
Liver Abscess
1. Kaiypov Abdumazhit
2. Rochelle Netto
Md Reyaz Alam
Het Patel
(1. Teacher, Surgery Dept., International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
The condition of liver abscess (LA) causes persistent health problems and death rates in all regions of the world despite improved methods for medical imaging and treatment. This review provides a complete overview of current knowledge about pyogenic and amebic liver abscesses which include information about changing disease patterns and rising cases of hypervirulent Klebsiella pneumoniae and changes to treatment methods which now use less invasive procedures instead of traditional surgery. The study examines all aspects of the condition which include its causes and disease process and patient symptoms and methods for diagnosing and treating the illness while using new information about percutaneous drainage and aspiration methods. The review reveals how different parts of the world experience different rates of occurrence while showing how teamwork between different health professions helps decrease the high death rates that result from septic complications.
Keywords: Pyogenic Liver Abscess, Klebsiella pneumoniae, Hypervirulent, Percutaneous Drainage, Amebic Liver Abscess.
Introduction
A liver abscess is defined as a collection of purulent material within the liver parenchyma which occurs due to bacterial and parasitic and fungal infections. Hepatic suppuration has existed as a medical condition since Hippocrates first described it, but patients affected by this condition had no chance of survival during the pre-antibiotic period. The introduction of surgical drainage in the 20th century failed to decrease the death rate which remained between 60% and 80%. The disease has undergone substantial changes during the last thirty years. The development of cross-sectional imaging, the improvement in microbiological identification techniques, and the shift toward percutaneous, minimally invasive drainage have reduced mortality rates to between 5% and 30%.
The rate of liver abscess occurs at a consistent level despite improved diagnostic methods because the condition presents itself to doctors in a gradual manner. The disease has experienced a major shift in its microbiological profile which now develops across different geographic areas and various disease stages. The primary cause of the disease evolved from portal pyeimia which resulted from appendicitis to its current state, in which biliary tract disease predominates in Western countries and hypervirulent Klebsiella pneumoniae causes most cases in Asia. The review presents clinically useful information about liver abscess through current research which examines its pathogenesis and diagnostic procedures and evidence-based treatment methods, while especially focusing on how percutaneous treatments work and how multidrug-resistant organisms emerged.
Methods
The IMRAD structure was used to build this narrative review because it helped create a scientific and logical structure for the presentation of research findings. The researchers performed a complete literature search using three databases which included PubMed and the Cochrane Library and Google Scholar. Search terms included “pyogenic liver abscess” “amebic liver abscess” “Klebsiella pneumoniae liver abscess” “percutaneous drainage” and “liver abscess epidemiology.”
The study focused on works published between 2015 and 2025 while also considering important historical texts and the latest meta- analyses. The researchers used data from peer-reviewed research articles and major textbooks (Practical Internal Medicine) and reliable clinical websites (BMJ Best Practice, Medscape, StatPearls) to create a comprehensive overview of current standard medical practices.
Epidemiology
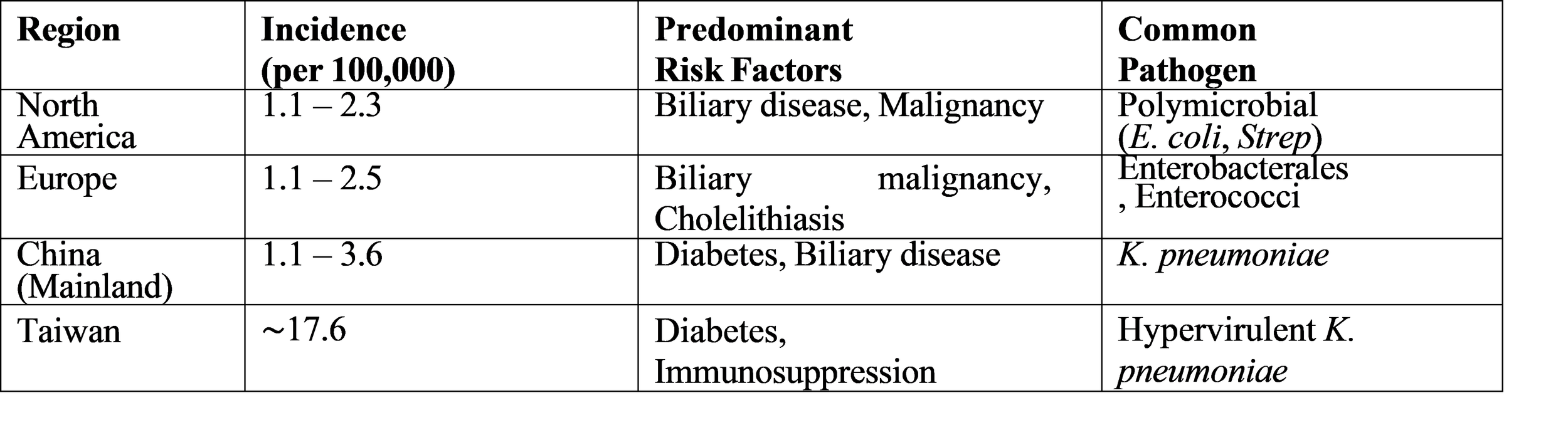
The global occurrence of liver abscesses shows considerable differences between different regions of the world. North America and Europe have an annual rate of pyogenic liver abscess (PLA) that ranges between 1.1 and 2.3 cases for every 100,000 people. However, Asian countries report much higher incidence rates. Taiwan shows an incidence rate of 17.6 per 100,000 people while mainland China has rates between.
1.1 and 3.6 per 100,000 people. A tertiary-care hospital in Germany conducted a study which found that patients had an average age of 63 years and most of them (63%) were male.
Table 1: Global Incidence and Key Risk Factors
Etiology and Microbiology
The percentage of cases which appendicitis used to cause liver abscesses has decreased to less than 10 percent because doctors now diagnose and treat the condition more effectively. The biliary tract disease which includes cholangitis and cholelithiasis and malignant obstruction has become the most frequent cause of diseases which affect approximately 60 percent of patients according to some medical studies.
Microbial Spectrum
The microbiology of PLA shows distinct polymicrobial characteristics but displays an epidemiological shift which has transformed its current status. The common pathogens in this region include Escherichia coli and other Enterobacteriaceae but Klebsiella pneumoniae currently stands as the primary infectious agent which affects people especially throughout Asia. The German cohort study conducted between 2013 and 2019 identified 58 percent of patients with Enterobacterales and 42 percent with enterococci and 18 percent with streptococci which demonstrates the presence of multiple bacterial types in Western populations.
The hypervirulent K. pneumoniae (hvKp) strain represents a dangerous threat to public health. HvKp causes infections which healthy people can contract from the community while classic K. pneumoniae causes hospital-acquired infections. The “liver abscess invasive syndrome” which leads to endophthalmitis and meningitis and fasciitis develops when hvKp causes infections. The development of invasive infections gets accelerated when patients with diabetes mellitus develop comorbid conditions.
The detection of Desulfovibrio desulfuricans and other rare pathogens demonstrates that advanced microbiological diagnostic methods which include MALDI-TOF MS are necessary for detecting uncommon anaerobic pathogens who possess unexpected antibiotic resistance.
Clinical Presentation and Diagnosis
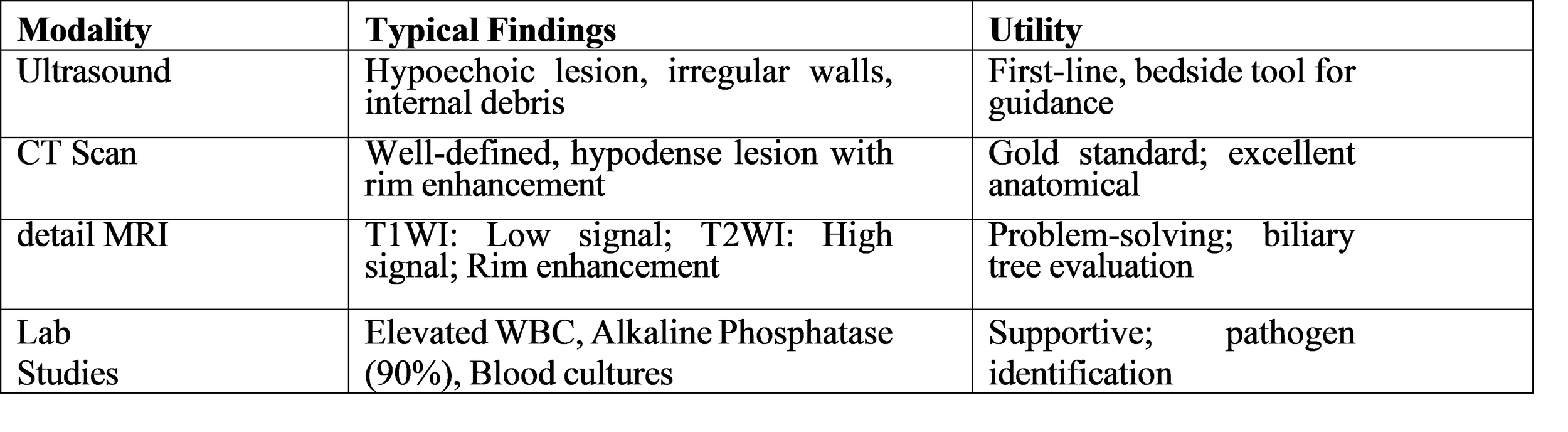
The clinical presentation of liver abscess shows extreme variability which results in diagnostic delays. The classic triad of fever, right upper quadrant pain, and jaundice (Charcot’s triad) is more suggestive of cholangitis, though liver abscess remains a key differential. Fever is the most consistent symptom which occurs in 90% of patients and frequently comes with chills and night sweats.
Diagnostic Imaging
The first imaging test which doctors use is ultrasound because of its easy access and safety from radiation exposure. The test shows a hypoechoic or anechoic lesion which has clear boundaries. The doctor uses contrast-enhanced computed tomography (CT) as the standard method to make medical diagnoses and create treatment plans. CT imaging enables accurate measurement of abscesses because it shows their complete size and total number and exact location. The test shows the “double target sign” or “cluster sign” which displays multiple tiny abscesses that combine to create a larger space.
Table 2: Diagnostic Findings in Liver Abscess
Treatment Modalities and Outcomes
The treatment of liver abscess requires two essential components which include delivering antibiotics and performing drainage procedures.
Antimicrobial Therapy
The medical team must begin broad-spectrum antibiotic treatment after they complete blood culture tests. The standard treatment includes a third-generation cephalosporin (for example ceftriaxone) together with metronidazole which provides coverage against both anaerobic bacteria and amebic infections. Patients who have diabetes or who recently stayed in a hospital should receive treatment with a carbapenem because they face the danger of infection from ESBL-producing bacteria. The total duration of therapy lasts from 4 to 6 weeks which starts with 2 to 4 weeks of intravenous treatment that continues until the patient shows clinical improvement because medical practitioners will use clinical signs to assess progress instead of imaging tests which show slower results.
Interventional Management
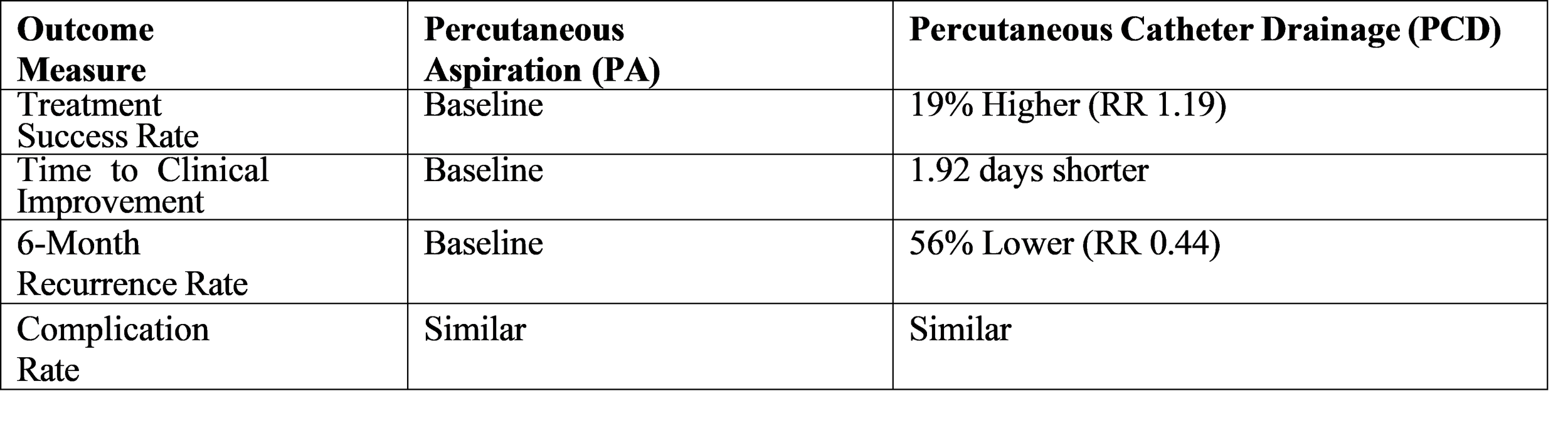
The medical field used open surgical drainage as its primary treatment method until the last forty years. The medical field now considers percutaneous catheter drainage (PCD) as the primary treatment method for abscesses that require surgical intervention and have dimensions greater than three centimeters.
A systematic review and meta-analysis conducted in 2025 studied the effectiveness of percutaneous aspiration (PA) compared to percutaneous catheter drainage (PCD) and produced strong evidence which helps doctors make treatment decisions. The research analyzed 1,290 participants and found that PCD provides better results than PA across multiple important medical measures. The data demonstrates that doctors believe simple aspiration works for smaller abscesses but larger abscesses require continuous catheter drainage to achieve complete evacuation and stop re-accumulation.
Outcomes
The mortality rate from liver abscess remains high even when patients receive their best possible medical treatment. The research showed that 80 percent of the 150 studied patients achieved complete recovery.
While their mortality rate reached 3.3 percent and 13.3 percent of the patients developed septicemia as a complication [3]. The existence of underlying cancer in patients leads to their poor long-term medical outcomes. A German study found that 30-day mortality rates remained constant between patients with malignancy and those without it (14.6% vs. 14.4%) but the one-year mortality rate for the malignancy group was much higher (58.4% vs. 29.6%) [9]. The development of positive blood cultures together with Enterobacterales detection serves as a key factor that leads to higher 30-day mortality rates.
Discussion
The synthesized data from this review shows that the typical liver abscess patient now has a different pro- file than before. The healthcare system has changed because doctors now provide immediate treatment for intra-abdominal infections while the population base has grown older thus creating a new patient demographic which includes elderly individuals with biliary disorders and diabetes. The growing dominance of hypervirulent Klebsiella pneumoniae as a major pathogen throughout Asia presents an urgent public health problem. The condition requires doctors to suspect endophthalmitis when their diabetic patients develop fever and visual problems because the disease can lead to severe metastatic infections.
Recent meta-analyses provide strong evidence which supports the existing treatment model that recommends percutaneous catheter drainage as superior to both simple aspiration and primary surgical procedures [4]. The procedure of percutaneous catheter drainage (PCD) stands as the preferred option for most patients because it achieves better treatment results and faster patient recovery times while reducing treatment recurrence. The method of continuous passive drainage establishes a better physiologic drainage system for enclosed spaces than the method of intermittent active aspiration. The implementation of these techniques should occur through a systematic approach because they do not function as exclusive options. Surgery maintains its essential function when doctors treat patients whose percutaneous drainage methods have failed or who possess multilocalated abscesses that require surgical intervention for intra-abdominal diseases.
The ongoing high mortality rates demonstrate that liver abscesses indicate severe comorbid conditions which result in high one-year mortality rates for patients who have cancer. Therefore, a diagnosis of PLA should trigger a thorough investigation for occult biliary or colonic pathology, particularly in older patients.
Conclusion
Liver abscesses continue to present dangerous medical challenges which require health professionals to maintain high suspicion levels for proper disease identification. The current medical landscape has evolved from its previous focus on appendicitis toward an era which centers on biliary diseases together with highly virulent strains of Klebsiella pneumoniae. The effective treatment process requires multiple specialists to start broad-spectrum antibiotic treatment while performing immediate imaging studies to achieve complete elimination of the infection source. The available evidence clearly demonstrates that percutaneous catheter drainage serves as the primary treatment method because it surpasses needle aspiration in both effectiveness and patient safety. The upcoming studies need to develop quick testing methods which will detect hypervirulent bacterial strains while they should establish effective antibiotic treatment plans against the rising threat of antimicrobial resistance. The presence of liver abscess requires medical professionals to conduct complete assessments which will detect hidden cases of liver and colorectal cancers because these conditions lead to poor long-term results.
References
[1] Jiang, W. (2022). Liver Abscess. In Practical Internal Medicine (16th ed.). People’s Medical Pub- lishing House.
[2] StatPearls. (2025). Liver Abscess. In StatPearls [Internet]. StatPearls Publishing. Available from: NCBI Bookshelf.
[3] Treatment and outcomes of patients (n=150) with a liver abscess. (2025). PMC.
[4] Li, X. F., et al. (2025). Comparative analysis of percutaneous aspiration and percutaneous catheter drainage for the treatment of liver abscess: A systematic review and meta-analysis. Medicine, 104(37), e44465.
[5] An unusual presentation of neutropenic enterocolitis (typhlitis). (2016). The Lancet Infectious Dis- eases.
[6] Flynn, J. E. (1946). Pyogenic Liver Abscess — Review of the Literature and Report of a Case Successfully Treated by Operation and Penicillin. The New England Journal of Medicine, 234, 403- 407.
[7] Peralta, R. (2024). Liver Abscess. Medscape. Updated Sep 03, 2024.
[8] Simmons, R. P., & Friedman, L. S. (2024). Liver abscess. BMJ Best Practice. Last updated Oct 31, 2024.
[9] Wendt, S., Bačák, M., Petroff, D., et al. (2024). Clinical management, pathogen spectrum and out- comes in patients with pyogenic liver abscess in a German tertiary-care hospital. Scientific Reports, 14(1).
[10] Huang, K. X., et al. (2025). Desulfovibrio desulfuricans bacteriaemia and associated liver abscess: Case report and literature review. Anaerobe, 102973.