
Pancreatitis-Acute and Chronic
1. Kaiypov Abdumazhit
2. Valiyarapadam Salam Almaas
Jasmine Abina
James Hanna
(1. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
ABSTRACT
An inflammatory process involving the pancreas, known as pancreatitis, can be categorized as either acute or chronic and may present in one of many ways. The clinical manifestations of acute pancreatitis are generally limited to epigastric or right upper quadrant pain, while manifestations of chronic pancreatitis are broader and may include abdominal pain in tandem with signs and symptoms of pancreatic endocrine and exocrine insufficiency. An understanding of the initial insult, proper classification, and prognosis are all factors that are of paramount importance as it pertains to managing patients who are afflicted with this disease. Our review delves into the depths of pancreatitis by exploring the embryology and anatomy of the pancreas, the pathophysiology and etiology of acute and chronic pancreatitis, and the medical and surgical management of acute and chronic pancreatitis.
Keywords: pancreatitis, surgery, surgical management of pancreatitis, pancreas disease, pancreatitis causes
INTRODUCTION
Pancreatitis is a pathology with many underlying facets. Understanding pancreatitis requires a grasp of anatomical, physiological, and pathological elements, while also requiring an appreciation for its two broad forms of existence and its many forms of management. Although medical management tends to be the initial stay of treatment for uncomplicated pancreatitis, there are still indications for surgical management. As time has progressed, newfound literature and studies have led to advancements and innovations that have changed the direction of surgical treatment, steering away from open surgical procedures, and more toward minimally invasive procedures that yield similar outcomes while still maintaining a strong level of efficacy. Pancreatitis is inflammation in your pancreas. Inflammation causes swelling and pain. If you have pancreatitis, it might feel like stomach pain that spreads to your back. Your pancreas is an organ in your abdomen. It sits between your stomach and your spine. If you lay your right hand across your stomach, that's roughly the size and shape of your pancreas behind it.
Your pancreas is involved in digestion and regulating your blood sugar. It makes digestive enzymes (like amylase) and hormones (like insulin). It delivers digestive enzymes to your small intestine through the pancreatic duct. Inflammation is your immune system’s response to injury. It’s supposed to help heal injured tissues. When your pancreas is injured, it’s most often from gallstones blocking the pancreatic duct, or from alcohol.
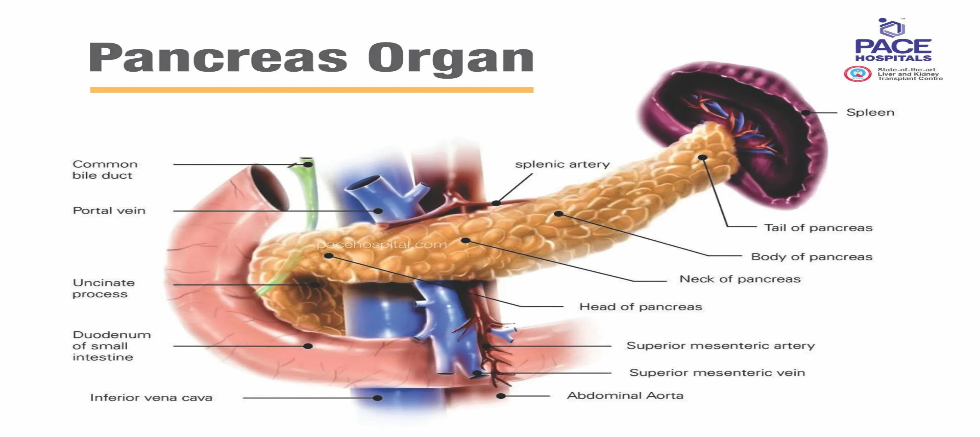
Pancreas function
The Pancreas secret pancreatic juice (a transparent fluid consists of electrolytes, water, and enzymes) that is rich in proteins and consists of bicarbonate fluid, digesting enzyme such as amylase, trypsin, nucleases, elastase, chymotrypsinogen , carboxypeptidase and lipase, these enzymes are essential for the digestion of fat, protein, fat, and carbohydrate in the food.
The pancreas performs two most important functions i.e. exocrine and endocrine function for human body -
● Exocrine function: It releases digestive enzymes to break down and digest fats, foods, carbohydrates, and proteins in our small intestine. The enzymes normally are produced and carried in an inactive form to the small intestine, where the enzymes are activated as needed. It also makes and releases bicarbonate that neutralizes stomach acids and allows for the activation of pancreatic enzymes.
● Endocrine function: it produces five hormones, beta cells secrete insulin, alpha cells secrete glucagon, delta cells secrete somatostatin, epsilon cells secrete ghrelin and PP (gamma) cells secrete pancreatic polypeptide; and releases them into the blood. These hormones regulate sugar (glucose) transport into the body's cells, where it is used for energy and to help maintain normal blood sugar levels.
TYPES OF PANCREATITIS
There are different types of conditions related to the pancreas including-
● Acute pancreatitis is a temporary condition. It happens when your pancreas is attempting to recover from a minor, short-term injury. Most people with acute pancreatitis will recover completely in a few days with supportive care: rest, hydration and pain relief. However, a very severe case of acute pancreatitis can cause serious health complications, some of them life-threatening.
● Chronic pancreatitis is a long-term, progressive condition. It doesn’t go away and gets worse over time. It happens when the injury or damage to your pancreas never stops. Chronic pancreatitis will eventually do lasting damage to your pancreas, although it may take many years. Constant inflammation causes scarring of your pancreas tissues (fibrosis), which stops them from making enzymes and hormones.
● Hereditary pancreatitis is a rare genetic condition to occur due to recurrent pancreatic attacks, which can lead to chronic pancreatitis. Symptoms include severe abdominal pain, tender and swollen belly, diarrhea, nausea, bloating, vomiting and fever. It also increases lifetime risk of pancreatic cancer. Hereditary pancreatitis can't be cured completely, can be managed by medical management, pancreatic enzyme supplements to cope-up with indigestion, insulin for diabetes, medications to control pain and lifestyle changes to reduce the risk of pancreatic cancer.
● Pancreatic cancer occurs when uncontrolled cell growth begins in the tissues of the pancreas. Cancerous and noncancerous tumors growths can occur in the pancreas. Pancreatic cancer can be cured if detected early but in most of the cases due to no symptoms is early stages it’s difficult to find it. Pancreatic cancer can also slow down the production of digestive enzymes by the pancreas, resulting in difficulty to break down food and absorbing nutrients. This malabsorption causes bloating, watery, greasy, foul-smelling stool, further can lead to weight loss and vitamin deficiencies.

Pathophysiology of Acute Pancreatitis
The pathophysiology of acute pancreatitis begins with specific triggering factors, the most common of which are gallstones and excessive alcohol consumption. Other less frequent triggers include hypertriglyceridemia, certain drugs, or direct physical trauma to the abdomen. These triggers lead to acinar cell injury, often through mechanical obstruction of the pancreatic duct, ischemia, or direct toxic effects, which disrupts the normal secretory processes of the pancreas.
A critical turning point in the mechanism is the premature activation of enzymes within the pancreas itself. Normally, trypsinogen is converted to trypsin only once it reaches the small intestine, but in pancreatitis, this conversion happens prematurely inside the pancreatic tissue. This active trypsin then triggers a cascade by activating other potent enzymes such as elastase, which damages blood vessels; phospholipase, which destroys cell membranes; and lipase, which results in fat necrosis.
This enzymatic surge leads to the autodigestion of the pancreas, where the organ effectively begins to digest its own tissue. This process ignites a massive inflammatory cascade, characterized by the release of pro-inflammatory cytokines like IL-1, IL-6. Locally, this results in significant edema, tissue necrosis, and potential hemorrhage within the pancreatic bed.
In severe cases, the inflammation is not contained locally and spills into the systemic circulation, leading to Systemic Inflammatory Response Syndrome (SIRS). This systemic involvement can result in life-threatening complications, including Acute Respiratory Distress Syndrome (ARDS), circulatory shock, and multi-organ failure. The severity of the disease is often dictated by the extent of this systemic cytokine storm rather than the local pancreatic damage alone.
Pathophysiology of Chronic Pancreatitis
The development of chronic pancreatitis is a prolonged pathological process that typically begins with a chronic injury to the pancreatic tissue. While alcohol consumption remains the most common driver, other factors such as genetic mutations, autoimmune disorders, and long-term ductal obstruction also play significant roles. These stressors initiate a cycle of persistent inflammation, which may manifest as either recurrent episodes of acute pancreatitis or a silent, continuous low-grade injury that gradually erodes the organ's structural integrity.
At the cellular level, this inflammatory environment leads to the activation of pancreatic stellate cells. Once activated, these cells shift into a myofibroblast-like state and begin to overproduce collagen and other extracellular matrix components. This process results in progressive fibrosis, where the healthy, functional parenchyma is slowly replaced by non-functional scar tissue. This structural overhaul often leads to significant ductal obstruction and the formation of characteristic calcifications within the pancreatic ducts.
The ultimate clinical consequence of these changes is a profound loss of function that affects both the exocrine and endocrine roles of the organ. Exocrine insufficiency occurs as the acinar cells are destroyed, leading to a critical decrease in digestive enzymes. This results in nutrient malabsorption and steatorrhea, which is the excretion of abnormal quantities of fat with the feces. Simultaneously, the destruction of islet cells leads to endocrine insufficiency, which manifests as diabetes mellitus because the pancreas can no longer produce adequate insulin to regulate blood glucose levels.
What are the most common causes of pancreatitis?
Gallstones and heavy alcohol consumption are the primary drivers of acute pancreatitis, accounting for approximately 80% of all clinical cases. When a gallstone migrates from the gallbladder into the common bile duct, it can become lodged at the Ampulla of Vater. This obstruction blocks the flow of pancreatic enzymes, causing a backup that triggers premature activation and subsequent inflammation within the pancreatic tissue itself.
Heavy drinking contributes to the disease through a different mechanism, primarily by causing direct toxic injury to the pancreatic acinar cells. Chronic alcohol exposure increases the protein concentration of pancreatic secretions, which can lead to the formation of small protein plugs that obstruct the minor ductules. Additionally, alcohol sensitizes the pancreas to the effects of cholecystokinin, further promoting the inappropriate intracellular activation of digestive enzymes.
While these two factors dominate the epidemiological landscape, the remaining 20% of cases arise from a diverse group of triggers. These include metabolic disturbances like hypertriglyceridemia, trauma to the abdomen, certain medications, and post-procedural complications following an endoscopic retrograde cholangiopancreatography (ERCP). Regardless of the initial cause, the final common pathway remains the autodigestion of the organ and the potential for a systemic inflammatory response.
Gallstone pancreatitis
Your common bile duct empties bile from your gallbladder into your intestine through the same opening as your pancreatic duct. If a gallstone enters the common bile duct and gets stuck at that junction, it can temporarily block the drainage of pancreatic juice from the pancreatic duct. This traps the enzymes inside your pancreas. As pressure builds up behind the obstruction, it activates the enzymes inside your pancreas and they begin digesting the pancreas itself. This causes the inflammatory response of gallstone pancreatitis.
Alcohol use
Heavy alcohol use is another clear cause of pancreatitis, though scientists aren’t sure why. It may be that the toxic byproducts of alcohol in your blood cause an inflammatory response in your pancreas, or they somehow chemically activate the digestive enzymes inside your pancreas. Scientists estimate that heavy alcohol use accounts for around half of both acute pancreatitis and chronic pancreatitis cases.
Other causes
While gallstones and alcohol dominate the clinical landscape, the remaining 20% of pancreatitis cases stem from a diverse array of less common triggers. Metabolic disturbances like hypertriglyceridemia—specifically when serum levels exceed 1000 mg/dL—and hypercalcemia can lead to the accumulation of toxic free fatty acids or calcium deposits that damage acinar cells. Genetic factors also play a role, as seen in hereditary pancreatitis caused by mutations in the $PRSS1$ gene or as a complication of cystic fibrosis, where thickened secretions obstruct the pancreatic ducts.
Infectious agents, particularly viruses like mumps, Coxsackievirus, and cytomegalovirus, can directly invade pancreatic tissue and trigger an inflammatory response. Autoimmune pancreatitis is another distinct entity where the body's own immune system attacks the organ, often characterized by a sausage-shaped enlargement of the pancreas on imaging. Structural issues such as pancreatic cancer or direct traumatic injury to the abdomen can also lead to ductal disruption and enzyme leakage.
Vascular issues like ischemia, resulting from reduced blood supply during major surgery or systemic shock, can deprive the pancreas of oxygen and lead to cell death. Furthermore, a wide variety of medications—ranging from certain diuretics to azathioprine—are known to irritate the pancreas in susceptible individuals. In some instances, even after a thorough diagnostic workup, no clear cause is identified, leading to a classification of idiopathic pancreatitis.
COMPLICATIONS
Most cases of acute pancreatitis don’t have complications, but 1 in 5 cases is more severe. It’s not clear why severe acute pancreatitis occurs in some cases and not others. A severe case can lead to serious complications, including death. Chronic pancreatitis also causes complications, but they develop more slowly and aren’t directly life-threatening. Most complications are manageable with treatment.
Acute pancreatitis
Complications of severe acute pancreatitis include:
1. Necrosis and infection. One in 3 cases of severe acute pancreatitis causes so much swelling in your pancreas that it cuts off some of the blood supply. The loss of blood supply causes tissue death (necrosis) in parts of your pancreas. Necrotic (dead) tissue is a feast for roaming bacteria. When bacteria infect these tissues, they thrive and replicate, spreading to your bloodstream. Infection in your bloodstream (septicemia) is an emergency. Your body reacts to an infection in the bloodstream by activating an immune response against the infection (systemic inflammatory response syndrome, or SIRS). This immune response can cause your blood vessels to enlarge, which leads to a drop in blood pressure (septic shock) and decreased blood flow to your vital organs. This can cause multiple organ failure.
2. Pancreatic pseudocysts. Inflammation in your pancreas can disrupt the pancreatic duct that feeds pancreatic juices to your intestine. This can cause pancreatic juices to leak out around the pancreas and cause inflammation of the surrounding tissue. Over time, the inflamed area forms a hardened capsule around the fluid, called a pseudocyst. Many pseudocysts don’t cause symptoms or need treatment. But they can occasionally become infected or become large enough to cause discomfort. Rarely, a blood vessel can erode into a pseudocyst and lead to bleeding inside the cyst. In these cases, your healthcare provider may need to intervene to drain the cyst or stop the bleeding.
3. Chronic pancreatitis. Repeat episodes of acute pancreatitis can lead to chronic pancreatitis. Constant inflammation in your pancreas eventually leads to scarring of the tissues (fibrosis). Fibrosis in your pancreas interferes with its ability to function as a gland. Over time, it produces less and less of the enzymes and hormones your body needs, leading to further complications.
Chronic pancreatitis
Complications of chronic pancreatitis develop over time and can include:
1. Exocrine pancreatic insufficiency (EPI), malabsorption and malnutrition. As fibrosis in your pancreas progresses, your pancreas produces less and less of the enzymes that your digestive system relies on. This causes the malabsorption of nutrients in your small intestine, especially fats and fat-soluble vitamins. Excess fats pass through your poop, causing fatty stools and eventually, chronic diarrhea. As you absorb less nutrition from your food, you could begin to lose weight and eventually feel the effects of the missing nutrients.
2. Hypoglycemia, hyperglycemia and Type 1 diabetes. Chronic pancreatitis will also cause your pancreas to produce less of the hormones that regulate your blood sugar (glucose). Depending on which is affected first, you may experience symptoms from a lack of glucagon, which causes hypoglycemia (low blood sugar), or from a lack of insulin, which causes hyperglycemia (high blood sugar). Eventually, both hormone supplies are depleted, and diabetes develops.
3. Chronic pain. While some people with chronic pancreatitis don’t experience pain or experience a remission of pain over time, others experience worsening pain that’s eventually constant. It can be challenging to manage, even with medication, and can affect your mental health, as well.
4. Increased risk of pancreatic cancer. Chronic inflammation is a risk factor for cancer wherever it occurs. In people with chronic pancreatitis, the risk of pancreatic adenocarcinoma is between 1% and 2%. Symptoms are similar to those of chronic pancreatitis, so they might go unnoticed. Doctors recommend that people with chronic pancreatitis have regular cancer screening.
Pancreatitis diagnosis
Pancreatitis has physical findings that affect body systems and can be diagnosed through blood test, imaging test and intervention procedure advised by doctor. Depending on symptoms, the Gastroenterologist will ask about medical history, any family history of pancreatitis, eating and drinking habits, taking any prescription or over-the-counter medications, including vitamins and supplements.
To diagnose pancreatitis, a gastroenterologist may recommend:
● Blood and Stool tests: Amylase or lipase blood test and Stool routine test for digestive enzymes of the pancreas. It will be elevated 3 times in pancreatitis from its normal range. If blood test is showing normal ranges then we need to go to further evaluation.
● Imaging tests: To understand pancreatitis and figure out what’s the cause. Doctor may recommend X-rays with a barium meal and Ultrasound imaging: specifically evaluate the gallbladder for stones
● Endoscopic ultrasound (EUS): Endoscopic examination to evaluate pancreatic masses and tumors, pancreatic cysts, small stone in bile duct and gall bladder not identified during ultrasound. This procedure is performed to collect small tissues of pancreas using FNA needle through the wall of the stomach or intestine directly into the pancreas.
● CT Scan, Magnetic resonance imaging (MRI), Magnetic resonance cholangiopancreatography (MRCP), or PET scans: Non-invasive tests for detailed imaging of the pancreas and the surrounding. CT scans expose the patient to some amount of radiation. Furthermore, some patients are unable to receive IV contrast for their CT scans (due to allergies or kidney problems), and thus the quality of the pictures will be sub-optimal. A special kind of MRI called an MRCP can give high-quality pictures of the pancreas, the pancreas duct, and the bile ducts. However, some patients who are claustrophobic may decide against having an MRI performed.
● Biopsy or Tissue analysis: a tissue sample (biopsy) from pancreas may help diagnose pancreatitis and further look for signs of pancreatitis.
● Endoscopic retrograde cholangiopancreatography (ERCP): to view the bile duct and pancreatic duct. It helps to remove gallstones from the bile duct gallstones that are causing a blockage.
Management and Treatment
How is pancreatitis treated?
Treatment depends on the cause, whether it’s acute or chronic and how severe it is. In general, you should always see a healthcare provider for symptoms of pancreatitis. Although some cases of acute pancreatitis may go away on their own, that depends on what caused the condition and how severe it is. In the meantime, most people with acute pancreatitis will need pain relief to get through it. Some people will need emergency treatment for certain causes. And some will need intensive care for complications.
Acute pancreatitis
Treatment for acute pancreatitis may include:
1. Supportive care
If the cause has been resolved and you don’t have severe or complicated pancreatitis, care will focus on supporting your body’s natural healing process. This usually includes:
● IV fluids. Pancreatitis is dehydrating, and hydration is very important for healing.
● Tube feeding. If you’re unable to tolerate food by mouth, your doctors may administer food via a tube placed through your nose or stomach to help you get enough nutrition.
● Parenteral nutrition: In very severe cases, your doctors may elect to provide nutrition through an intravenous line.
● Pain relief. You’ll have medication through an IV directly to your bloodstream or by mouth.
2. Gallstone removal
If you have gallstone pancreatitis, your provider may need to remove an impacted gallstone from your bile ducts. They’ll also recommend gallbladder removal surgery to prevent gallstones from causing you future problems. Procedures may include:
● Endoscopic retrograde cholangiopancreatography (ERCP). This procedure goes inside your bile ducts with an endoscope — a thin, flexible catheter with a camera attached. Most gallstones in your bile ducts can be removed this way. The endoscope passes down your throat and through your esophagus into your stomach and bile ducts. It sends images to a monitor. Watching the monitor, the endoscopist can insert tools through the catheter to remove gallstones.
● Gallbladder removal surgery. Once gallstones have brought you to the hospital, the chance of them causing you trouble again is high. Gallbladder removal is the standard treatment for gallstones that cause complications. It can usually be done through minimally invasive (laparoscopic) surgery. A laparoscopic cholecystectomy removes your gallbladder through a few small incisions, using the aid of a laparoscope, and a tiny camera is inserted through one of the incisions. Some people may require traditional open surgery depending on their condition.
3. Additional support
If you have complications, you may also need:
● Antibiotics.
● Procedures to drain fluid or remove dead tissue.
● Intensive care.
Chronic pancreatitis
If you have chronic pancreatitis, your general healthcare provider may refer you to a specialist (gastroenterologist). Treatment for chronic pancreatitis begins with pain management and lifestyle changes to slow down the progression of the disease. Eventually, you may need enzyme supplements and insulin injections to replace the enzymes and insulin your pancreas no longer produces.
1. Lifestyle changes
If you have chronic pancreatitis, it’s paramount that you quit drinking alcohol and quit smoking. These factors both contribute greatly to pancreatitis and will speed up the progression of the disease. Your healthcare provider can connect you with resources to help you quit. It’s also important to maintain a low-fat diet with plenty of fruits and vegetables and to drink plenty of water each day.
2. Pain management
Long-term pain management can be complex. You may need to experiment with a variety of different medications and procedures to find what works for you. Make sure to stay in touch with your healthcare provider about your pain, especially if what you’re doing isn’t working. They can refer you to a chronic pain specialist to help you manage your pain. In some cases, endoscopic procedures to remove scar tissue or pancreas stones may improve your symptoms. Injection of local anesthetic agents into the nerves of the pancreas (celiac plexus block) is another option for selected patients.
3. Supplements
Over time, many people with chronic pancreatitis can develop exocrine pancreatic insufficiency (EPI). These people will need to take pancreatic enzymes in supplement form. You might also need to take nutritional supplements to get enough calories and micronutrients (vitamins and minerals). Some people will develop glucose intolerance and eventually diabetes, becoming insulin-dependent.
4. Surgery
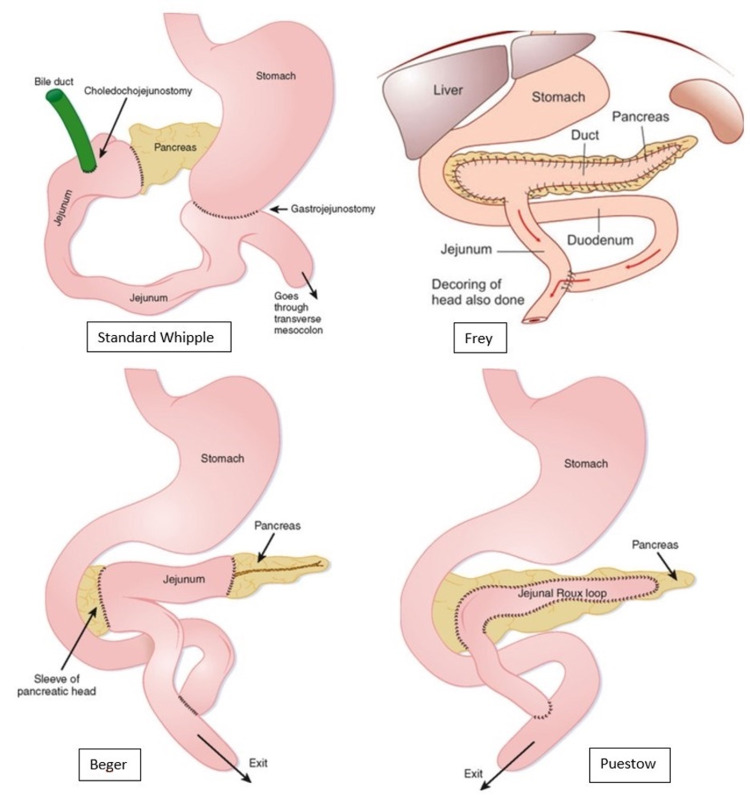
Approximately 40% to 75% of patients suffering from CP will require surgery at some point during the course of their disease to alleviate symptoms of pain. The Puestow procedure, also known as a longitudinal pancreatojejunostomy, is the treatment of choice in patients with CP, a dilated pancreatic duct, no inflammatory mass, and abstinence from alcohol for more than one year. This surgical procedure is done via the creation of an opening along the anterior surface of the pancreas from the head extending as far into the tail as possible, after which, calcified stones are removed and a Roux-en-Y jejunostomy is attached to the sides of the pancreas. Traditionally, the Puestow procedure was done through an open incision; however, recent advancements have made it possible to perform this procedure through laparoscopic and robotic techniques. The procedure is associated with a morbidity and mortality rate of about 1%, and pain relief if reported in up to 80% of patients.
The Frey and Beger procedures were developed with the underlying notion that the head of the pancreas functions like a pacemaker for pain in CP. The Frey procedure consists of excising the anterior head of the pancreas, including the major and minor pancreatic ducts and the duct of Santorini, with preservation of the posterior pancreatic head and the pancreatic neck. Additionally, the main pancreatic duct is opened, and a Roux-en-Y limb is brought up to complete a pancreatojejunostomy. Studies have shown that post-operative morbidity in the Frey procedure ranges from 7.5% to 39%, with mortality rates ranging from 0% and 2.4% A recent study of patients who underwent a Frey procedure found that over 90% of patients had full alleviation of pain
Beger’s procedure is notorious for being one of the first procedures that consist of a pancreatic head resection while still being able to preserve the duodenum. Beger’s procedure is also referred to as duodenum-preserving pancreatic head resection (DPPHR). This procedure is done by first preserving the posterior branch of the gastroduodenal artery, which supplies the duodenum, the intrapancreatic segment of the CBD, and the pancreaticoduodenal groove .Next, there is resection of the neck and head of the pancreas, specifically at the area superimposing the portal vein and SMV, with a conscious effort to preserve pancreatic tissue present at the innermost portion of the duodenum .A study on the outcomes of Beger’s procedure revealed that 91.7% of patients reported being pain-free after a median of 5.7 years. Beger’s procedure has been found to be efficacious in patients with inflammatory masses at the head of the pancreas .While Frey’s procedure also addresses disease associated with a head mass, the inability to rule out malignancy is an absolute contraindication for performing Frey’s procedure .Beger’s procedure avoids major surgical resection of the CBD, duodenum, and portal vein and circumvents the need to restore bile flow, food passage, and portal blood flow, while still preserving the endocrine function of the pancreas .Frey’s procedure is generally considered to be simpler than Beger’s; however, studies comparing both procedures have shown no differences in postoperative morbidity, pain relief, exocrine insufficiency, and quality of life .
A distal pancreatectomy is indicated for those with distal pancreatic disease and simultaneous small duct diameter, as well as for those who have undergone a failed Puestow procedure, those with a pseudoaneurysm in the pancreatic tail, portal hypertension secondary to small duct disease, or suspicion of malignancy in the pancreatic tail .This procedure is associated with the risk of symptomatic recurrence, with long-term relief achieved in only 60% of patients, and complete pancreatectomy needed in 13% of patients. Furthermore, approximately half of patients also develop exocrine and endocrine insufficiency. Historically, the Whipple operation, or a pancreaticoduodenectomy, was the gold standard procedure for managing CP. However, in recent times, the Whipple procedure is used almost exclusively for resectable pancreatic ductal adenocarcinomas, rather than for CP . Although the Whipple operation was shown to be effective in the treatment of pain, there was evidence of significant long-term morbidity and complications. A study conducted by Izbicki et al. showed that two years after surgery, the rate of in-hospital complication for patients who underwent the Whipple operation was 53.3%, compared with 19.4% in those who underwent the Frey procedure. Furthermore, global quality of life improved by 71% in those who underwent the Frey procedure, compared to 43% in those who underwent the Whipple procedure.
In a meta-analysis, it was determined that both the short- and long-term outcomes of the Berger and Frey procedures regarding the global quality of life were ominously better than the Whipple procedure. A pictorial overview of the aforementioned surgical procedures is depicted in Figure 1. The last resort procedure is a total pancreatectomy, which is associated with severe morbidity secondary to brittle diabetes and lethal episodes of hypoglycemia.
Figure 3. Depiction of the final gross anatomical changes associated with the Whipple, Frey, Beger, and Puestow procedures.
Prevention
Ways to prevent pancreatitis may include:
● Prevent or manage gallstones. Take steps to prevent gallstones by maintaining a healthy weight and eating a balanced diet. If you have a history of gallstones, your healthcare professional may recommend removing your gallbladder.
● Avoid alcohol and cigarettes. Drinking alcohol and smoking cigarettes increases the risk of pancreatitis
● Avoid certain medicines. Some medicines increase the risk of pancreatitis. Talk with your healthcare professional about the medicines you take.
● Eat a balanced diet. Eat vegetables, fruit, whole grains and lean proteins. Avoid foods that are high in fat.
● Stay hydrated. Drinking enough water helps with digestion and gallbladder function.
Summary
Pancreatitis is inflammation of the pancreas. Acute pancreatitis refers to sudden inflammation that often causes severe pain, while chronic pancreatitis develops more gradually. An individual experiencing severe abdominal pain should connect with a healthcare professional or seek immediate medical attention. Early diagnosis and treatment are crucial for relieving pain and inflammation associated with acute pancreatitis. It is not possible to reverse the damage or inflammation from chronic pancreatitis, but regular treatment can help manage symptoms and prevent complications from worsening.
REFERENCE
1. https://www.mayoclinic.org/diseases-conditions/pancreatitis/symptoms-causes/syc-20360227
2 https://www.pacehospital.com/pancreatitis-acute-and-chronic-symptoms-causes-and-treatment
3. https://my.clevelandclinic.org/health/diseases/8103-pancreatitishttps://pmc.ncbi.nlm.nih.gov/articles/PMC8684888/
4. https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/breaking-down-pancreatitis
5. https://pmc.ncbi.nlm.nih.gov/articles/PMC8684888/