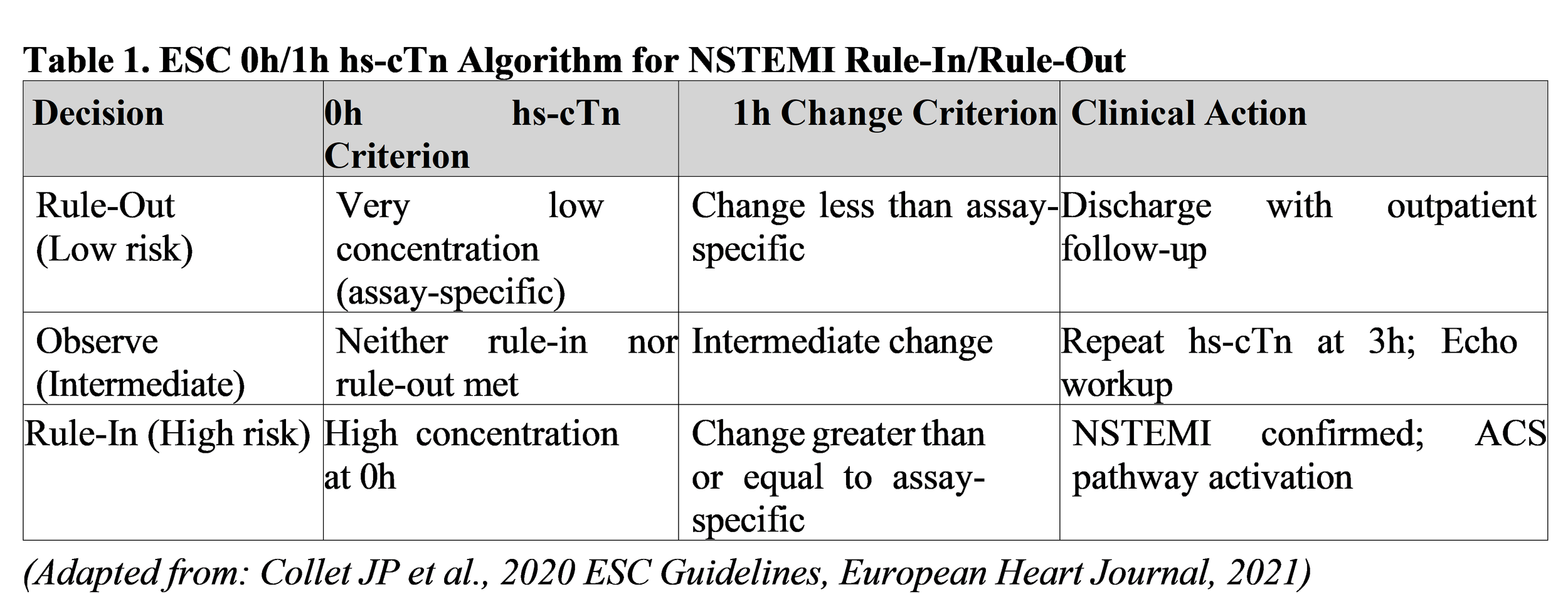
The universal definition of myocardial infarction (Fourth Universal Definition, 2018) requires detection of a rise and/or fall of cardiac troponin values with at least one value above the 99th percentile URL, in the context of ischaemic symptoms, new ischaemic ECG changes, imaging evidence of new wall motion abnormality, or identification of a coronary thrombus [7].
4. Risk Stratification in Acute Coronary Syndromes
4.1 GRACE Score
The GRACE Score (Global Registry of Acute Coronary Events) calculates predicted in-hospital and 6-month mortality risk based on eight variables: age, heart rate, systolic blood pressure, serum creatinine, Killip class, ST deviation, cardiac arrest at admission, and elevated cardiac biomarkers. The ESC guidelines recommend GRACE score (Class I, Level B) to guide invasive strategy timing in NSTE-ACS: Very High risk (less than or equal to 2h), High risk (less than or equal to 24h), Low- Intermediate risk (less than or equal to 72h) [2].
4.2 TIMI Risk Score
The TIMI Risk Score for UA/NSTEMI comprises seven variables (age greater than or equal to 65, 3 or more CAD risk factors, prior coronary stenosis greater than or equal to 50%, ST deviation, 2 or more anginal events in 24 h, aspirin use in past 7 days, elevated serum cardiac markers); score greater than or equal to 3 identifies patients at increased risk of 14-day adverse events [6].
5. Management of Stable Angina Pectoris
5.1 Anti-Ischaemic Pharmacotherapy
The pharmacological management of stable angina targets both symptomatic relief and secondary cardiovascular prevention. Evidence-based first-line anti-ischaemic agents are [1, 6]:
Beta-blockers (Class I, Level A): First-line agents reducing heart rate and myocardial oxygen demand. Preferred agents: Metoprolol succinate 25-200 mg/day, Bisoprolol 2.5-10 mg/day. Target resting heart rate: 55-60 bpm.
Calcium Channel Blockers (Class I, Level A): Amlodipine 5-10 mg/day for non- dihydropyridines. First-line for Prinzmetal variant angina.
Long-acting Nitrates (Class IIa, Level B): Isosorbide mononitrate 30-120 mg/day. Sublingual GTN 0.4 mg is standard for acute relief.
5.2 Secondary Prevention
All patients with confirmed CHD require lifelong secondary prevention: Aspirin 75-100 mg/day; High-intensity statin (Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg) targeting LDL-C less than
1.4 mmol/L with greater than or equal to 50% reduction from baseline; ACE inhibitors or ARBs for patients with LVEF less than or equal to 40%, hypertension, diabetes, or CKD [1, 3].
6. Management of ST-Elevation Myocardial Infarction (STEMI)
6.1 Time-to-Treatment Standards
The ESC 2017 STEMI Guidelines specify binding time-to-treatment benchmarks, as each 30- minute delay in reperfusion is associated with a 7.5% increase in 30-day mortality [3, 8]:
First Medical Contact (FMC) to ECG diagnosis: less than or equal to 10 minutes.
FMC to primary PCI (balloon inflation): less than or equal to 90 minutes. The gold standard benchmark for PCI-capable systems.
FMC to fibrinolysis: less than or equal to 10 minutes after STEMI diagnosis, when PCI unavailable within 120 minutes.
6.2 Primary Percutaneous Coronary Intervention (Primary PCI)
Primary PCI is the recommended reperfusion strategy for all STEMI patients presenting within 12 hours (Class I, Level A). The procedural standard includes: radial artery access as preferred approach (Class I, Level A); drug-eluting stent (DES) implantation over bare-metal stents (Class I, Level A); and complete revascularisation in haemodynamically stable patients with multivessel disease (Class IIa, Level A) [3].
6.3 Fibrinolytic Therapy
When primary PCI cannot be performed within 120 minutes of STEMI diagnosis, fibrinolytic therapy should be initiated within 10 minutes of ECG diagnosis (Class I, Level A). Fibrin-specific agents are preferred: Tenecteplase (weight-based single IV bolus), Alteplase (15 mg bolus plus 0.75 mg/kg over 30 min plus 0.5 mg/kg over 60 min), or Reteplase (10 U plus 10 U IV bolus 30 minutes apart) [3, 8]. After successful fibrinolysis, coronary angiography is mandated within 3-24 hours. Failed fibrinolysis (less than 50% ST resolution at 60-90 minutes) requires immediate rescue PCI.
6.4 Antithrombotic Therapy in STEMI
Dual antiplatelet therapy (DAPT) must be initiated as early as possible. Aspirin 150-300 mg loading dose followed by 75-100 mg/day is combined with a P2Y12 inhibitor: Ticagrelor 180 mg loading dose (90 mg twice daily) or Prasugrel 60 mg loading dose (10 mg/day) are preferred over Clopidogrel [2, 9]. DAPT duration: 12 months post-STEMI. Anticoagulation during primary PCI: unfractionated heparin (UFH) 70-80 U/kg IV bolus or bivalirudin 0.75 mg/kg bolus plus 1.75 mg/kg/h infusion [3].
7. Management of Non-ST-Elevation ACS (NSTE-ACS)
7.1 Risk-Stratified Invasive Strategy Timing
The timing of invasive coronary angiography in NSTE-ACS is determined by GRACE risk score and clinical features [2]:
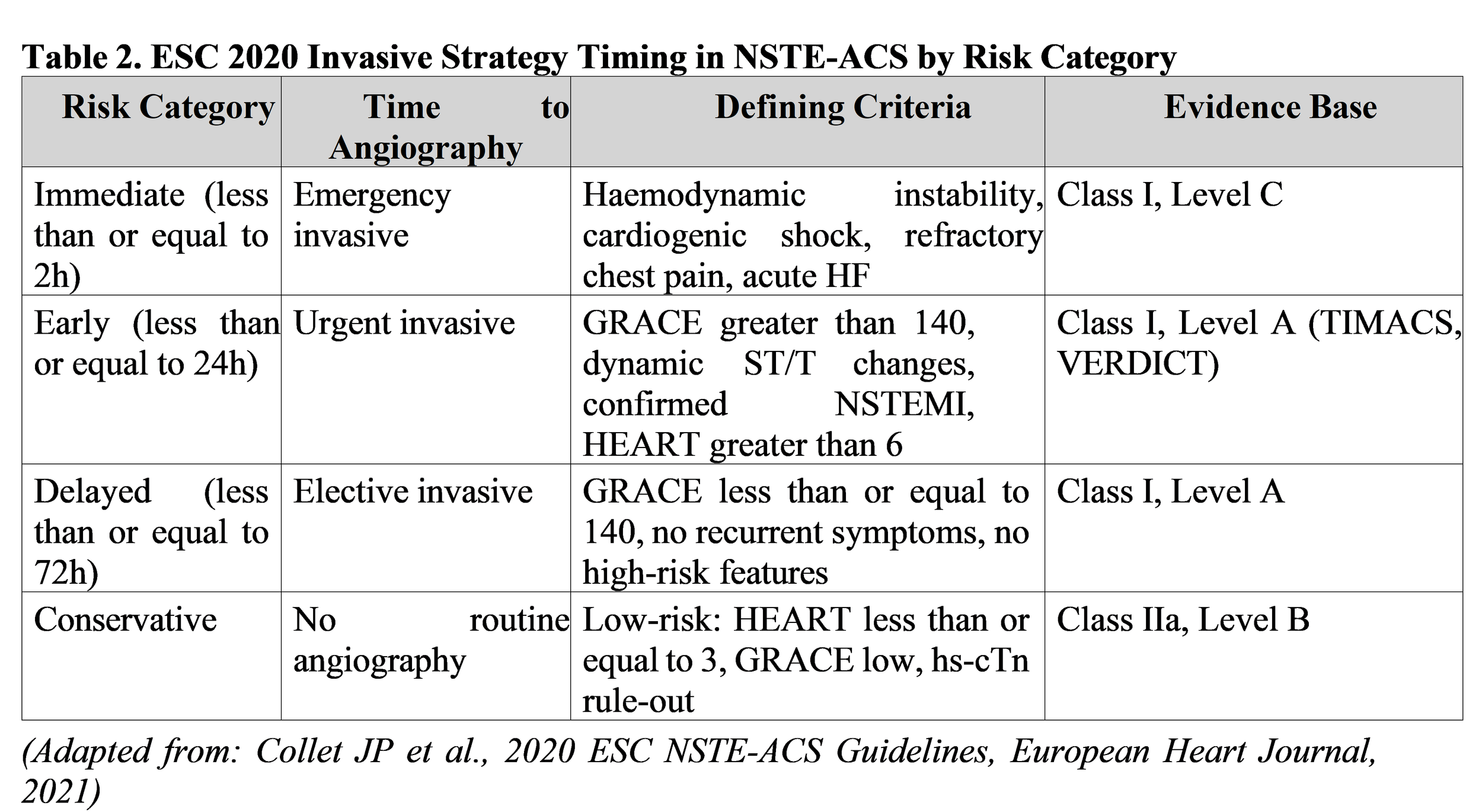
7.2 Antithrombotic Therapy in NSTE-ACS
Antiplatelet therapy in NSTE-ACS follows the same DAPT backbone as STEMI. Ticagrelor (180 mg loading dose, 90 mg twice daily) is preferred in NSTE-ACS managed invasively (Class I, Level B) based on PLATO trial data showing 16% relative risk reduction versus Clopidogrel [9]. Parenteral anticoagulation with fondaparinux (2.5 mg SC daily), enoxaparin (1 mg/kg SC twice daily), or UFH is recommended for all NSTE-ACS patients from diagnosis until revascularisation [2, 10].
8. Long-Term Post-MI Management and Complications
8.1 Acute Heart Failure and Cardiogenic Shock
Acute decompensated heart failure (ADHF) occurs in 10-20% of AMI patients. Cardiogenic shock, defined as sustained hypotension (SBP less than 90 mmHg for greater than 30 minutes) with signs of tissue hypoperfusion despite adequate filling pressure, carries in-hospital mortality exceeding 40- 50% [1, 2]. Immediate management priorities: (1) urgent coronary revascularisation by primary PCI (the SHOCK trial demonstrated 50% relative mortality reduction); (2) mechanical circulatory support (IABP, Impella, ECMO); and (3) inotropic support (dobutamine, low-dose epinephrine) [3].
8.2 Left Ventricular Thrombus (LVT)
Left ventricular thrombus forms in 2-5% of anterior MI (pre-reperfusion era: 5-15%). Risk factors: anterior MI, LVEF less than 40%, akinetic myocardium. Transthoracic echocardiography is the standard diagnostic modality. Management: anticoagulation with UFH, LMWH, or fondaparinux for minimum 3 months (Class I, Level B); warfarin (INR 2-3) or newer anticoagulants as alternatives [2, 3]. Systemic embolism risk is 10-20% without treatment, reduced to less than 2% with anticoagulation.
8.3 Post-MI Arrhythmias
Ventricular fibrillation (VF) and sustained ventricular tachycardia (VT) during acute STEMI (first 24-48 hours, primary VF/VT) are managed with immediate unsynchronised defibrillation (200 J biphasic shock). Intravenous amiodarone (150 mg bolus over 10 minutes, then 1 mg/min for 6 hours) is standard [1, 3]. Late VF/VT (greater than 48 hours post-MI) indicates reentrant substrate and warrants electrophysiology study and ICD implantation consideration [2, 3].
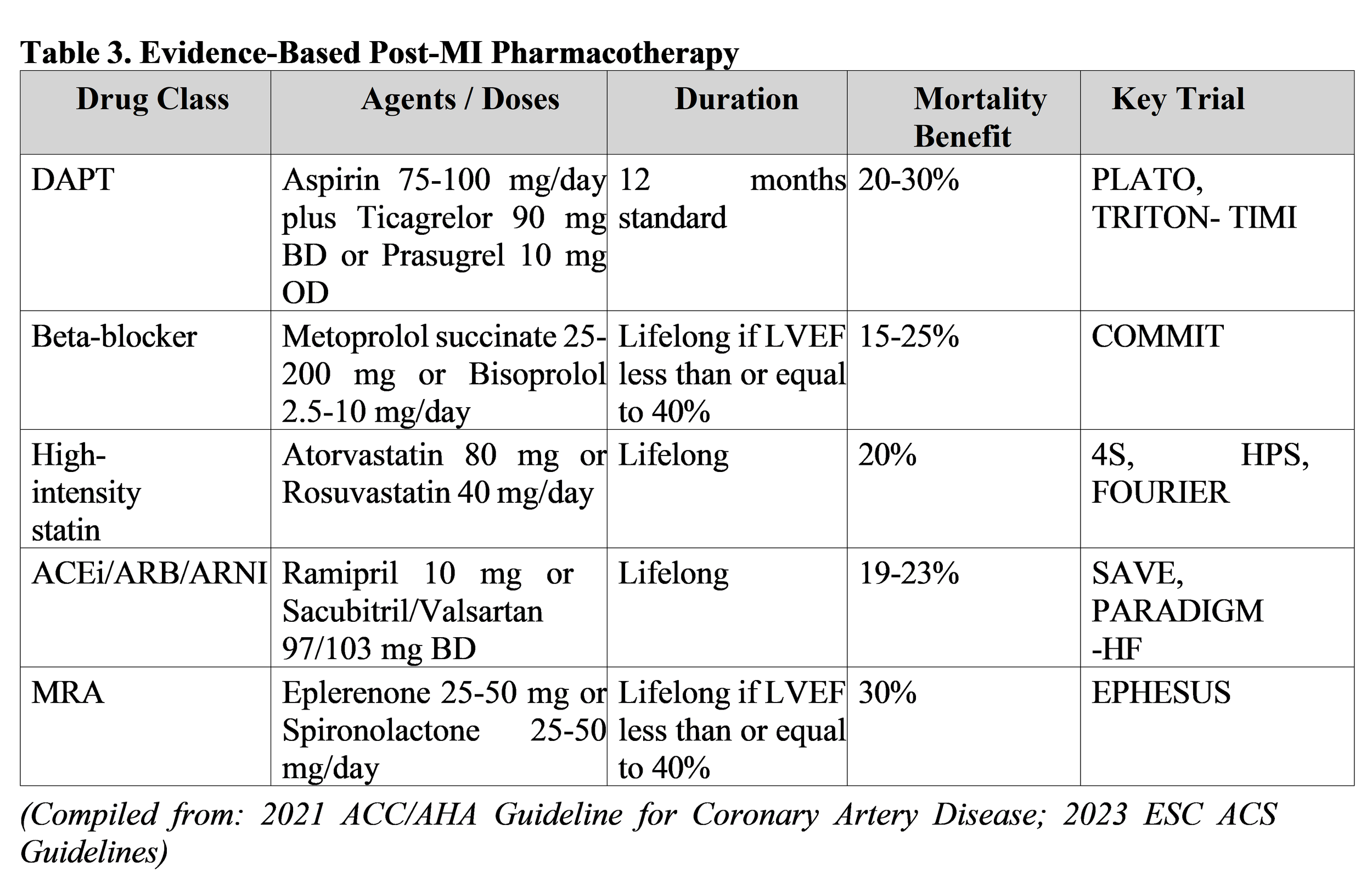
8.4 Secondary Prevention Pharmacotherapy
Post-MI pharmacotherapy includes six pillars (Class I recommendations): (1) DAPT (Aspirin plus Ticagrelor or Prasugrel) for 12 months; (2) beta-blockers lifelong if LVEF less than or equal to 40%; (3) high-intensity statins (Atorvastatin 80 mg or Rosuvastatin 40 mg); (4) ACE inhibitors (Ramipril 10 mg) or ARNI (Sacubitril/Valsartan); (5) mineralocorticoid receptor antagonists (Eplerenone or Spironolactone) if LVEF less than or equal to 40%; and (6) SGLT2 inhibitors (Dapagliflozin, Empagliflozin) if HFrEF or T2DM [1, 3]. The SAVE trial demonstrated 19% mortality reduction with ACEi [8]; EPHESUS trial demonstrated 30% mortality reduction with Eplerenone in post-MI HFrEF [9].
9. Conclusion
Angina pectoris and myocardial infarction represent the most consequential acute clinical manifestations of coronary heart disease, demanding rapid, systematic, and evidence-guided clinical action at every stage. The methodical recommendations presented in this review, grounded in the 2023 ESC ACS Guidelines and 2021 ACC/AHA Coronary Artery Disease Guideline, provide a comprehensive framework encompassing: structured chest pain assessment and ACS classification; mandatory 10-minute ECG acquisition and hs-cTn 0h/1h rule-in/rule-out algorithms; GRACE and TIMI risk stratification for timing of invasive strategy in NSTE-ACS; reperfusion time benchmarks of less than or equal to 90 minutes (primary PCI) and less than or equal to 10 minutes (fibrinolysis) for STEMI; evidence-based antithrombotic regimens incorporating Ticagrelor and Prasugrel; and lifelong six-pillar secondary prevention pharmacotherapy. Adherence to these standards, combined with systematic cardiac rehabilitation and long-term risk factor modification, offers the greatest opportunity to reduce the devastating global burden of coronary heart disease mortality and morbidity.
Disclosure of Funding Sources
The authors declare that no specific funding was received for the preparation of this review article. No granting agencies, institutional support, or non-material project frameworks contributed to this work.
10. References
[1] Knuuti, J., Wijns, W., Saraste, A., et al. (2020). 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal, 41(3), 407-477. https://doi.org/10.1093/eurheartj/ehz425
[2] Collet, J. P., Thiele, H., Barbato, E., et al. (2021). 2020 ESC Guidelines for the management of acute coronary syndromes without persistent ST-segment elevation. European Heart Journal, 42(14), 1289-1367. https://doi.org/10.1093/eurheartj/ehab232
[3] Ibanez, B., James, S., Agewall, S., et al. (2018). 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal, 39(2), 119-177. https://doi.org/10.1093/eurheartj/ehx393
[4] Libby, P., Ridker, P. M., and Hansson, G. K. (2011). Progress and challenges in translating the biology of atherosclerosis. Nature, 473(7347), 317-325. https://doi.org/10.1038/nature10146
[5] Fuster, V., Badimon, L., Badimon, J. J., and Chesebro, J. H. (1992). The pathogenesis of coronary artery disease and the acute coronary syndromes. New England Journal of Medicine, 326(4), 242-250. https://doi.org/10.1056/NEJM199201233260406
[6] Campeau, L. (1976). Grading of angina pectoris. Circulation, 54(3), 522-523. https://doi.org/10.1161/01.CIR.54.3.522
[7] Thygesen, K., Alpert, J. S., Jaffe, A. S., et al. (2018). Fourth Universal Definition of Myocardial Infarction. European Heart Journal, 40(3), 237-269. https://doi.org/10.1093/eurheartj/ehy462
[8] O'Gara, P. T., Kushner, F. G., Ascheim, D. D., et al. (2013). 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. Journal of the American College of Cardiology, 61(4), e78-e140. https://doi.org/10.1016/j.jacc.2012.11.019
[9] Wallentin, L., Becker, R. C., Budaj, A., et al. (2009). Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes (PLATO Trial). New England Journal of Medicine, 361(11), 1045-1057. https://doi.org/10.1056/NEJMoa0904327
[10] Yusuf, S., Mehta, S. R., Chrolavicius, S., et al. (2006). Comparison of Fondaparinux and Enoxaparin in Acute Coronary Syndromes (OASIS-5). New England Journal of Medicine, 354(14), 1464-1476. https://doi.org/10.1056/NEJMoa055443