
Anatomical and Functional Analysis of The Twelve Cranial Nerves with Clinical Correlations
1. Zarina Zhamaldinovna Toichieva
2. Thirushanth Ramesh
3. Jothi Basu Kasinathan
4. Priyadharshini Ramesh
(1. Lecturer, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
2. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
3. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic
4. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
The twelve cranial nerves form a vital part of the peripheral nervous system, responsible for diverse sensory, motor, and autonomic functions. The nerves arise from specific nuclei in the brain stem and forebrain, supplying highly specialized innervations to structures in the head, neck, and visceral organs. The current review provides a comprehensive analysis of the anatomical course, functional modes, embryonic development, and clinical relevance of each cranial nerve. Special attention is paid to their integration, crucial for neuroanatomy and lesion localization in clinical medicine.
Keywords: The cranial nerves, neuroanatomy, brainstem nuclei, innervation, sensory and motor pathways, the parasympathetic nervous system, the trigeminal nerve, the facial nerve, the vagus nerve, the oculomotor nerve, disorders of the cranial nerves, neurologic examination, head and neck, the peripheral nervous system, and clinical neuroanatomy.
Introduction
Cranial nerves are special neural structures derived from the brain as opposed to spinal nerves which originate from the spinal cord. They act as major channels for transmission of impulses between the brain and its peripheral parts. Functions of these nerves range from sensing organs (vision, auditory, gustatory, olfactory sensations), muscular movement, and autonomic functions. The nuclei of cranial nerves are located mainly in the brain stem (midbrain, pons, and medulla). The function of these nerves is grouped into fiber components like:
General somatic efferent (GSE) General somatic afferent (GSA) Special visceral afferent (SVA) General visceral efferent (GVE), etc.
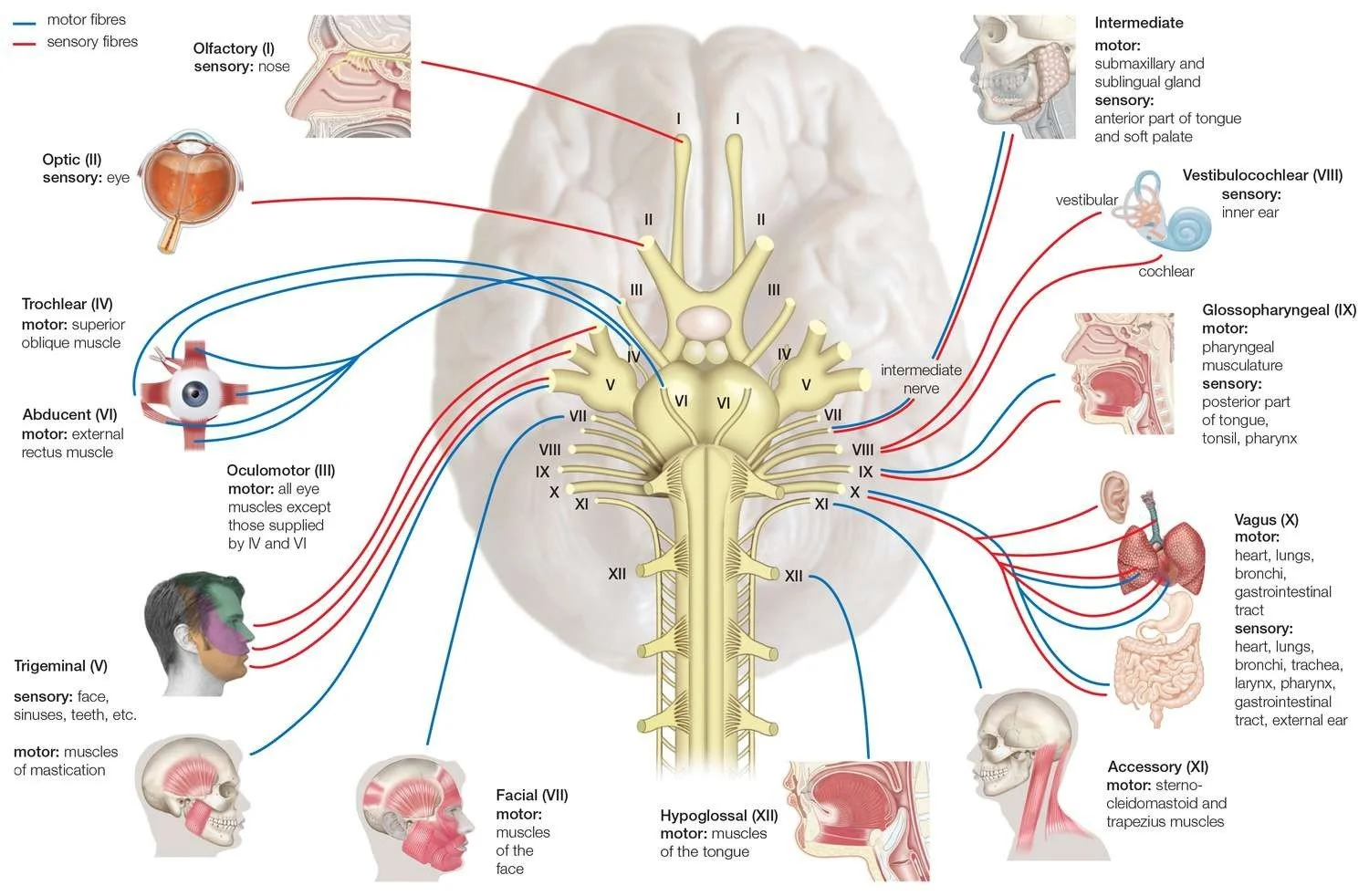
Embryological and Functional Classification
The cranial nerves are derived from the neural crest and placodes. Based on their function, they can be classified into the following categories:
Sensory Cranial Nerves
1.I Olfactory
2.II Optic
3.VIII Vestibulocochlear
Motor Cranial Nerves
1.III Oculomotor
2.IV Trochlear
3.VI Abducens
4.XI Accessory
5.XII Hypoglossal
Mixed Cranial Nerves
1.V Trigeminal
2.VII Facial
3.IX Glossopharyngeal
4.X Vagus
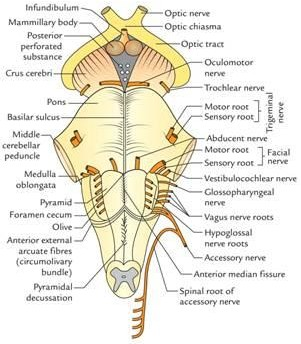
Detailed Cranial Nerve Anatomy and Innervation
I. Olfactory Nerve (CN I)
The olfactory nerve serves as the organ of smell and is an extension of the brain. Receptors: Bipolar cells within olfactory mucosa
Tract: Olfactory filaments → Cribriform plate → Olfactory bulb → Olfactory tract Nerve supply: Mucous membrane of nose (olfactory area)
Clinical Significance: Results in anosmia; earliest symptom of neurodegeneration
II. Optic Nerve (CN II)
The optic nerve carries impulses for vision from the retina to the brain. Source: Ganglion cells of retina
Course: Optic nerve → optic chiasm → optic tract → lateral geniculate nucleus → visual cortex Unique Attribute: Partial crossing at chiasm
Medical Significance: Lesion leads to specific field defects
III. Oculomotor Nerve (CN III)
A mixed nerve containing somatic and autonomic fibers. Ganglia: Ciliary ganglion
Roots: Oculomotor nerve roots Supply:
Oculomotor nerve (cranial nerve III) Ciliary ganglion
Levator palpebrae superioris muscle Intrinsic muscles of eyeball
Parasympathetic supply to pupillary sphincter and ciliary body
IV. Trochlear Nerve (CN IV)
The smallest cranial nerve, unique for dorsal emergence. Innervation: Superior oblique muscle
Function: Depression and intorsion of the eyeball
Clinical Note: Vertical diplopia, difficulty walking downstairs.
V. Trigeminal Nerve (CN V)
Largest cranial nerve with broad distribution of sensory nerves. Branches: V1 – Ophthalmic V2 – Maxillary V3
Mandibular Nerve Supply:
Sensory: Face, scalp, cornea, nasal cavity Motor: Mastication muscles
Clinical Significance: Trigeminal
VI. Abducens Nerve (CN VI)
Controls lateral eye movement.
● Innervation: Lateral rectus muscle
● Clinical Note: Lesion causes medial deviation (esotropia)
VII. Facial Nerve (CN VII)
A very complicated mixed nerve, performing several functions. Structures:
Branchiomotor component (for facial expression) Parasympathetic fiber (innervating glands)
Sensory (taste from the anterior two-thirds of the tongue) Nerve Supply:
Muscles of facial expression
Lacrimal gland, submandibular gland, sublingual
VIII. Vestibulocochlear Nerve (CN VIII)
Essential for hearing and balance.
● Divisions: Vestibular and cochlear
● Innervation: Inner ear sensory receptors
● Clinical Note: Lesions cause vertigo, hearing loss
IX. Glossopharyngeal Nerve (CN IX)
Plays roles in taste, swallowing, and autonomic function.
● Innervation:
○ Stylopharyngeus muscle
○ Parotid gland (via optic ganglion)
○ Posterior 1/3 tongue
● Clinical Note: Loss of gag reflex
X. Vagus Nerve (CN X)
The most extensive cranial nerve with widespread visceral innervation.
● Innervation:
○ Pharynx, larynx
○ Heart, lungs, gastrointestinal tract
● Function: Parasympathetic regulation
● Clinical Note: Hoarseness, dysphagia
XI. Accessory Nerve (CN XI)
Controls major neck muscles.
● Innervation: Sternocleidomastoid and trapezius
● Clinical Note: Shoulder droop, weak head rotation
XII. Hypoglossal Nerve (CN XII)
Controls tongue movements.
● Innervation: Intrinsic and extrinsic tongue muscles
● Clinical Note: Tongue deviates toward side of lesion
Cranial Nerve Nuclei Organization
Cranial nerve nuclei are arranged longitudinally in the brainstem:
● Medial: Motor nuclei
● Lateral: Sensory nuclei
This organization is clinically relevant in brainstem lesions.
Clinical Examination of Cranial Nerves
Systematic examination involves: CN I: Smell test
CN II: Visual acuity, visual field-testing CN III, IV, VI: Ophthalmologic test
CN V: Sensation of face, chewing CN VII: Facial expressions
CN VIII: Hearing test (Rinne test, Weber test) CN IX, X: Gag reflex
CN XI: Shrugging shoulders CN XII: Tongue movements
Discussion
Cranial nerves show a complex anatomical course and multifunctionality. Due to their association with the brain stem, they form important indicators for localization in neurology. However, thanks to progress in neurophysiology and radiology, our knowledge about them is better understood.
Conclusion
The twelve pairs of cranial nerves are very important in sensory reception, motor skills, and autonomic functions. It is imperative to understand their anatomical features and innervations in order to diagnose neurological diseases. The understanding of these is the basis of clinical neurology.
References
1. Standring S, ed. Gray’s Anatomy. 42nd ed. Elsevier; 2020.
2. Snell RS. Clinical Neuroanatomy. 8th ed. Wolters Kluwer; 2019.
3. Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 8th ed. Wolters Kluwer; 2018.
4. Blumenfeld H. Neuroanatomy Through Clinical Cases. 2nd ed. Sinauer; 2010.
5. Kiernan JA. Barr’s The Human Nervous System. 10th ed. Lippincott Williams & Wilkins; 2014.