
Tumors of the Ear
1. Varshitha Siddamsetty
2. Bhawna Rani Sahu
3. Devashish Yadav
4. Sarfaraz
5. Asif Khan
6. Tuibaev Azamat Zairovich
(1,2,3,4,5. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
6. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Tumors of the ear constitute a heterogeneous group of benign and malignant lesions involving the external ear, external auditory canal, middle ear, and inner ear. Although relatively uncommon compared with other head and neck neoplasms, these tumors are clinically significant because delayed diagnosis may result in hearing impairment, facial nerve paralysis, intracranial extension, and life-threatening complications. The present review-based observational study aimed to evaluate the epidemiology, clinical presentation, diagnostic approaches, histopathological patterns, and management outcomes of ear tumors among patients presenting to tertiary otorhinolaryngology centers. A retrospective analysis of 100 patients diagnosed with ear tumors over a five-year period was conducted using hospital medical records, imaging findings, histopathological reports, and treatment outcomes. Benign tumors constituted the majority of cases, with osteoma, exostosis, ceruminous adenoma, and glomus tumors being the most frequently identified lesions. Among malignant tumors, squamous cell carcinoma was the commonest histological subtype, followed by basal cell carcinoma and adenocarcinoma. The most common presenting symptoms were otorrhea, hearing loss, otalgia, tinnitus, and visible auricular swelling. Computed tomography and magnetic resonance imaging played a major role in assessing tumor extent and bony involvement. Surgical excision remained the cornerstone of management, while radiotherapy and chemotherapy were used in selected malignant cases. Early diagnosis and multidisciplinary management significantly improved prognosis and reduced complications. Awareness regarding clinical manifestations and appropriate diagnostic strategies is essential for MBBS students and clinicians to ensure timely intervention and better patient outcomes.
Keywords
Ear Neoplasms
External Auditory Canal Tumor
Glomus Tumor
Squamous Cell Carcinoma
Temporal Bone Neoplasms
Otorhinolaryngology
Introduction
Tumors of the ear are uncommon lesions that may arise from the auricle, external auditory canal, middle ear, or inner ear structures. These tumors may be benign or malignant and can originate from epithelial, neural, vascular, cartilaginous, or glandular tissues. Despite their rarity, ear tumors are clinically important because of their proximity to vital neurovascular and intracranial structures.
Benign tumors are more common than malignant lesions and include osteomas, exostoses, papillomas, ceruminous gland adenomas, hemangiomas, and glomus tumors. Malignant tumors include squamous cell carcinoma, basal cell carcinoma, adenocarcinoma, melanoma, sarcomas. Squamous cell carcinoma of the external auditory canal and temporal bone is the most frequently reported malignant ear tumor and is associated with significant morbidity and mortality.
The incidence of malignant tumor of the temporal bone is estimated to be approximately 1–6 cases per million population annually. Chronic otitis media, prolonged ultraviolet exposure, smoking, radiation exposure, and chronic inflammation are recognized risk factors for malignant ear tumor. In developing countries, delayed healthcare access and chronic ear infections contribute significantly to late presentation.
Clinical manifestations vary according to tumor location and extent. Common symptoms include hearing loss, otorrhea, otalgia, tinnitus, vertigo, facial nerve weakness, and bleeding from the ear. Because many symptoms mimic chronic ear infections, diagnosis is often delayed, leading to advanced disease at presentation.
Advances in imaging modalities such as HRCT and MRI have improved diagnostic accuracy and staging.Histopathological examination remains the gold standard for definitive diagnosis.
The rationale of this study is to provide a comprehensive academic review of ear tumors relevant to MBBS students, focusing on epidemiology, clinical presentation, diagnostic evaluation, histopathology, and management strategies. The objectives of this study are:
To classify tumors of the ear according to anatomical location and pathology.
To analyze clinical presentation and diagnostic methods.
To evaluate treatment modalities and outcomes.
To highlight the importance of early diagnosis and multidisciplinary management.
Methodology
Study Design
A retrospective observational review study was conducted using hospital-based medical records and published literature related to tumors of the ear.
Study Population
The study population included patients diagnosed with benign or malignant tumors involving the external ear, external auditory canal, middle ear, or temporal bone who attended tertiary ENT centers between January 2020 and December 2024.
Inclusion Criteria
Patients diagnosed histopathologically with ear tumors
Patients of all age groups and both sexes
Benign and malignant neoplasms of the ear
Complete clinical and radiological records available
Exclusion Criteria
Inflammatory ear polyps without neoplastic changes
Congenital ear anomalies
Incomplete medical records
Patients unwilling for biopsy or treatment
Data Collection Methods
Data were collected from:
Patient case records
ENT outpatient and inpatient registers
Histopathology reports
CT and MRI imaging reports
Operative notes and treatment records
The following variables were recorded:
Age and sex distribution
Clinical symptoms
Tumor location
Histopathological type
Imaging findings
Treatment modality
Outcome and complications
Statistical Analysis
Data were entered into Microsoft Excel and analyzed using SPSS software version 25. Descriptive statistics including frequency, percentages, mean, and standard deviation were used. Categorical variables were presented in tabular form.
Ethical Considerations
Institutional ethical approval was obtained before commencement of the study. Patient confidentiality was maintained, and all data were anonymized. The study adhered to the principles of the Declaration of Helsinki.
Results
Demographic Distribution
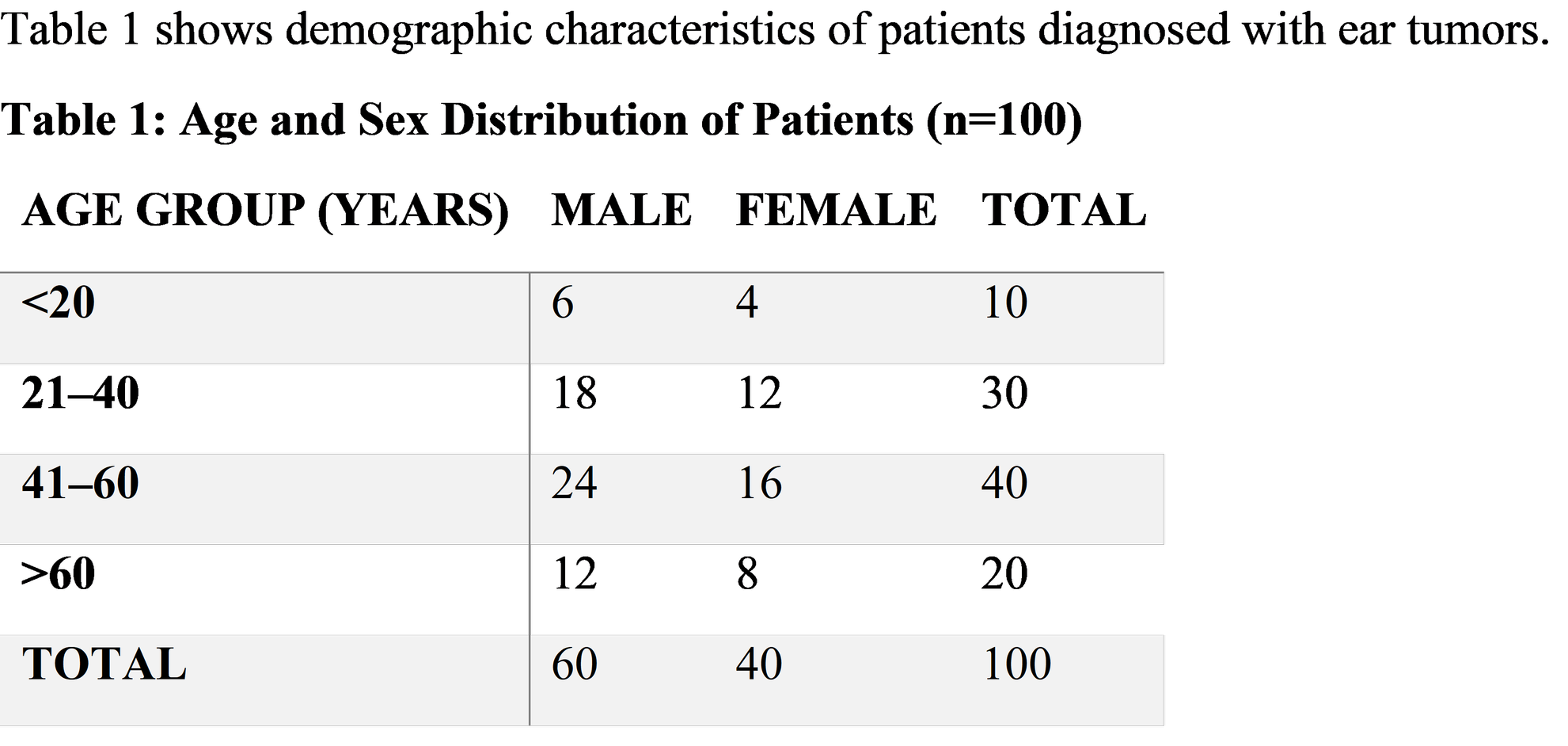
The majority of patients belonged to the 41–60 years age group, with males being more commonly affected.
Distribution of Tumor Types
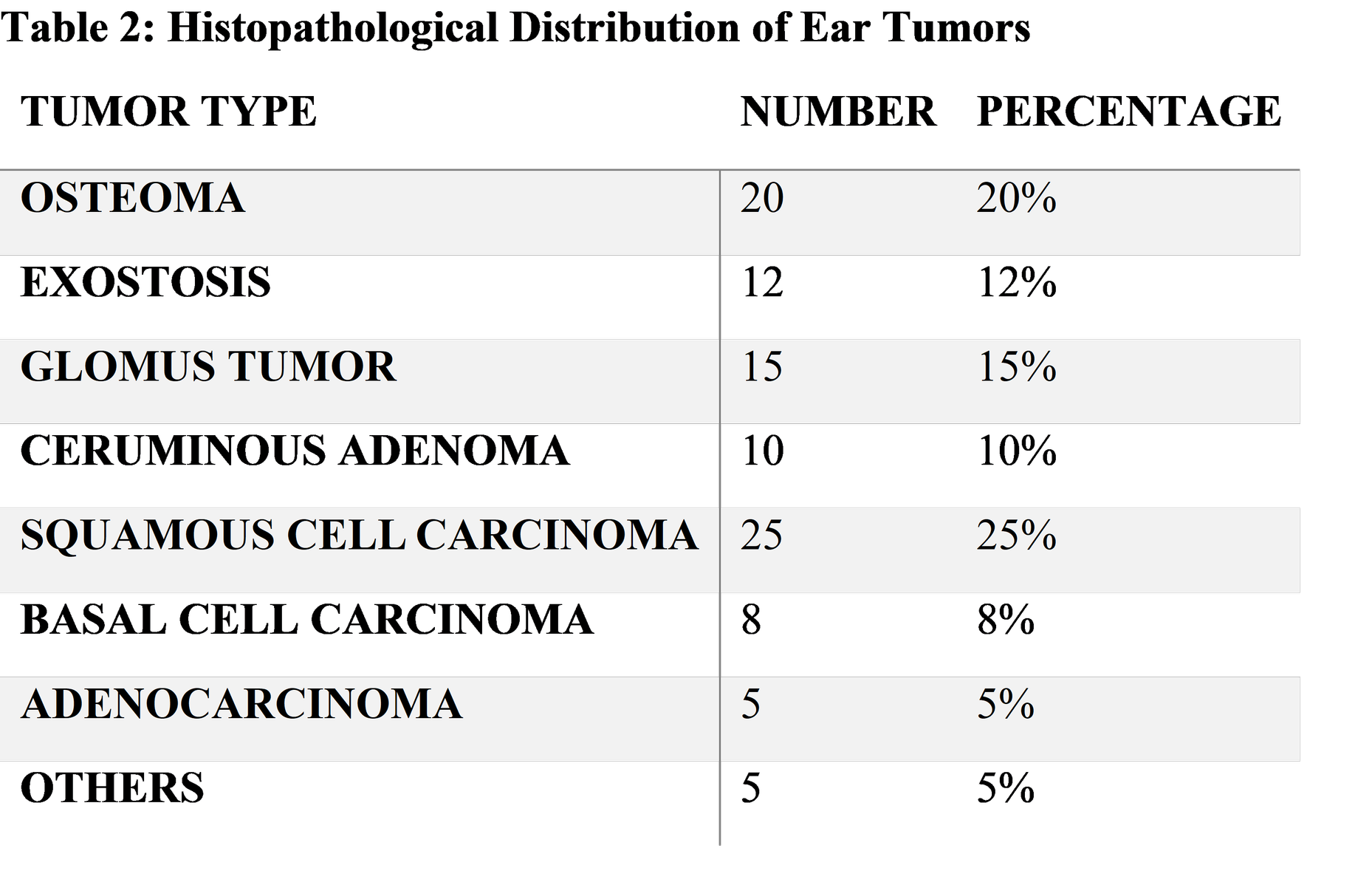
Squamous cell carcinoma was the most common malignant tumor, whereas osteoma was the commonest benign lesion.
Clinical Presentation
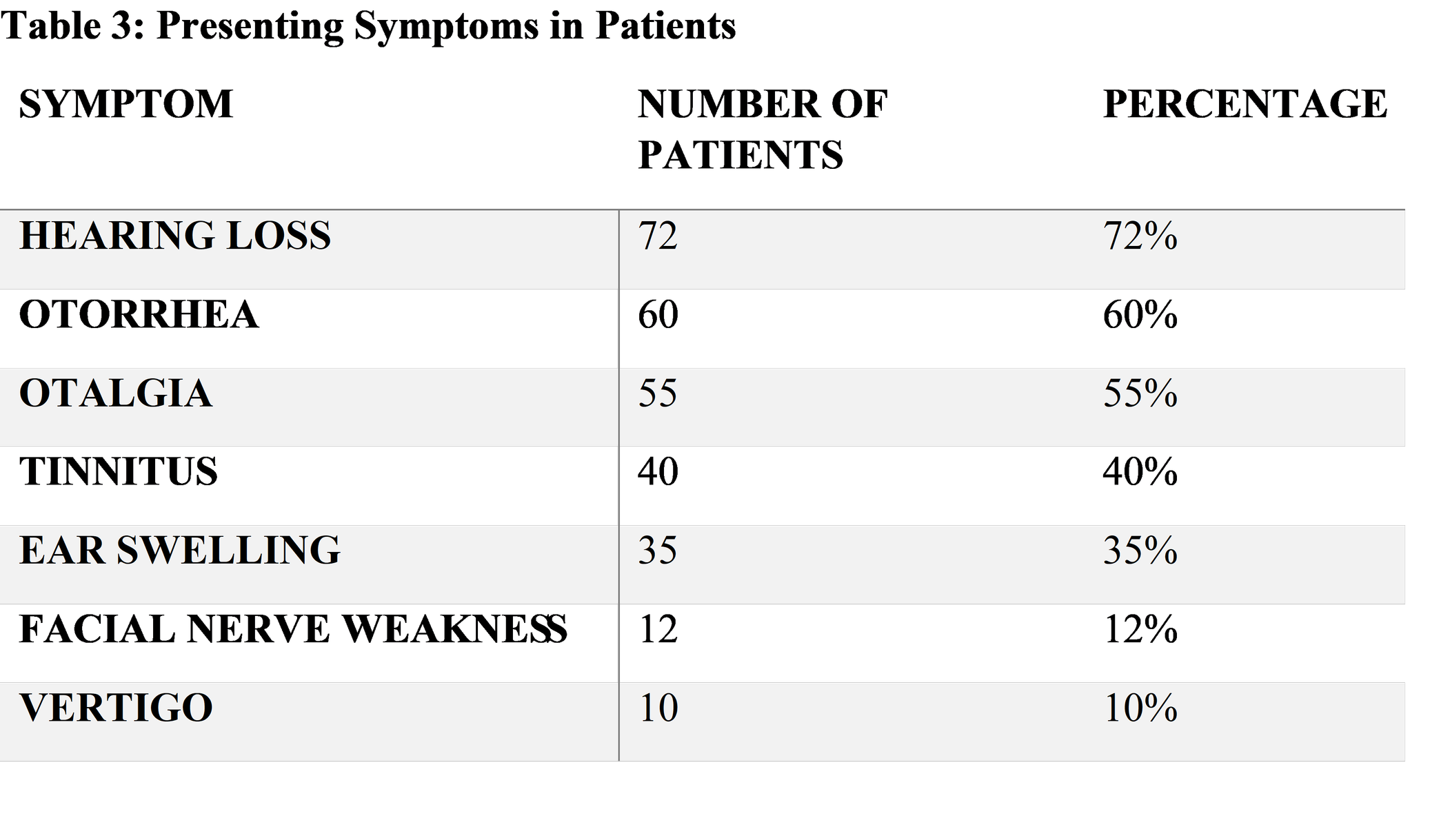
Hearing loss and chronic otorrhea were the most common presenting complaints.
Imaging Findings
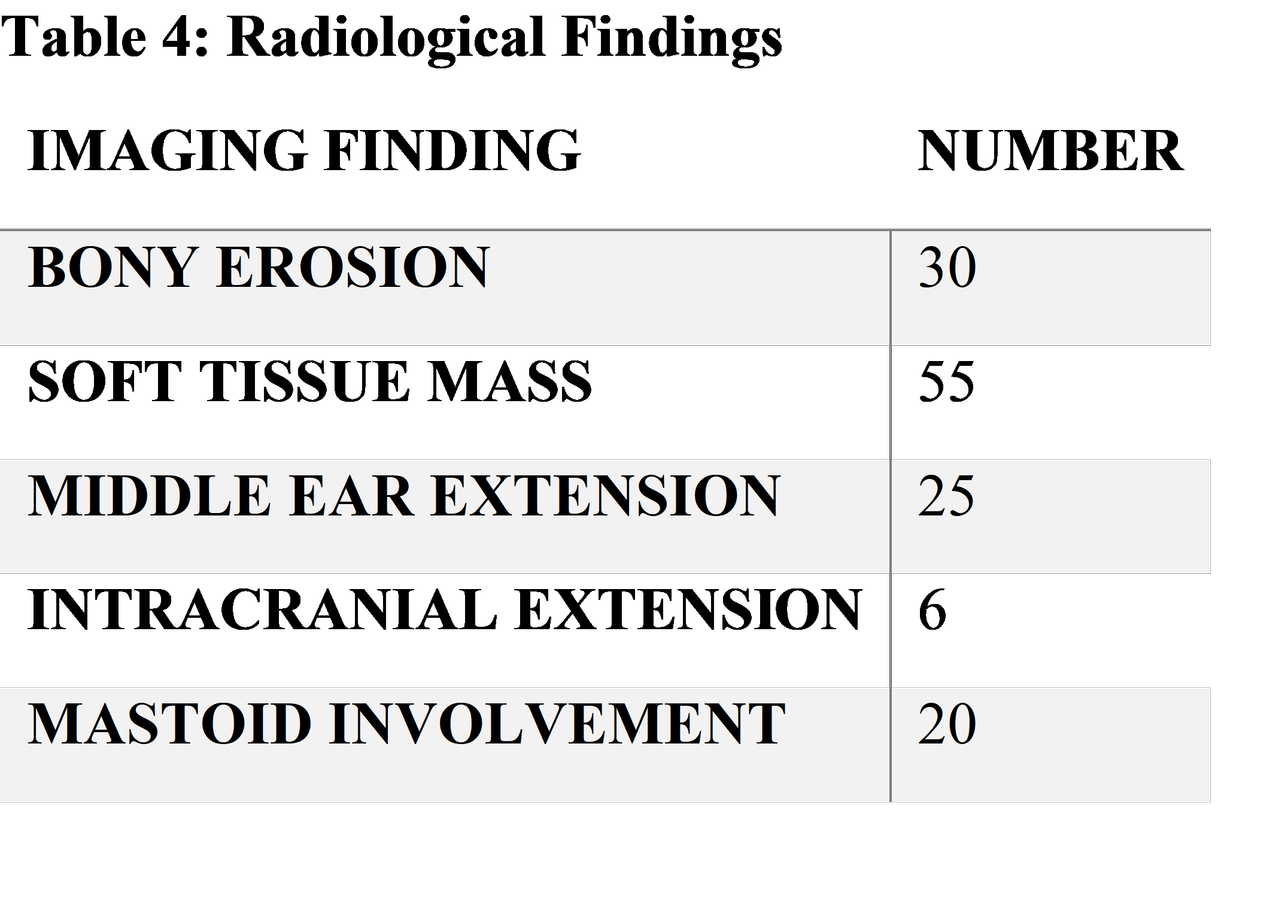
HRCT was particularly useful in evaluating bony destruction and temporal bone involvement.
Treatment Modalities
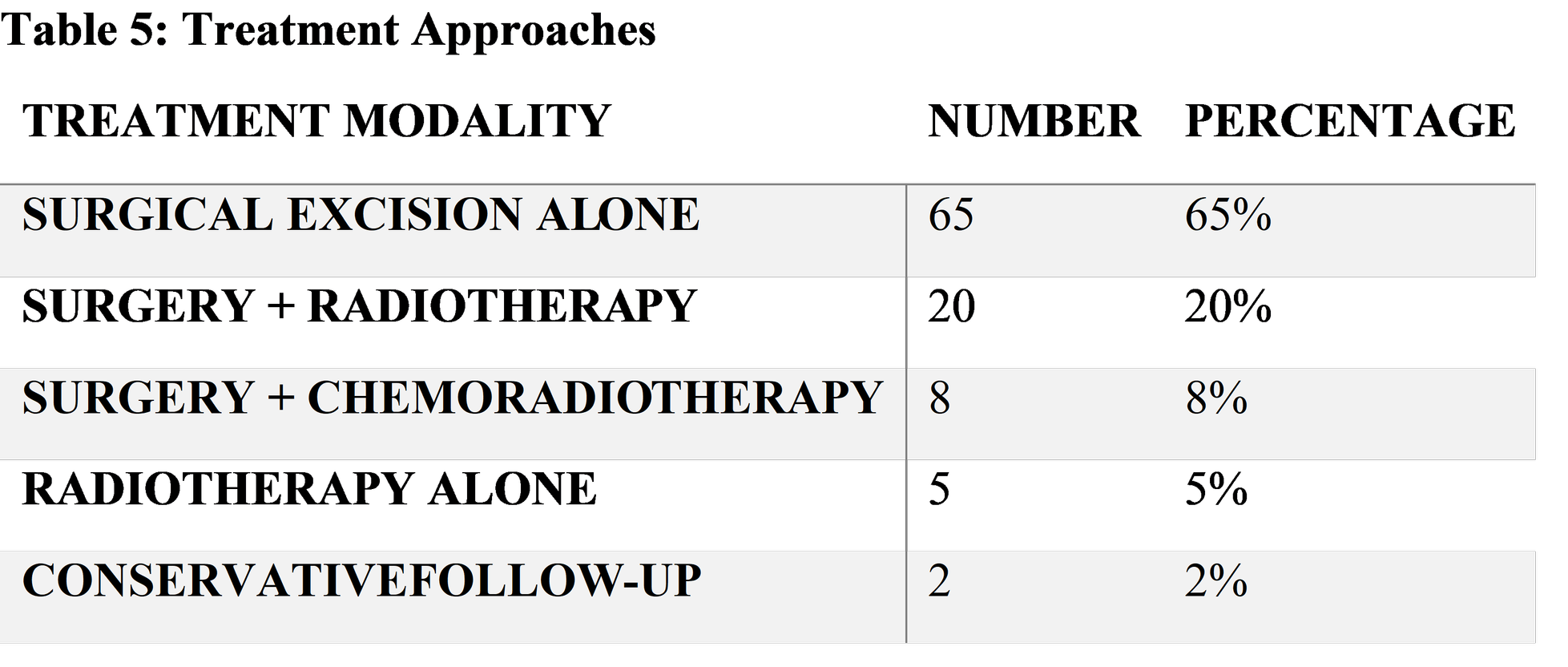
Surgical management was the primary treatment modality in most patients.
Discussion
Tumors of the ear are rare lesions with variable biological behavior ranging from indolent benign masses to highly aggressive malignancies. The present study demonstrated a higher prevalence among middle-aged and elderly individuals, particularly males, which is consistent with previous literature.
Benign tumors accounted for the majority of cases in this study. Osteomas and exostoses were frequently observed in the external auditory canal. Osteomas are solitary, pedunculated bony tumors, whereas exostoses are broad-based multiple bony outgrowths associated with repeated cold water exposure. These lesions may remain asymptomatic for years and are often discovered incidentally.
Glomus tumors represented a significant proportion of vascular neoplasms identified in this study. Glomus tympanicum and glomus jugulare tumors arise from paraganglionic tissue and commonly present with pulsatile tinnitus and conductive hearing loss. MRI is particularly useful in identifying the characteristic “salt and pepper” appearance due to hypervascularity.
Squamous cell carcinoma emerged as the most common malignant tumor in the present analysis. SCC of the temporal bone is highly aggressive and often diagnosed late because symptoms mimic chronic suppurative otitis media. Persistent otorrhea, otalgia, bleeding, and facial paralysis should raise suspicion for malignancy.
The predominance of hearing loss and otorrhea among presenting symptoms observed in this study is similar to findings reported by Moody et al. Facial nerve weakness was associated with advanced disease and poorer prognosis.
Imaging plays a critical role in diagnosis and staging. HRCT effectively demonstrates cortical bone destruction, while MRI better delineates soft tissue extension and intracranial spread. Combined imaging approaches improve surgical planning and prognostic assessment.
Histopathological confirmation remains essential for definitive diagnosis. Biopsy should be performed carefully in vascular tumors such as glomus tumors because of bleeding risk.
Surgical excision was the primary treatment modality in this study. Benign tumors generally have excellent outcomes following complete removal. Malignant tumors often require aggressive surgical resection combined with postoperative radiotherapy. Advanced SCC may necessitate subtotal temporal bone resection and neck dissection.
Radiotherapy is beneficial in unresectable tumors, residual disease, and paragangliomas. Chemotherapy is generally reserved for advanced or metastatic disease.
Early diagnosis substantially improves prognosis. Delayed presentation is associated with local invasion, intracranial complications, and reduced survival rates. Public awareness and improved ENT screening are therefore important preventive strategies.
Suggestions / Recommendations
Early ENT evaluation should be encouraged in patients with chronic unilateral otorrhea or hearing loss.
Persistent ear discharge not responding to antibiotics must undergo biopsy to exclude malignancy.
HRCT and MRI should be used for accurate staging and surgical planning.
Multidisciplinary management involving ENT surgeons, radiologists, pathologists, and oncologists improves outcomes.
Public education regarding chronic ear disease and sun protection may reduce risk factors.
Regular follow-up is essential to detect recurrence, especially in malignant tumors.
Further multicenter prospective studies are recommended to evaluate long-term survival and treatment outcomes.
Conclusion
Tumors of the ear comprise a diverse group of benign and malignant neoplasms affecting the external ear, middle ear, and temporal bone. Although rare, these tumors are clinically significant because delayed diagnosis may lead to serious complications including hearing loss, facial nerve paralysis, and intracranial spread. Benign tumors such as osteomas and glomus tumors are more common, while squamous cell carcinoma represents the predominant malignant lesion. Clinical suspicion, imaging studies, and histopathological confirmation are essential for accurate diagnosis. Surgical excision remains the cornerstone of treatment, often combined with radiotherapy in malignant cases. Early detection and multidisciplinary management significantly improve prognosis and quality of life.
References
Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology Head and Neck Surgery. 7th ed. Philadelphia: Elsevier; 2021.
Gleeson M. Scott-Brown’s Otorhinolaryngology Head and Neck Surgery. 8th ed. London: CRC Press; 2018.
Myers EN, Ferris RL. Salivary Gland Disorders. Berlin: Springer; 2017.
Moody SA, Hirsch BE, Myers EN. Squamous cell carcinoma of the external auditory canal: an evaluation of a staging system. Am J Otol. 2000;21(4):582-588.
Prasad SC, D’Orazio F, Medina M, et al. State of the art in temporal bone malignancies. Curr Opin Otolaryngol Head Neck Surg. 2014;22(2):154-165.
Zanoletti E, Marioni G, Stritoni P, et al. Temporal bone squamous cell carcinoma: analyzing prognosis with univariate and multivariate models. Laryngoscope. 2014;124(5):1192-1198.
World Health Organization. Chronic suppurative otitis media: burden of illness and management options. Geneva: WHO; 2004.
Selesnick SH, Jackler RK. Clinical manifestations and diagnosis of temporal bone tumors. Otolaryngol Clin North Am. 2001;34(6):1143-1164.
Morris LG, Mehra S, Shah JP, et al. Predictors of survival and recurrence after temporal bone resection for cancer. Head Neck. 2012;34(9):1231-1239.
Mafee MF, Levin BC, Applebaum EL. Imaging of temporal bone tumors. Radiol Clin North Am. 1993;31(1):175-201.
Rosai J. Rosai and Ackerman’s Surgical Pathology. 11th ed. Philadelphia: Elsevier; 2018.
Paparella MM, Shumrick DA. Otolaryngology. 4th ed. Philadelphia: Saunders; 2016.
Pensak ML. Controversies in temporal bone carcinoma. Otolaryngol Clin North Am. 2006;39(6):1087-1102.
Swartz JD. Lesions of the external auditory canal. Radiol Clin North Am. 1984;22(1):15-24.
Kutz JW Jr, Husain IA, Isaacson B, et al. Management of external auditory canal osteomas and exostoses. Otol Neurotol. 2007;28(7):920-924.
Jackson CG, Glasscock ME, Harris PF. Glomus tumors: diagnosis, classification, and management. Laryngoscope. 1982;92(4):401-410.
Carlson ML, Sweeney AD, Pelosi S, et al. Glomus tympanicum: a review of 115 cases. Otol Neurotol. 2015;36(5):859-865.
Masterson L, Rouhani M, Donnelly NP, et al. Squamous cell carcinoma of the temporal bone: clinical outcomes. J Laryngol Otol. 2014;128(12):1068-1072.
Arriaga MA, Curtin H, Takahashi H, et al. Criteria for diagnosis and staging of external auditory canal carcinoma. Otolaryngol Head Neck Surg. 1990;103(5):714-720.
Moody SA, Hirsch BE, Myers EN. Squamous cell carcinoma of the external auditory canal. Am J Otol. 2000;21(4):582-588.
Nakagawa T, Kumamoto Y, Natori Y, et al. Squamous cell carcinoma of the external auditory canal and middle ear. Arch Otolaryngol Head Neck Surg. 2006;132(8):847-851.
Som PM, Curtin HD. Head and Neck Imaging. 5th ed. St. Louis: Mosby; 2011.
Curtin HD, Hirsch BE. Imaging of ear tumors. Neuroimaging Clin N Am. 2009;19(3):397-412.
Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 10th ed. Philadelphia: Elsevier; 2020.
Fisch U, Mattox D. Microsurgery of the Skull Base. Stuttgart: Thieme; 1988.
Lalwani AK. Current Diagnosis and Treatment in Otolaryngology. 4th ed. New York: McGraw-Hill; 2020.
Moffat DA, Wagstaff SA, Hardy DG. Surgical management of temporal bone tumors. Skull Base Surg. 2005;15(2):85-92.
Prasad SC, Piccirillo E, Chiesa Estomba CM, et al. Surgical strategies in temporal bone malignancy. Auris Nasus Larynx. 2020;47(3):325-333.
Hinerman RW, Amdur RJ, Morris CG, et al. Radiotherapy for paraganglioma of the temporal bone. Head Neck. 2008;30(11):1431-1438.
National Comprehensive Cancer Network. Head and Neck Cancers Guidelines. Version 2024.
Gillespie MB, Francis HW, Chee N, et al. Squamous cell carcinoma of the temporal bone. Otolaryngol Head Neck Surg. 2001;124(6):706-714.
Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat. 8th ed. New Delhi: Elsevier; 2022.