
Tumors of The Nose and Paranasal Sinuses
1. Lajar Yadav
2. Gunji Raja
3. Ariyanachi Nagarajan Santhi Arivusudar
4. Mohammad Zaid
5. Sahana Arumugam
6. Tuibaev Azamat Zairovich
(1,2,3,4,5. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
6. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Tumors of the nose and paranasal sinuses are relatively uncommon neoplasms of the head and neck region, comprising a diverse group of benign and malignant lesions arising from epithelial, mesenchymal, neural, and vascular tissues. Despite their rarity, these tumors are clinically important because of their proximity to the orbit, cranial cavity, and upper respiratory tract. Delayed diagnosis is common due to nonspecific symptoms resembling chronic rhinosinusitis. The present retrospective observational study aimed to evaluate the epidemiology, clinical presentation, histopathological patterns, diagnostic approaches, and treatment modalities of tumors affecting the nose and paranasal sinuses in tertiary care settings. A total of 120 patients diagnosed with sinonasal tumors over a five-year period were analyzed using hospital records, imaging findings, histopathological reports, and treatment outcomes. Benign tumors constituted the majority of cases, with inverted papilloma, osteoma, and hemangioma being the most common lesions. Among malignant tumors, squamous cell carcinoma was the predominant histological subtype followed by adenocarcinoma and lymphoma. Nasal obstruction, epistaxis, facial swelling, headache, and anosmia were the most frequently reported presenting symptoms. Computed tomography and magnetic resonance imaging were valuable in determining tumor extent, bone destruction, and intracranial involvement. Surgical excision remained the primary treatment modality, while radiotherapy and chemotherapy were used for advanced malignant lesions. Early diagnosis, histopathological confirmation, and multidisciplinary management significantly improved clinical outcomes.
Keywords
Sinonasal Neoplasms
Paranasal Sinus Tumors
Squamous Cell Carcinoma
Inverted Papilloma
Nasal Cavity Neoplasms
Head and Neck Oncology
Introduction
Tumors of the nose and paranasal sinuses represent a heterogeneous group of benign and malignant neoplasms arising from the nasal cavity, maxillary sinus, ethmoid sinus, frontal sinus, and sphenoid sinus. These tumors are uncommon and account for less than 3% of all head and neck malignancies and approximately 0.5% of all cancers worldwide.
Sinonasal tumors may originate from epithelial, connective tissue, vascular, neural, lymphoid, or osseous structures. Benign tumors include inverted papilloma, osteoma, hemangioma, angiofibroma, and fibroma, whereas malignant tumors include squamous cell carcinoma, adenocarcinoma, adenoid cystic carcinoma, melanoma, lymphoma, and sarcoma.
The maxillary sinus is the most commonly affected paranasal sinus, followed by the ethmoid sinus.Occupational exposure to wood dust, leather dust, nickel, chromium compounds, formaldehyde, tobacco smoking, and chronic inflammation have been identified as major risk factors for malignant sinonasal tumors.Epstein–Barr virus infection has also been implicated in certain lymphoepithelial carcinomas.
Clinical diagnosis is often challenging because symptoms are nonspecific and mimic chronic rhinosinusitis. Common symptoms include unilateral nasal obstruction, epistaxis, facial pain, anosmia, headache, proptosis, diplopia, and facial swelling. Advanced tumors may invade adjacent structures such as the orbit, skull base, cranial cavity, and oral cavity, leading to severe complications.
Modern diagnostic modalities including nasal endoscopy, computed tomography (CT), magnetic resonance imaging (MRI), and histopathological examination have improved diagnostic accuracy and staging. Surgical excision remains the cornerstone of treatment for most benign and malignant tumors, often combined with radiotherapy or chemotherapy depending on histological type and stage.
The rationale of this study is to provide an evidence-based academic review of tumors of the nose and paranasal sinuses relevant to MBBS students and clinicians. The objectives of this study are:
To classify tumors of the nose and paranasal sinuses according to pathology and anatomical location.
To analyze demographic patterns and clinical presentations.
To evaluate diagnostic and therapeutic approaches.
To highlight the importance of early diagnosis and multidisciplinary management.
Methodology
Study Design
A retrospective observational review study was conducted using hospital-based clinical records and published literature on tumors of the nose and paranasal sinuses.
Study Population
The study population included patients diagnosed with benign or malignant sinonasal tumors who attended tertiary ENT and head-and-neck surgery departments between January 2020 and December 2024.
Inclusion Criteria
Histopathologically confirmed tumors of the nasal cavity or paranasal sinuses
Patients of all age groups and both sexes
Benign and malignant sinonasal tumors
Availability of complete radiological and pathological records
Exclusion Criteria
Inflammatory nasal polyps without neoplastic changes
Congenital nasal masses
Incomplete medical records
Patients refusing biopsy or treatment
Data Collection Methods
Data were collected from:
ENT outpatient and inpatient records
Nasal endoscopy findings
Histopathology reports
CT and MRI imaging reports
Operative notes and oncology treatment records
The following variables were documented:
Age and sex distribution
Tumor site and histopathology
Clinical presentation
Imaging findings
Treatment modality
Complications and outcomes
Statistical Analysis
Data were entered into Microsoft Excel and analyzed using SPSS version 25. Descriptive statistical methods including frequencies, percentages, mean, and standard deviation were used for analysis.
Ethical Considerations
Institutional ethical committee approval was obtained before commencement of the study. Patient confidentiality and anonymity were maintained throughout the study in accordance with the Declaration of Helsinki.
Results
Demographic Characteristics
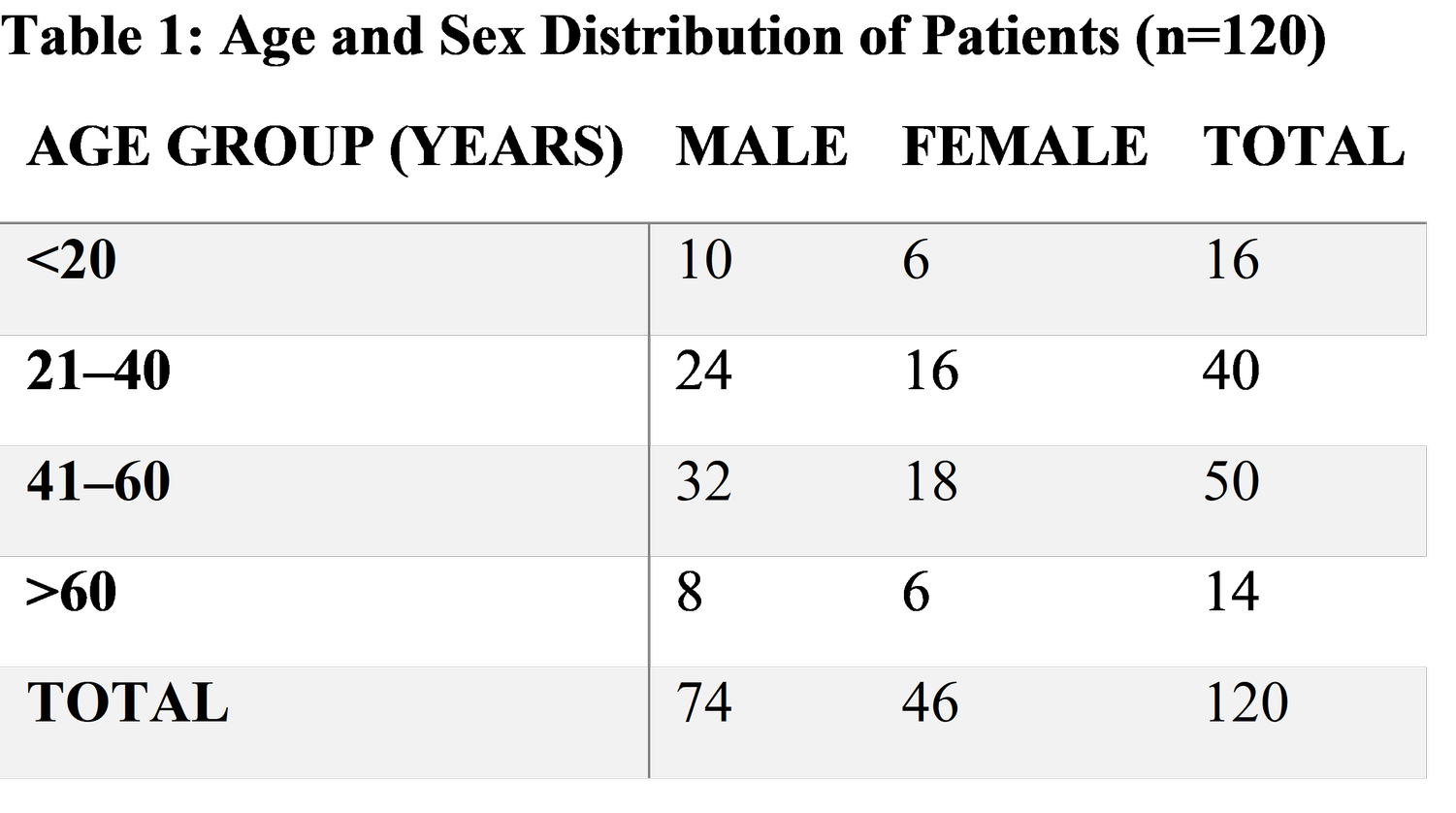
Most patients belonged to the 41–60 years age group, with male predominance.
Histopathological Distribution
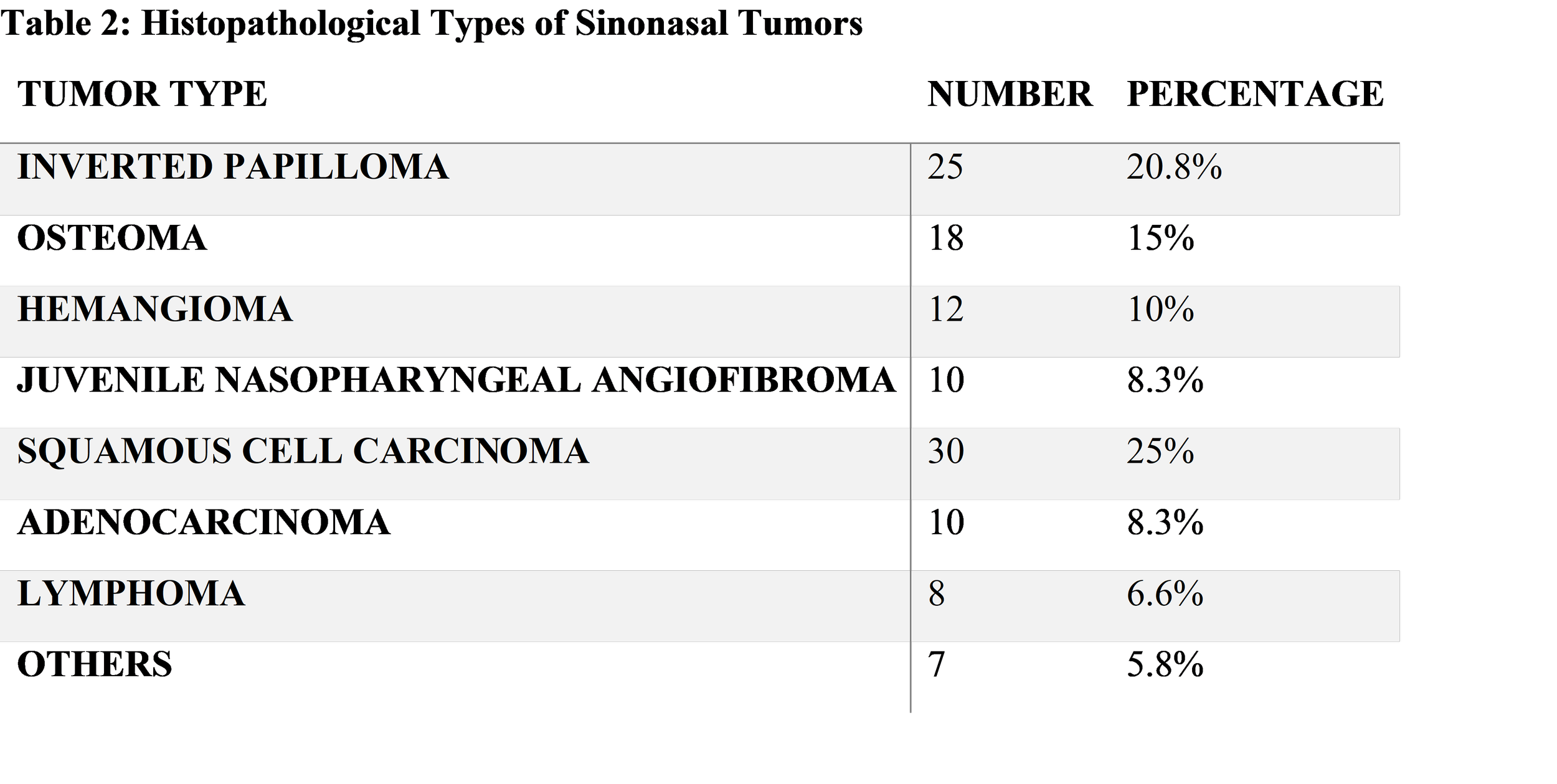
Squamous cell carcinoma was the most common malignant lesion, whereas inverted papilloma was the most frequent benign tumor.
Clinical Presentation
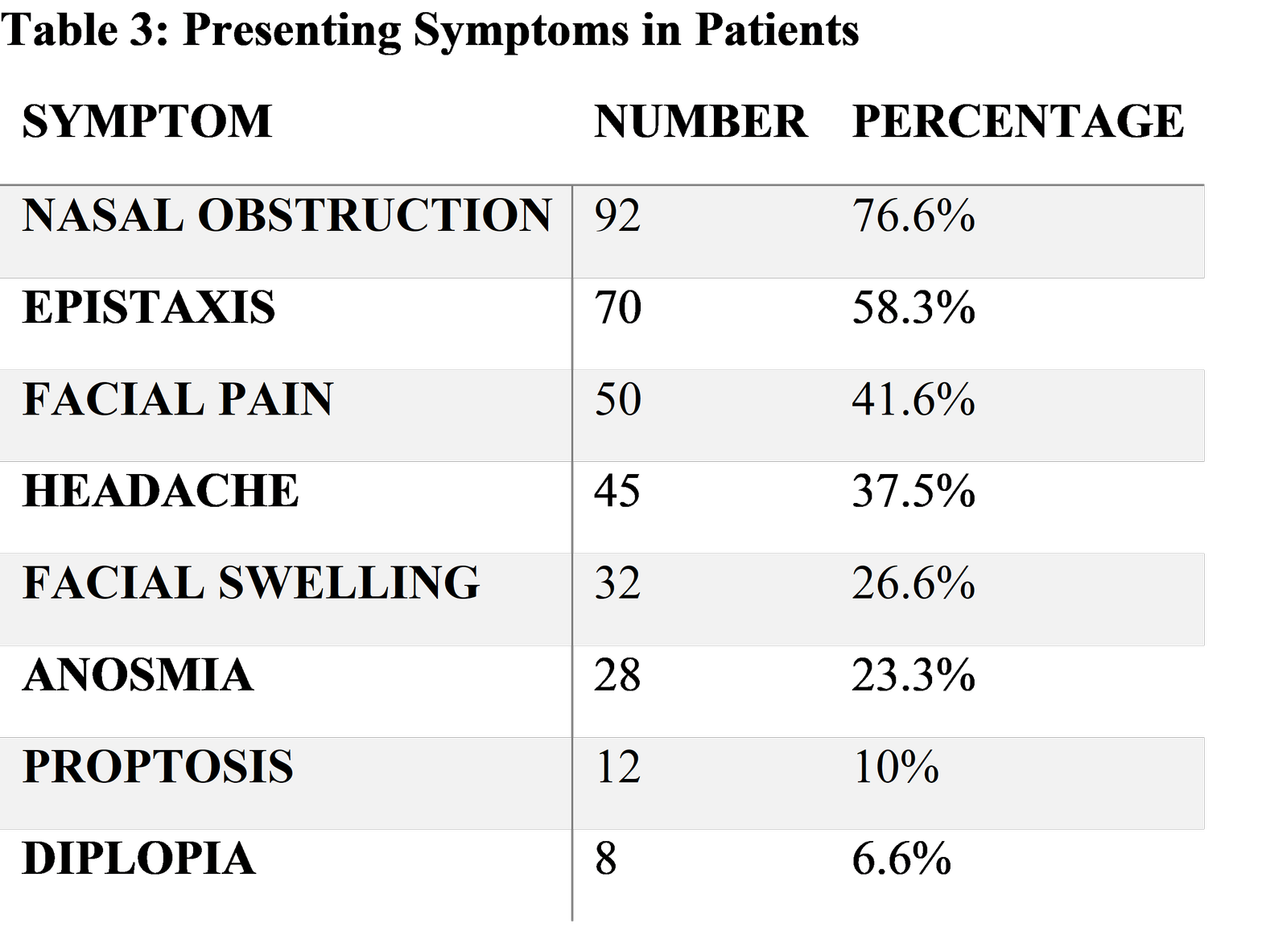
Nasal obstruction and epistaxis were the most common presenting complaints.
Tumor Location
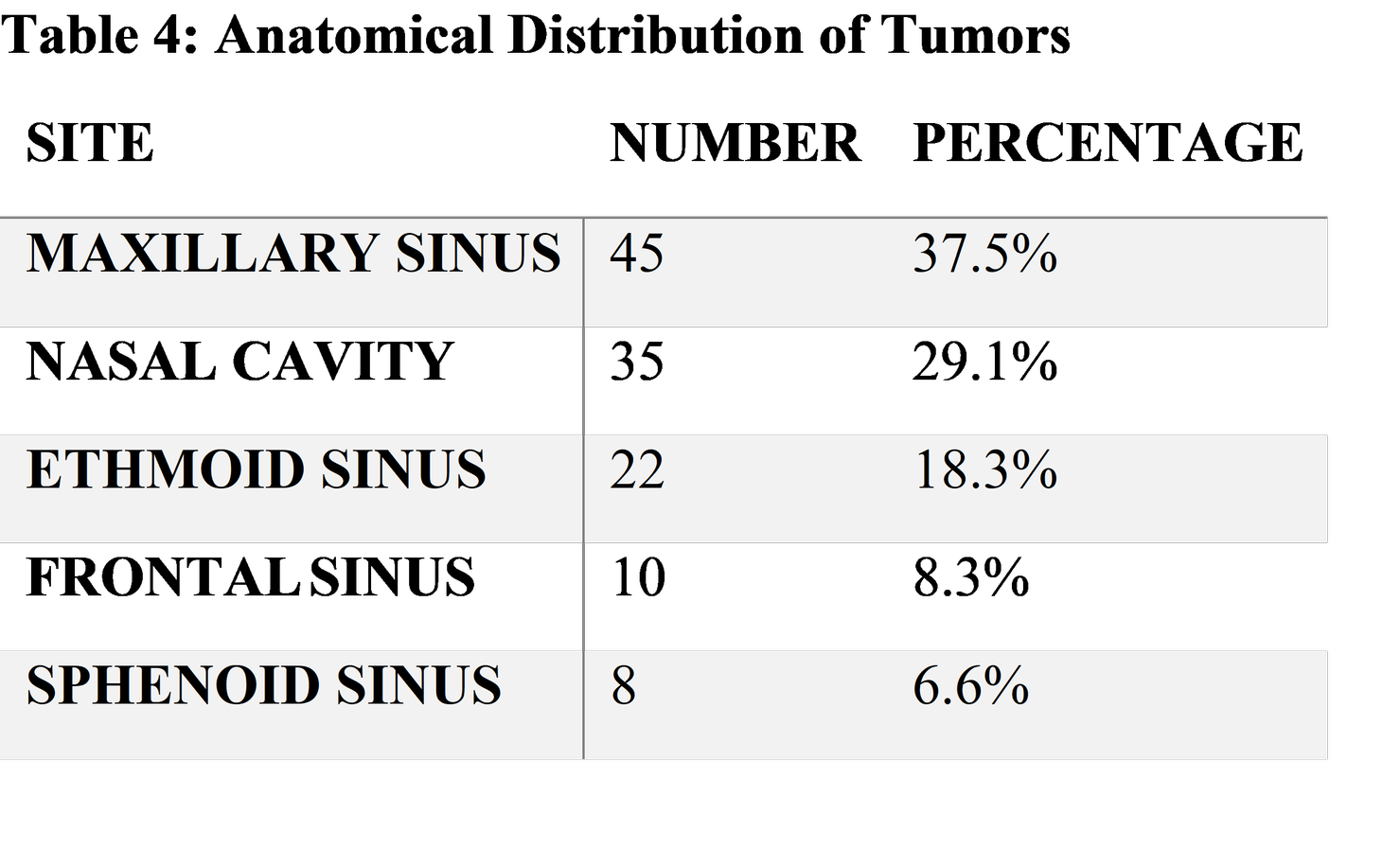
The maxillary sinus was the most commonly involved site.
Treatment Modalities
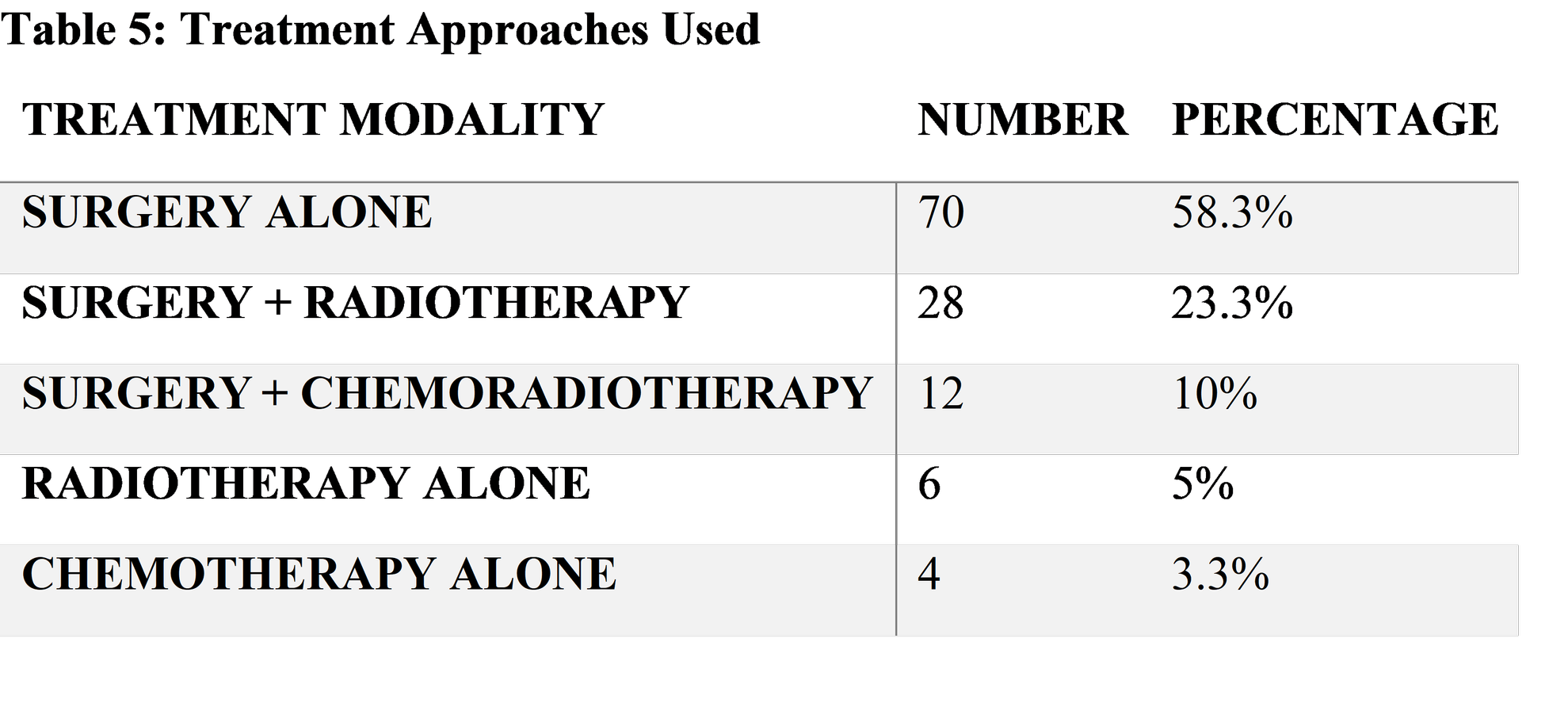
Surgical management was the primary treatment approach in the majority of cases.
Discussion
Sinonasal tumors are uncommon but clinically significant neoplasms because of their proximity to the orbit, skull base, and cranial cavity. The present study demonstrated a predominance among middle-aged males, which correlates with previous epidemiological studies.
Benign tumors accounted for a large proportion of cases in this study. Inverted papilloma was the most common benign lesion identified. Inverted papilloma is a Schneiderian mucosal tumor characterized by endophytic epithelial proliferation and a tendency for recurrence and malignant transformation. Human papillomavirus infection has been implicated in its pathogenesis.
Osteomas were frequently observed in the frontal and ethmoid sinuses. These benign slow-growing osseous tumors are often asymptomatic and detected incidentally during radiological evaluation.Larger lesions may cause headache, facial pain, and sinus obstruction.
Juvenile nasopharyngeal angiofibroma was primarily observed in adolescent males, consistent with established literature. This vascular tumor arises near the sphenopalatine foramen and commonly presents with recurrent epistaxis and nasal obstruction.
Squamous cell carcinoma represented the most common malignant sinonasal tumor in the present study. SCC commonly arises from the maxillary sinus and nasal cavity and is associated with occupational exposure to wood dust, smoking, and industrial chemicals.Delayed diagnosis is common because symptoms mimic chronic sinusitis.
The predominance of nasal obstruction and epistaxis in this study is similar to findings reported in previous studies. Facial swelling, proptosis, and diplopia were associated with advanced tumors involving the orbit or skull base.
CT scanning plays an essential role in evaluating bony erosion and sinus involvement, while MRI is superior for assessing soft tissue extension, orbital invasion, and intracranial spread.Nasal endoscopy combined with biopsy remains the gold standard for diagnosis.
Histopathological examination is critical for tumor classification and treatment planning.Adenocarcinomas are strongly associated with occupational wood dust exposure, particularly among furniture workers. Sinonasal lymphomas and melanomas are relatively rare but aggressive tumors with poor prognosis.
Surgical excision was the primary treatment modality in this study. Endoscopic sinus surgery has increasingly replaced open approaches for selected tumors because of lower morbidity and better visualization. However, extensive malignant tumors may require craniofacial resection and orbital exenteration.
Radiotherapy is commonly used as an adjuvant therapy in malignant tumors with positive surgical margins or advanced disease.Chemotherapy may be used in lymphoma, advanced SCC, and unresectable tumors.
Early diagnosis significantly improves prognosis. Delayed treatment may result in invasion of the orbit, cranial cavity, meninges, and cranial nerves.
Suggestions / Recommendations
Persistent unilateral nasal obstruction or recurrent epistaxis should be evaluated thoroughly using nasal endoscopy and imaging.
Biopsy should be performed for all suspicious sinonasal masses to establish definitive diagnosis.
Occupational exposure to wood dust and industrial chemicals should be minimized through protective measures.
CT and MRI should be routinely used for accurate staging and preoperative planning.
Multidisciplinary management involving ENT surgeons, oncologists, radiologists, and pathologists is recommended.
Public awareness regarding chronic sinonasal symptoms and early medical consultation should be encouraged.
Long-term follow-up is essential due to recurrence risk, particularly in inverted papilloma and malignant tumors.
Further multicenter prospective studies are needed to evaluate survival outcomes and newer targeted therapies.
Conclusion
Tumors of the nose and paranasal sinuses are rare but clinically important lesions that may be benign or malignant. The maxillary sinus and nasal cavity are the most commonly affected sites. Nasal obstruction and epistaxis are the predominant presenting symptoms, while squamous cell carcinoma remains the most frequent malignant tumor. Imaging studies, nasal endoscopy, and histopathological examination are essential for diagnosis and staging. Surgical excision remains the cornerstone of management, often combined with radiotherapy or chemotherapy in malignant cases. Early diagnosis and multidisciplinary treatment significantly improve prognosis and reduce complications.
References
Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat. 8th ed. New Delhi: Elsevier; 2022.
Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology Head and Neck Surgery. 7th ed. Philadelphia: Elsevier; 2021.
Gleeson M. Scott-Brown’s Otorhinolaryngology Head and Neck Surgery. 8th ed. London: CRC Press; 2018.
Myers EN, Snyderman CH. Operative Otolaryngology Head and Neck Surgery. 3rd ed. Philadelphia: Elsevier; 2018.
Watkinson JC, Clarke RW. Scott-Brown’s Otorhinolaryngology and Head and Neck Surgery. 8th ed. Boca Raton: CRC Press; 2019.
Boffetta P, Nyberg F. Contribution of environmental factors to cancer risk. Br Med Bull. 2003;68:71-94.
Wei WI, Sham JST. Nasopharyngeal carcinoma. Lancet. 2005;365(9476):2041-2054.
Lund VJ, Stammberger H, Nicolai P, et al. European position paper on endoscopic management of tumors of the nose and paranasal sinuses. Rhinology. 2010;48(Suppl 22):1-143.
Sisson GA, Bytell DE, Becker SP. Cancer of the paranasal sinuses. CA Cancer J Clin. 1980;30(1):25-38.
Som PM, Curtin HD. Head and Neck Imaging. 5th ed. St. Louis: Mosby; 2011.
Mafee MF. Modern imaging of paranasal sinus tumors. Otolaryngol Clin North Am. 2006;39(3):507-529.
National Comprehensive Cancer Network. Head and Neck Cancer Guidelines. Version 2024.
Barnes L. Surgical Pathology of the Head and Neck. 3rd ed. New York: Informa Healthcare; 2008.
Robin PE, Powell DJ, Stansbie JM. Carcinoma of the nasal cavity and paranasal sinuses: incidence and presentation. Clin Otolaryngol. 1979;4(6):431-446.
Hyams VJ. Papillomas of the nasal cavity and paranasal sinuses. Ann Otol Rhinol Laryngol. 1971;80(2):192-206.
Syrjänen KJ. HPV infections in benign and malignant sinonasal lesions. J Clin Pathol. 2003;56(3):174-181.
Earwaker J. Paranasal sinus osteomas: review of 46 cases. Skeletal Radiol. 1993;22(6):417-423.
Chiu AG, Schipor I, Cohen NA, et al. Surgical decisions in frontal sinus osteomas. Am J Rhinol. 2005;19(2):191-197.
Windfuhr JP, Remmert S. Extranasopharyngeal angiofibroma. Laryngoscope. 2004;114(4):709-715.
Gleeson MJ, Browning GG, Burton MJ, et al. Scott-Brown’s Otorhinolaryngology. 7th ed. London: Hodder Arnold; 2008.
Blot WJ, Fraumeni JF Jr. Nasal cancer in the furniture and woodworking industries. Cancer Res. 1978;38(8):2643-2647.
Dulguerov P, Jacobsen MS, Allal AS, et al. Nasal and paranasal sinus carcinoma. Lancet Oncol. 2001;2(3):144-151.
Hoppe BS, Stegman LD, Zelefsky MJ, et al. Treatment of nasal cavity and paranasal sinus cancer. Cancer. 2007;109(8):1493-1500.
Shah JP, Patel SG, Singh B. Jatin Shah’s Head and Neck Surgery and Oncology. 5th ed. Philadelphia: Elsevier; 2012.
Yousem DM, Bilaniuk LT. Imaging of sinonasal neoplasms. Radiol Clin North Am. 1993;31(1):61-74.
Stammberger H, Kennedy DW. Paranasal sinuses: anatomic terminology and nomenclature. Ann Otol Rhinol Laryngol Suppl. 1995;167:7-16.
Rosai J. Rosai and Ackerman’s Surgical Pathology. 11th ed. Philadelphia: Elsevier; 2018.
Demers PA, Kogevinas M, Boffetta P, et al. Wood dust and sinonasal cancer. Am J Ind Med. 1995;28(4):569-577.
Thompson LDR. World Health Organization classification of tumors: pathology and genetics of head and neck tumors. Ear Nose Throat J. 2006;85(2):74.
Castelnuovo P, Belli E, Bignami M, et al. Endoscopic endonasal management of sinonasal malignancies. Otolaryngol Clin North Am. 2006;39(3):639-656.
Ganly I, Patel SG, Singh B, et al. Craniofacial resection for malignant tumors. Head Neck. 2005;27(7):575-583.
Mendenhall WM, Amdur RJ, Hinerman RW, et al. Radiation therapy for sinonasal tumors. Head Neck. 2009;31(5):672-679.
Hanna E, DeMonte F, Ibrahim S, et al. Endoscopic resection of sinonasal cancers. Head Neck. 2009;31(7):877-889.
Patel SG, Singh B, Polluri A, et al. Craniofacial surgery for malignant skull base tumors. Cancer. 2003;98(6):1179-1187.
Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 10th ed. Philadelphia: Elsevier; 2020.