
Pneumosclerosis and Emphysema: Pathogenesis, Diagnostic Standards, and Contemporary Management Strategies
1. Ragunath
Yogashree
2. A. Esengeldi kyzy
(1. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic)
Abstract
Pneumosclerosis and pulmonary emphysema represent two closely related yet pathologically distinct chronic respiratory conditions that together contribute substantially to global morbidity and mortality. Pneumosclerosis is characterized by the progressive replacement of functional pulmonary parenchyma by fibrous connective tissue, leading to restrictive ventilatory impairment and impaired gas exchange. Pulmonary emphysema, a central component of Chronic Obstructive Pulmonary Disease (COPD), is defined by permanent, abnormal enlargement of the air spaces distal to the terminal bronchioles accompanied by destruction of alveolar walls without obvious fibrosis. Both conditions share overlapping etiological pathways—including chronic inflammation, oxidative stress, and protease-antiprotease imbalance—yet differ fundamentally in their structural sequelae and clinical presentations. This review examines the epidemiology, classification, and pathophysiological mechanisms of pneumosclerosis and emphysema, outlines current evidence-based diagnostic standards including high-resolution computed tomography (HRCT), pulmonary function testing, and histopathological criteria, and discusses contemporary pharmacological and non-pharmacological management guided by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines.
Keywords: Pneumosclerosis, Pulmonary Fibrosis, Emphysema, COPD, Pulmonary Function Tests, HRCT, GOLD Guidelines, Alveolar Destruction.
1. Introduction
Chronic respiratory diseases represent a growing public health challenge, affecting over 500 million people worldwide and ranking as the third leading cause of death globally [1]. Among these, pneumosclerosis and pulmonary emphysema occupy a prominent position due to their insidious onset, progressive course, and significant impact on quality of life and functional capacity. The Global Burden of Disease Study 2019 estimated that COPD—of which emphysema is a cardinal structural feature—was responsible for approximately 3.23 million deaths annually, while interstitial lung diseases encompassing various forms of pneumosclerosis collectively affected over 5 million individuals worldwide [2].
Pneumosclerosis, derived from the Greek words pneumon (lung) and skleros (hard), refers broadly to the pathological process by which normal, compliant lung parenchyma is replaced by stiff, non-functional fibrous tissue. This fibrotic remodeling may arise as the final common pathway of diverse insults, including repeated infections, autoimmune disorders, occupational dust exposure, drug toxicity, and idiopathic processes. Emphysema, by contrast, reflects a destructive rather than fibrotic process: the progressive breakdown of alveolar septae by inflammatory mediators and proteolytic enzymes, resulting in abnormally enlarged, non-functional air spaces and loss of elastic recoil [3].
Despite their distinct pathological signatures, pneumosclerosis and emphysema frequently coexist in the form of Combined Pulmonary Fibrosis and Emphysema (CPFE) syndrome, a challenging condition in which spirometric parameters may appear deceptively normal while severe gas exchange impairment and pulmonary hypertension dominate the clinical picture. This review provides a structured analysis of both conditions from a unified pathophysiological, diagnostic, and therapeutic perspective.
2. Classification
2.1 Classification of Pneumosclerosis
Pneumosclerosis may be classified according to its distribution, etiology, and histopathological pattern. The major categories recognized in current practice include [1, 4]:
Post-infectious pneumosclerosis: Arising from repeated or incompletely resolved pulmonary infections (bacterial, viral, fungal, or mycobacterial) that trigger chronic inflammation and progressive fibrotic repair. Tuberculosis is a historically significant cause, particularly prevalent in Central Asian and Eastern European populations.
Occupational pneumosclerosis (Pneumoconiosis): Caused by chronic inhalation of mineral dusts. Principal subtypes include silicosis (silica dust), coal workers' pneumoconiosis (coal dust), and asbestosis (asbestos fibers). These forms carry significant medicolegal and occupational health implications.
Idiopathic Pulmonary Fibrosis (IPF): The most common idiopathic interstitial pneumonia, characterized by a Usual Interstitial Pneumonia (UIP) histopathological pattern on lung biopsy. IPF carries a median survival of 3–5 years from diagnosis without antifibrotic treatment [4].
Connective Tissue Disease-associated Interstitial Lung Disease (CTD-ILD): Occurring in the context of systemic autoimmune diseases such as rheumatoid arthritis, systemic sclerosis, and polymyositis/dermatomyositis.
Drug-induced pneumosclerosis: Caused by agents such as bleomycin, amiodarone, methotrexate, and nitrofurantoin.
2.2 Classification of Emphysema
Pulmonary emphysema is classified anatomically based on the portion of the acinus predominantly affected [3, 5]:
Centriacinar (Centrilobular) emphysema: The most common type, primarily affecting the central portions of the secondary pulmonary lobule (respiratory bronchioles), with sparing of the distal alveoli. Strongly associated with cigarette smoking and predominantly involves the upper lobes.
Panacinar (Panlobular) emphysema: Uniform destruction of the entire acinus from the respiratory bronchiole to the alveolar sacs. Characteristically associated with α1-antitrypsin deficiency and predominantly involves the lower lobes.
Paraseptal (Distal acinar) emphysema: Affects the distal alveoli adjacent to pleura and interlobular septa. Frequently underlies primary spontaneous pneumothorax in young adults.
Irregular emphysema: Irregular acinar involvement associated with scarring; always associated with fibrosis.
3. Pathophysiology
3.1 Pathogenesis of Pneumosclerosis
The fibrotic process underlying pneumosclerosis follows a stereotyped sequence of events regardless of the initiating insult. Repeated epithelial injury—whether from infection, inhalation of toxic particles, autoimmune attack, or idiopathic triggers—activates resident alveolar macrophages and recruits circulating inflammatory cells. These cells release a cascade of pro-fibrotic mediators, most notably Transforming Growth Factor-β1 (TGF-β1), which is considered the master orchestrator of pulmonary fibrosis [4].
TGF-β1 drives the differentiation of quiescent fibroblasts into contractile, matrix-synthesizing myofibroblasts—the principal effector cells of fibrosis. Myofibroblast activation results in excessive deposition of collagen types I and III, fibronectin, and other extracellular matrix (ECM) components in the alveolar interstitium. This matrix deposition progressively obliterates the gas-exchanging surface area, dramatically reduces lung compliance, increases the work of breathing, and ultimately impairs oxygen transfer across the alveolar-capillary membrane [4, 6].
3.2 Pathogenesis of Emphysema
The central pathogenetic mechanism of emphysema is the protease-antiprotease imbalance hypothesis. Cigarette smoke and other inhaled toxins recruit large numbers of neutrophils and macrophages into the lung, which release excessive quantities of proteolytic enzymes—principally neutrophil elastase, matrix metalloproteinases (MMPs), and cathepsins. These proteases degrade the structural proteins of the alveolar wall, including elastin and collagen, causing alveolar septae to break down and coalesce into enlarged, non-functional spaces [3, 5].
Simultaneously, cigarette smoke inactivates α1-antitrypsin (AAT)—the principal endogenous inhibitor of neutrophil elastase—through oxidative modification of its active methionine residue, further tilting the protease-antiprotease balance toward destruction. Genetic deficiency of AAT (PiZZ phenotype) exacerbates this imbalance profoundly, explaining the early-onset, lower-lobe emphysema seen in AAT-deficient individuals [5]. Loss of alveolar elastic recoil results in dynamic airway collapse during expiration, air trapping, lung hyperinflation, and progressive airflow limitation—the hallmarks of obstructive ventilatory impairment.
4. Clinical Features
4.1 Clinical Presentation of Pneumosclerosis
Pneumosclerosis typically presents insidiously, with patients often attributing early symptoms to aging or deconditioning. The cardinal clinical features include [1, 4]:
Progressive exertional dyspnea: Initially provoked by moderate exertion, advancing to dyspnea at rest in severe cases. This is the most common presenting complaint and the primary driver of functional decline.
Non-productive dry cough: A persistent, irritating cough without significant sputum production, frequently the first symptom reported by patients with IPF.
Velcro-like bibasal inspiratory crackles: A characteristic auscultatory finding in IPF and other UIP-pattern diseases, produced by the sudden opening of fibrotic small airways. Their presence has high specificity for interstitial lung disease.
Finger clubbing: Present in approximately 50% of IPF patients; less common in other interstitial pneumonias.
Signs of pulmonary hypertension and cor pulmonale: Including elevated jugular venous pressure, right ventricular heave, loud P2, and peripheral edema in advanced disease.
4.2 Clinical Presentation of Emphysema
Emphysema classically manifests within the broader COPD syndrome. The classic presentation of pure emphysema (“pink puffer” phenotype) includes [3, 5]:
Severe dyspnea with relatively mild cough: Patients expend enormous respiratory effort to maintain relatively normal blood gas values, often appearing breathless but without significant cyanosis.
Barrel chest deformity: Due to chronic hyperinflation with increased AP diameter, elevated ribs, and horizontal positioning.
Pursed-lip breathing: An instinctive compensatory mechanism that generates positive end-expiratory pressure to prevent dynamic airway collapse during exhalation.
Hyperresonance on percussion and diminished breath sounds: Reflecting the overinflated, air-filled lung fields.
Cachexia and muscle wasting: Due to chronic systemic inflammation, increased work of breathing, and hypoxia-driven catabolism.
5. Diagnostic Standards
5.1 Pulmonary Function Testing (PFT)
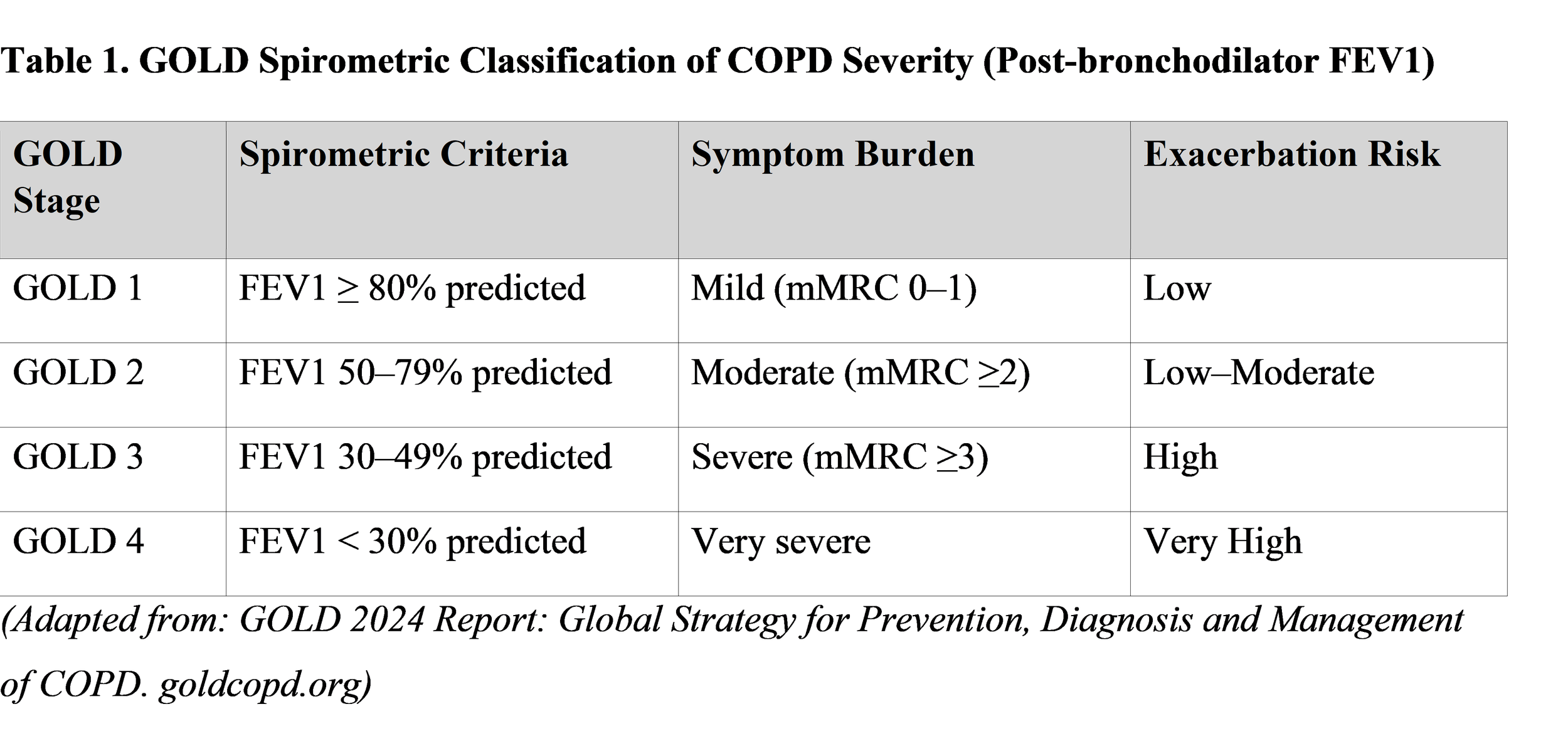
Spirometry is the cornerstone of functional assessment. Pneumosclerosis produces a restrictive ventilatory defect: reduced Forced Vital Capacity (FVC), reduced Total Lung Capacity (TLC), and a normal or elevated FEV1/FVC ratio. Emphysema produces an obstructive defect: reduced FEV1, normal or reduced FVC, and an FEV1/FVC ratio below 0.70 post-bronchodilator (the GOLD diagnostic criterion). The diffusion capacity for carbon monoxide (DLCO) is reduced in both conditions—an early and sensitive marker of parenchymal gas exchange impairment [3, 6]. The ATS/ERS task force recommends post-bronchodilator spirometry for all patients with suspected COPD.
5.2 High-Resolution Computed Tomography (HRCT)
HRCT of the thorax is the most sensitive non-invasive imaging modality for both pneumosclerosis and emphysema. In IPF/UIP-pattern pneumosclerosis, HRCT demonstrates bilateral, predominantly basal and subpleural reticular opacities with honeycombing (clustered cystic air spaces) with or without traction bronchiectasis. A confident HRCT diagnosis of UIP pattern eliminates the need for surgical lung biopsy per the 2022 ATS/ERS/JRS/ALAT guidelines [4, 6]. In emphysema, HRCT demonstrates low-attenuation areas (LAA) without visible walls, allowing precise quantification of emphysema extent and subtype classification that spirometry cannot provide.
5.3 Laboratory and Additional Investigations
Relevant laboratory investigations include arterial blood gas analysis (ABG) for assessment of hypoxemia and hypercapnia, serum lactate dehydrogenase (LDH) and KL-6 as markers of alveolar epithelial injury in interstitial pneumonias, autoimmune serology (ANA, anti-dsDNA, anti-SCL-70, anti-CCP) for CTD-ILD evaluation, and α1-antitrypsin serum levels and phenotyping (Pi typing) for AAT deficiency assessment in emphysema patients with early onset or lower-lobe predominance [5]. Six-minute walk test (6MWT) and cardiopulmonary exercise testing (CPET) provide objective functional capacity assessment and inform prognosis.
6. Management
6.1 Management of Pneumosclerosis
Treatment of pneumosclerosis is guided by the underlying etiology, rate of progression, and functional status.
Antifibrotic therapy: For IPF specifically, two antifibrotic agents are approved—Nintedanib (a tyrosine kinase inhibitor targeting VEGFR, FGFR, and PDGFR) and Pirfenidone (with anti-inflammatory and antifibrotic properties)—both demonstrated to reduce the annual decline in FVC by approximately 50% compared to placebo in pivotal trials (INPULSIS, CAPACITY/ASCEND) [4, 7].
Immunosuppression for CTD-ILD: Mycophenolate mofetil, azathioprine, and rituximab (for refractory cases) form the pharmacological backbone, guided by the underlying connective tissue diagnosis.
Corticosteroids: Used acutely for hypersensitivity pneumonitis and some CTD-ILD, but contraindicated in IPF (may accelerate decline per PANTHER-IPF trial).
Lung transplantation: The only treatment modality that significantly extends survival in advanced IPF. Bilateral lung transplantation is preferred. Referral should be considered early, as waiting times are prolonged [4].
6.2 Management of Emphysema/COPD
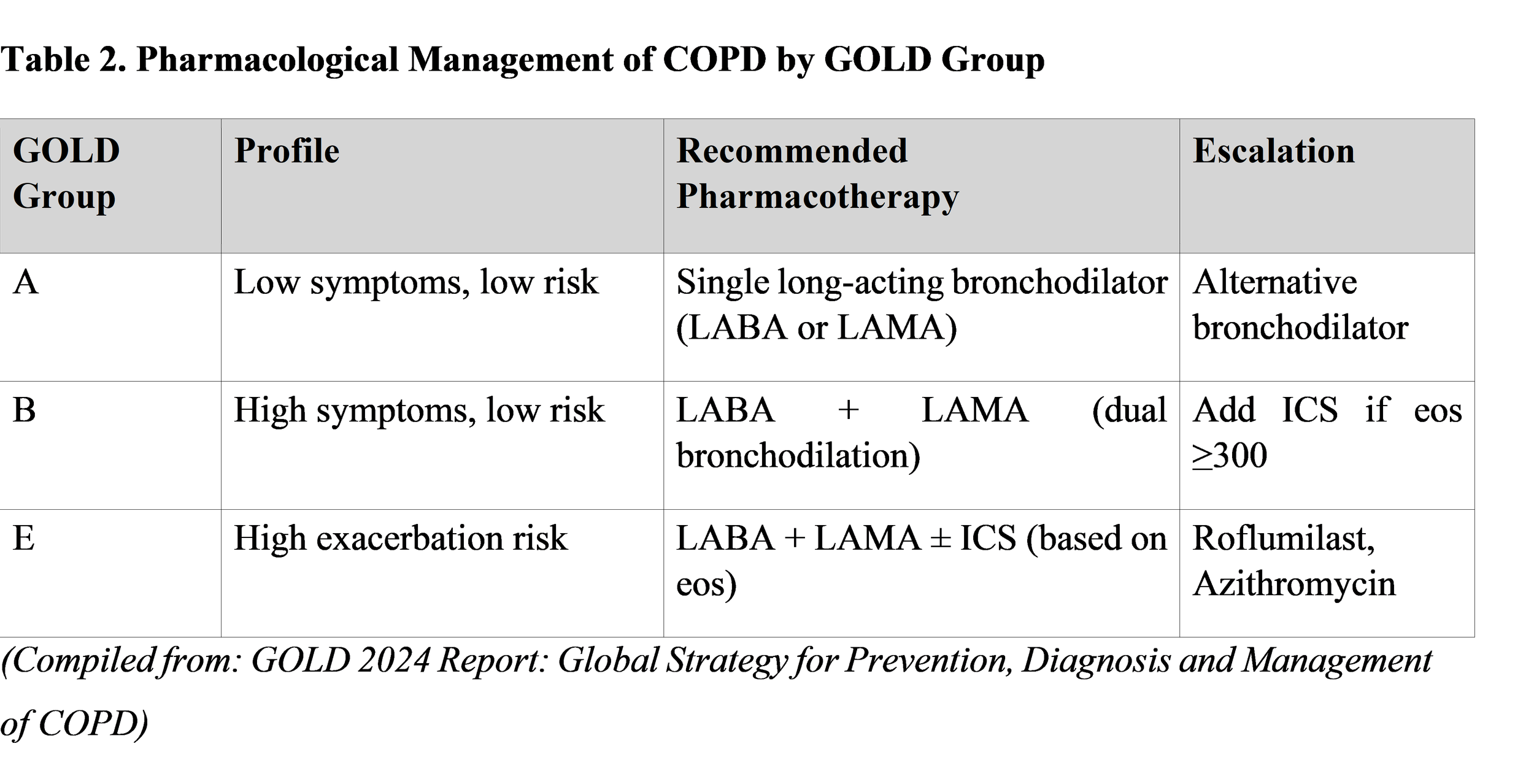
Management follows the GOLD 2024 ABCD assessment framework, stratifying patients by symptom burden and exacerbation history to guide pharmacotherapy [3]:
Bronchodilator therapy: Long-acting β2-agonists (LABA: Salmeterol, Formoterol, Indacaterol) and long-acting muscarinic antagonists (LAMA: Tiotropium, Umeclidinium, Glycopyrronium) form the cornerstone of COPD maintenance therapy. Dual bronchodilation (LABA + LAMA) is superior to monotherapy for symptom relief and exacerbation prevention.
Inhaled corticosteroids (ICS): Reserved for patients with frequent exacerbations (GOLD 3–4) or blood eosinophil count ≥ 300 cells/μL, as combination ICS/LABA/LAMA triple therapy reduces exacerbation rates and improves quality of life.
α1-Antitrypsin Augmentation Therapy: Weekly intravenous infusions of pooled human AAT (Prolastin-C, Zemaira) for patients with documented AAT deficiency (serum AAT < 11 μmol/L) and obstructive spirometry have been shown to slow emphysema progression by CT densitometry [5, 8].
Pulmonary Rehabilitation: A multidisciplinary program combining exercise training, nutritional support, and education. The strongest evidence-based intervention to improve exercise tolerance, health-related quality of life, and reduce hospital admissions in COPD [3].
Surgical and bronchoscopic interventions: Lung Volume Reduction Surgery (LVRS) benefits patients with upper-lobe predominant emphysema and low post-rehabilitation exercise capacity (NETT trial). Bronchoscopic Lung Volume Reduction (BLVR) using endobronchial valves (Zephyr, PulmoValve) offers a less invasive alternative with significant benefit in heterogeneous emphysema with intact interlobar fissures [8].
6.3 Oxygen Therapy and Ventilatory Support
Long-term oxygen therapy (LTOT) is indicated when resting PaO2 ≤ 55 mmHg (or SpO2 ≤ 88%) on two separate measurements at least three weeks apart in stable patients. LTOT improves survival in hypoxemic COPD patients (MRC and NOTT trials). Non-invasive positive pressure ventilation (NIV/BiPAP) is beneficial for patients with hypercapnic respiratory failure (PaCO2 > 55 mmHg) and has been shown to reduce hospital admissions and improve survival in severe stable COPD with chronic hypercapnia [3, 9].
7. Combined Pulmonary Fibrosis and Emphysema (CPFE)
CPFE is a distinct clinical syndrome recognized since Cottin et al. first described it in 2005, characterized by upper-lobe emphysema coexisting with lower-lobe fibrosis on HRCT. It predominantly affects older male smokers and presents with the functional paradox of near-normal spirometry despite severe dyspnea and dramatically reduced DLCO [6]. The syndrome carries a substantially worse prognosis than either condition alone, with pulmonary hypertension developing in 30–50% of patients and a median survival of approximately 2.1 years after diagnosis [6, 10]. Treatment is currently empiric and supportive; no randomized trials have specifically addressed CPFE pharmacotherapy, representing an urgent unmet research need.
[Figure 3]
Figure 3. Proposed diagnostic and management algorithm for a patient presenting with suspected pneumosclerosis or emphysema. Key decision nodes include spirometric pattern (obstructive vs. restrictive), HRCT findings, AAT serum levels, and autoimmune serology to guide etiological classification and appropriate therapeutic pathway. (Adapted from: Raghu, G. et al., ATS/ERS/JRS/ALAT Clinical Practice Guideline: Diagnosis of Idiopathic Pulmonary Fibrosis, AJRCCM, 2022).
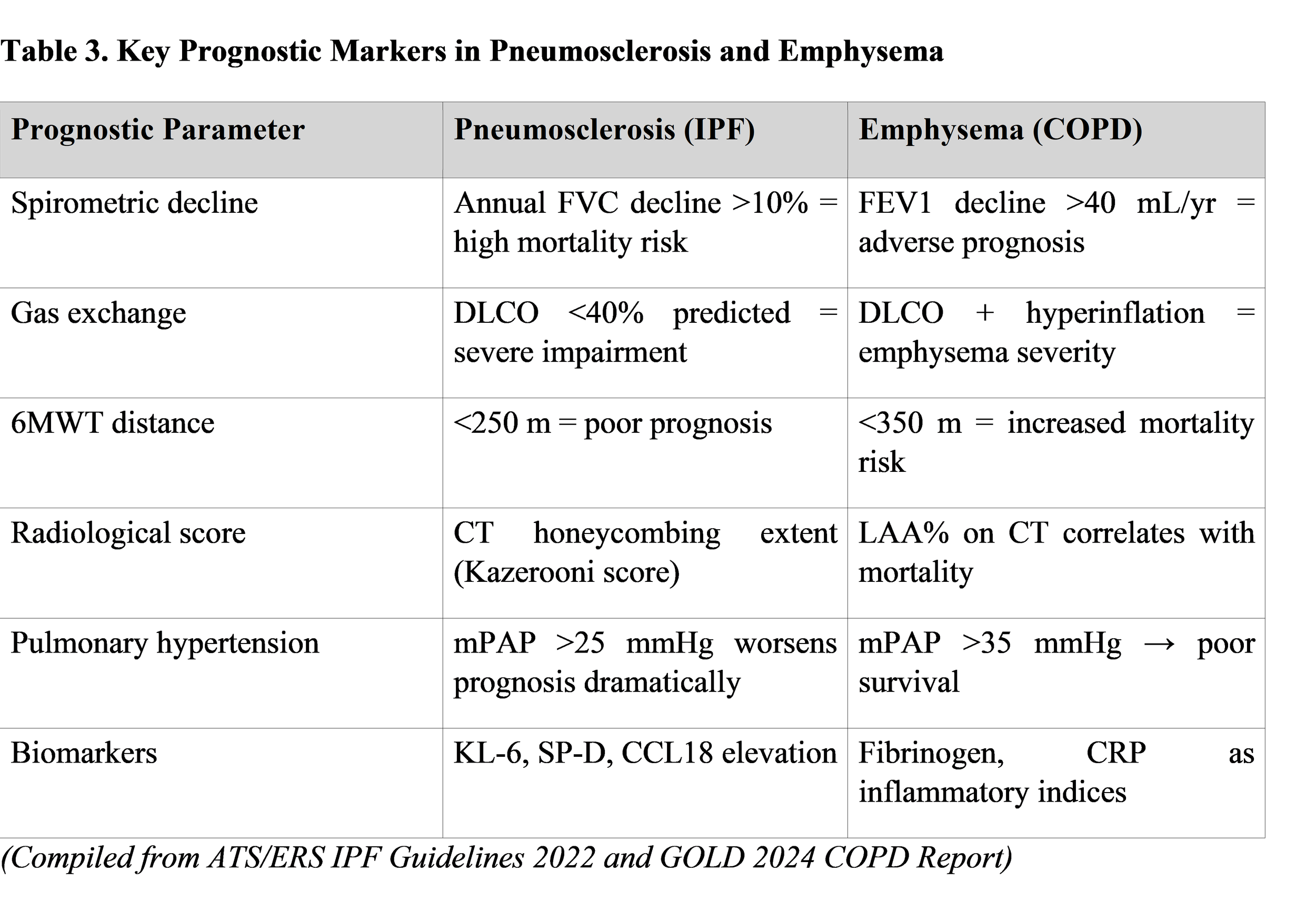
8. Prognosis and Monitoring
9. Conclusion
Pneumosclerosis and pulmonary emphysema, though pathologically divergent—one characterized by progressive fibrotic consolidation and the other by destructive alveolar rarefaction—share the common clinical destiny of progressive, disabling respiratory impairment. Both conditions demand early diagnosis through systematic application of pulmonary function testing and HRCT imaging, targeted etiological investigation, and timely initiation of evidence-based treatment. The introduction of antifibrotic agents for IPF and the evolution of triple bronchodilator and endobronchial valve therapies for emphysema represent landmark advances in the management of these historically treatment-resistant conditions. The emerging CPFE syndrome serves as a critical reminder that these diseases do not exist in isolation and that a comprehensive, individualized approach is essential. Future research priorities include the development of biomarker-guided treatment algorithms, novel antifibrotic targets for non-IPF pneumoscleroses, and dedicated randomized trials for CPFE.
Disclosure of Funding Sources
The authors declare that no specific funding was received for the preparation of this review article. No granting agencies, institutional support, or non-material project frameworks contributed to this work.
10. References
[1] Raghu, G., Remy-Jardin, M., Richeldi, L., et al. (2022). Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. American Journal of Respiratory and Critical Care Medicine, 205(9), e18–e47. https://doi.org/10.1164/rccm.202202-0399ST
[2] GBD 2019 Chronic Respiratory Disease Collaborators. (2020). Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017. The Lancet Respiratory Medicine, 8(6), 585–596. https://doi.org/10.1016/S2213-2600(20)30105-3
[3] Global Initiative for Chronic Obstructive Lung Disease (GOLD). (2024). Global Strategy for Prevention, Diagnosis and Management of COPD: 2024 Report. https://goldcopd.org/2024-gold-report/
[4] Lederer, D. J., & Martinez, F. J. (2018). Idiopathic Pulmonary Fibrosis. New England Journal of Medicine, 378(19), 1811–1823. https://doi.org/10.1056/NEJMra1705751
[5] Silverman, E. K. (2020). Genetics of COPD. Annual Review of Physiology, 82, 413–431. https://doi.org/10.1146/annurev-physiol-021317-121224
[6] Cottin, V., Selman, M., Inoue, Y., et al. (2022). Syndrome of Combined Pulmonary Fibrosis and Emphysema: An Official ATS/ERS/JRS/ALAT Research Statement. American Journal of Respiratory and Critical Care Medicine, 206(4), e7–e41. https://doi.org/10.1164/rccm.202206-1041ST
[7] Richeldi, L., du Bois, R. M., Raghu, G., et al. (2014). Efficacy and Safety of Nintedanib in Idiopathic Pulmonary Fibrosis (INPULSIS trial). New England Journal of Medicine, 370(22), 2071–2082. https://doi.org/10.1056/NEJMoa1402584
[8] Valipour, A., Shah, P. L., Herth, F. J., et al. (2016). Two-Year Outcomes After Bilateral Endobronchial Valve (Zephyr) Placement in Patients with Severe Emphysema: Results from the TRANSFORM Study. Annals of the American Thoracic Society, 13(10), 1716–1725. https://doi.org/10.1513/AnnalsATS.201603-193OC
[9] Wedzicha, J. A., Miravitlles, M., Hurst, J. R., et al. (2017). Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. European Respiratory Journal, 49(3), 1600791. https://doi.org/10.1183/13993003.00791-2016
[10] Ryerson, C. J., Hartman, T., Elicker, B. M., et al. (2013). Clinical features and outcomes in combined pulmonary fibrosis and emphysema in idiopathic pulmonary fibrosis. Chest, 144(1), 234–240. https://doi.org/10.1378/chest.12-2403
[11] Kumar, V., Abbas, A. K., & Aster, J. C. (2021). Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. ISBN: 978-0323531139.
[12] Webb, W. R., Muller, N. L., & Naidich, D. P. (2015). High-Resolution CT of the Lung (5th ed.). Lippincott Williams & Wilkins. ISBN: 978-1451186710.