
Diabetes Mellitus in Children: A Comprehensive Research Overview
1. Gulnaz Osmonova
2. Mahboob Alam
(1, Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Student, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
Abstract
Diabetes mellitus (DM) in children represents a significant and growing public health challenge worldwide. While Type 1 diabetes mellitus (T1DM) has historically been the predominant phenotype in the pediatric population, the incidence of Type 2 diabetes mellitus (T2DM) in youth has risen sharply over the past two decades. This review synthesizes recent data on the epidemiology, pathophysiology, clinical features, diagnosis, complications, and management of diabetes in children. Emphasis is placed on differentiating etiologies, understanding risk factors, and outlining evidence-based approaches to care.
Keywords: Pediatric diabetes; Type 1 DM; Type 2 DM; Hyperglycemia; Insulin deficiency; Insulin resistance; DKA; Hypoglycemia; Childhood obesity; Insulin therapy; HbA1c; CGM; Complications
Introduction
Diabetes mellitus is defined by chronic hyperglycemia resulting from impaired insulin secretion, insulin action, or both. In children, T1DM — an autoimmune destruction of pancreatic β-cells leading to absolute insulin deficiency — remains the most common form. However, T2DM, previously considered an adult disease, is now increasingly diagnosed in children due to the rising global prevalence of obesity and sedentary lifestyles.
Diabetes mellitus (DM) in children is a chronic metabolic disease characterized by elevated blood glucose levels due to insulin deficiency and/or insulin resistance. It presents unique clinical challenges in pediatric populations and significantly impacts growth, development, and quality of life
Types and Epidemiology
Types of Pediatric Diabetes
Type 1 Diabetes Mellitus (T1D)
Autoimmune destruction of pancreatic β-cells leads to an absolute deficiency of insulin.
Most common type in children, historically the dominant form of pediatric diabetes.
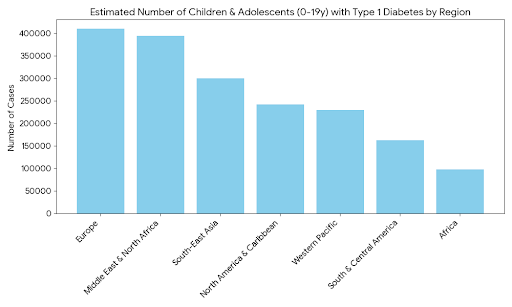
Global Regional Prevalence (Type 1 Diabetes)
Europe and the Middle East/North Africa (MENA) regions currently report the highest absolute numbers of children living with Type 1 Diabetes (T1D). Southeast Asia also shows a significant burden, largely driven by high case numbers in India (estimated at over 300,000 cases in children).
Type 2 Diabetes Mellitus (T2D)
Characterized predominantly by insulin resistance, often in the context of obesity, with a relative insulin secretory defect.
Incidence in pediatric age groups is rising sharply alongside global increases in childhood obesity.
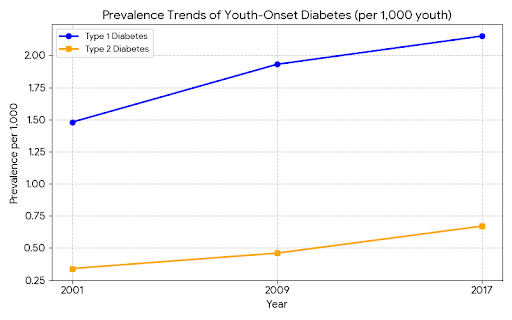
Prevalence Trends: Type 1 vs. Type 2
While Type 1 Diabetes remains more common in children, the prevalence of youth-onset Type 2 Diabetes (T2D) is rising at a steeper rate. In the United States, T1D prevalence rose from 1.48 to 2.15 per 1,000 youth between 2001 and 2017, while T2D grew from 0.34 to 0.67 per 1,000.
Monogenic Diabetes (e.g., MODY)
Rare genetic forms of diabetes due to single-gene defects affecting β-cell function.
Frequently misdiagnosed as type 1 or type 2 diabetes unless genetic testing is performed.
Distribution of Diabetes Types
In the pediatric and young adult population (ages 0–25), Type 1 Diabetes accounts for approximately 80% of all cases. Type 2 Diabetes makes up about 15%, with the remaining cases consisting of Monogenic Diabetes (MODY) or secondary forms of the disease.
Neonatal Diabetes
Very rare, presents in the first 6 months of life; can be transient or permanent
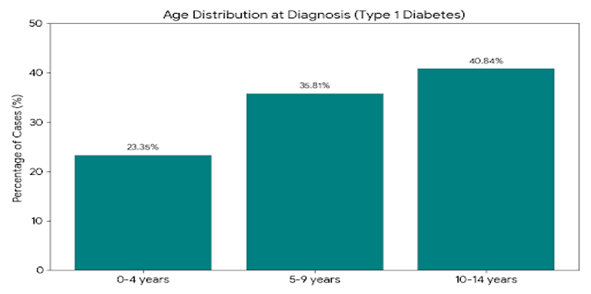
Age Distribution at Diagnosis
Type 1 Diabetes is most frequently diagnosed in early adolescence. Statistics show that roughly 41% of pediatric diagnoses occur between the ages of 10 and 14, while younger children (0–4 years) account for about 23% of new cases.
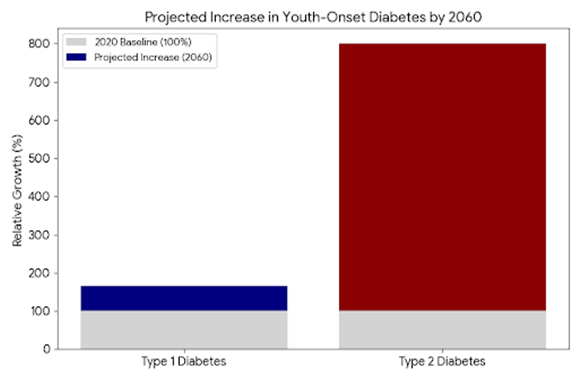
Future Projections (2060)
The CDC and other health organizations project a significant "awakening epidemic." If current trends continue, the number of children with T1D could increase by 65% by 2060, while cases of youth-onset T2D could skyrocket by nearly 700%, largely linked to rising childhood obesity and environmental factors.
Key points:
T2DM prevalence mirrors childhood obesity rates.
T2DM often presents in adolescence and is associated with metabolic syndrome feature.
Pathophysiology
T1DM
T1DM is an autoimmune condition marked by immune-mediated destruction of β-cells, resulting in insufficient insulin production and hyperglycemia. Genetic predisposition and environmental triggers — including viral exposures — contribute to disease onset.
T2DM
T2DM is characterized by peripheral *insulin resistance* and relative β-cell dysfunction. Obesity and sedentary lifestyle exacerbate insulin resistance, while genetic and intrauterine factors may predispose children to early disease. ([PubMed][8])
Mechanisms include:
Insulin resistance in muscle and adipose tissue.
β-cell dysfunction and inadequate insulin secretion.
Clinical Presentation
Symptoms
Symptoms of diabetes in children can include:
Polyuria (excessive urination)
Polydipsia (increased thirst)
Weight loss
Fatigue
In T1DM: signs of DKA (nausea, vomiting, abdominal pain)
Differential Diagnosis
Accurate classification between T1DM, T2DM, and rarer monogenic forms (e.g., MODY) is critical given implications for therapy and prognosis.
Diagnosis
Diagnosis in children follows standard glucose and HbA1c criteria:
Fasting plasma glucose ≥126 mg/dL or
HbA1c ≥6.5% (details may vary by guideline)
Additional tests include:
Autoantibody panels (to support T1DM)
C-peptide levels
Genetic testing when monogenic diabetes is suspected.
Complications
Both T1DM and T2DM in childhood carry risks for acute and long-term complications:
Acute
DKA is more common in T1DM at presentation.
Chronic
Microvascular complications (retinopathy, nephropathy, neuropathy)
Macrovascular disease (cardiovascular risk)
Poorly controlled T2DM diagnosed in youth may accelerate complication onset relative to adult-onset disease.
Management Strategies
Management goals for pediatric diabetes include optimizing glycemic control, preventing complications, and supporting psychosocial wellbeing.
T1DM
Insulin therapy remains the mainstay, often via multiple daily injections or insulin pumps.
Continuous Glucose Monitoring (CGM) and advanced hybrid closed-loop systems improve glycemic metrics like Time in Range (TIR).
T2DM
Lifestyle modification (diet and exercise) is foundational.
Metformin and, in some cases, insulin or other pharmacotherapy are used.
Multidisciplinary Care
Comprehensive care teams — including endocrinologists, dietitians, and psychosocial support — are essential for effective long-term management.
Prevention and Public Health Implications
Public health initiatives targeting childhood obesity, physical activity promotion, and early screening in high-risk populations are critical to curtail the rise of T2DM in youth.
Future Directions
Emerging research areas include predictive modeling for risk stratification, technologies for hypoglycemia prediction, and personalized therapy approaches grounded in genetic and biomarker data.
Conclusion
Diabetes mellitus in children encompasses a spectrum of disorders with distinct pathophysiologies and clinical trajectories. T1DM remains the most common form but the global surge in T2DM among youth highlights the need for vigilant screening, early diagnosis, and tailored management strategies. Advances in monitoring technologies, multidisciplinary care, and preventive public health strategies are essential to improving outcomes for children with diabetes.
References.
1.Type 2 Diabetes Mellitus in Children: Epidemiology & Management — Review focusing on the rise of T2DM in youth.
2.Type 2 Diabetes Mellitus in Children: Primary Care & Public Health Considerations — JAMA perspective on pathophysiology and prevention.
3.Children and Adolescents with Type 1 and Type 2 Diabetes in PDC Registries — Comparative clinical characteristics and glycemic control.
4.Diabetes Mellitus in Children and Adolescents — Classic review with trends in type 1 vs type 2 diabetes
5.Etiologic Distribution & Clinical Characteristics of Pediatric Diabetes — Cohort study of multiple DM types in children.
6.Parents’ Experiences of Caring for a Young Child with T1D: Systematic Review — Qualitative evidence on psychosocial impact.
7.Diabetes Mellitus in Children — Int. Journal of Medical Research & Insights — Holistic clinical overview including technology and guidelines.
8.Pediatric Diabetes Incidence Trends & Obesity Correlation — Historical overview of trends.
9.ISPAD Clinical Practice Consensus Guidelines: Type 2 Diabetes in Children & Adolescents — Authoritative guideline reference.
10.Genetic & Monogenic Determinants of Early Onset Diabetes — Insight into non-classic diabetes subtypes (MODY).