
Systemic Lupus Erythematous
1. Samatbek Turdaliev
2. Anumol
Attoor Sanjith
(1. Teacher, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.
2. Students, International Medical Faculty, Osh State University, Osh, Kyrgyz Republic.)
ABSTRACT
Systemic lupus erythematous (SLE) is a multifactorial autoimmune disease characterized by multisystem involvement and significant clinical and serological heterogeneity. Its pathogenesis involves genetic, epigenetic, environmental, and ecological factors leading to deregulated innate and adaptive immune responses, auto reactive B-cell activation, and immune complex deposition in tissues. Clinical manifestations range from mild, self-limiting symptoms to severe, life-threatening organ damage, making diagnosis challenging. Antinuclear antibodies are present in over 95% of patients and serve as a key serological marker. The updated EULAR classification criteria have improved diagnostic accuracy. Current management strategies aim to achieve remission, prevent irreversible organ damage, and enhance patients’ quality of life.
KEYWORS: Systemic Lupus Erythematous, pathogenesis, epigenetic, autoimmune disease, multisystem involvement, genetic susceptibility, EULAR classification criteria.
INTRODUCTION
Systemic lupus erythematous (SLE) is a multisystem chronic autoimmune disease with a relapsing and remitting course. Its prevalence is higher in women of childbearing age, with a female predominance of 9:1 [1] . This striking sex bias strongly implicates sex hormones (especially estrogen), X chromosome-linked immune regulatory genes, and epigenetic mechanisms in disease pathogenesis. The observation that the gender ratio narrows before puberty and after menopause further supports a hormonal influence.
Furthermore, other autoantibodies might be present in SLE patients, such as anti-Scl-70 antibodies (present in systemic sclerosis), anti-La, and anti-Ro antibodies (present in Sjogren disease), anticardiolipin antibodies, and anti-phospholipid antibodies thus indicating a wide association between SLE and other autoimmune diseases[2]. These findings highlight the immunologic overlap between SLE and other systemic autoimmune diseases, underscoring the concept of systemic autoimmune rheumatic disorders.
REVIEW
Globally, the reported incidence and prevalence of SLE differ significantly by geography, with North America reporting the highest incidence and prevalence, Africa reporting the lowest incidence, and Australia reporting the lowest prevalence. Age, gender, and ethnicity play a significant role in determining the clinical outcome and management of the disease. SLE is more prevalent in the female population, but its course is more critical and expeditious in men, which culminates in a bad prognosis[3] . Global variations in the incidence and prevalence of SLE are well documented and reflect a complex interplay of genetic susceptibility, environmental exposures, socioeconomic factors, access to healthcare, and diagnostic practices. North America consistently reports the highest incidence and prevalence, likely due to higher proportions of genetically susceptible populations (e.g., Afro American and Hispanic ancestry), better disease recognition, and robust reporting systems.
Age, gender, and ethnicity play a critical role in disease expression, severity and outcomes. While SLE most commonly affects women-particularly during reproductive years- the disease course in men is often more severe and rapidly progressive. Male patients are more likely to present with renal, neurologic, and cardiovascular involvement, higher disease activity at diagnosis, and delayed recognition.
Globally, the reported incidence and prevalence of SLE differ significantly by geography, with North America reporting the highest incidence and prevalence, Africa reporting the lowest incidence, and Australia reporting the lowest prevalence. Age, gender, and ethnicity play a significant role in determining the clinical outcome and management of the disease. SLE is more prevalent in the female population, but its course is more critical and expeditious in men, which culminates in a bad prognosis[4]. The pathogenesis of systemic lupus erythematous is best explained by a multifunctional model involving dynamic interactions between genetic susceptibility, environmental exposures (the exposome), and epigenetic modifications. Genome-wide association studies have identified numerous susceptibility loci related to immune regulation, including genes involved in type I interferon signalling, complement pathways, and lymphocyte activation. However, genetic predisposition alone is insufficient to cause disease.
Environmental factors such as ultraviolet B (UVB) radiation, infections (particularly viral infections), and chemical or drug exposures act as triggers in genetically predisposed individuals. These factors induce epigenetic changes- including DNA hypomethylation, histone modification, and altered microRNA expression- which dysregulate immune-related gene expression. UVB exposure promotes keratinocyte apoptosis and the release of nuclear antigens, while infection activate innate immune pathways through toll-like receptors, collectively contributing to the breakdown of central and peripheral immune tolerance.
In the last decade, a genome-wide association study (GWAS) has mapped >90 SLE susceptibility loci, with many single nucleotide polymorphisms acting additively. In addition, rare monogenic forms of SLE have also been reported[5]. Among the 730 SLE-associated polymorphisms, 21 lead to amino acid change, 484 exist within gene coding regions, and the rest are inter-genic, suggesting a significant effect on gene regulation instead of protein sequence[6]. Generally, the observation that only a small fraction of SLE-associated variants result in amino-acid substitutions, while the majority are located within intronic or inter-genic regions, strongly indicates that disease risk is driven mainly by altered gene regulation rather than changes in protein structure. These regulatory variants influence gene expression through effects on enhancers, promoters, transcription factor binding sites, and epigenetic marks, particularly within immune-related pathways such as type I interferon signalling, B cell activation, T-cell costimulation and complement regulation.
The susceptibility genes involved in aberrant T/B cell signalling in SLE encode adaptor molecules, kinases, and cytokines that regulate T/B-cell activation, proliferation, and interaction. For example, the class II human leukocyte antigen (HLA) region encodes molecules involved in antigen presentation[7]. Susceptibility genes involved in systemic lupus erythematous largely affect aberrant T- and B- cell signalling pathways and encode adaptor molecules, kinases, transcription factors, and cytokines that regulate lymphocyte activation, proliferation, differentiation, and intercellular interactions. Variants in these genes lower immune activation thresholds and impair regulatory mechanisms, thereby promoting the survival and expansion of auto reactive lymphocytes. Notably, the class II human leukocyte antigen (HLA) region represents one of the strongest genetic associations with SLE and encodes molecules essential for antigen presentation to CD4+T cells. Certain HLA class II alleles enhance the presentation of self-antigens, facilitating auto reactive T-cell activation and pathogenic T-B cell collaboration, which ultimately drives autoantibody production and immune-mediated tissue injury.
T cells play a significant role in SLE pathogenesis, driving inflammation by secretion of pro-inflammatory cytokines, inducing B cells to generate autoantibodies, and maintaining disease via a pool of auto reactive memory T cells. However, the ratios of some T cell subsets and their function are abnormal in patients with SLE[8]. T cells play a pivotal role in the pathogenesis of systemic lupus erythematous by orchestrating immune dysregulation at multiple levels. Aberrantly activated CD4+T helper cells promote inflammation through the excessive secretion of pro-inflammatory cytokines and provide inappropriate help to B cells, thereby driving the production of pathogenic autoantibodies. In addition, the persistence of auto-reactive memory T cells contribute to disease chronicity and relapse, even during periods of clinical remission.
T follicular helper (Tfh) cells are essential for germinal centre induction, proliferation, and isotope switching, and somatic hyper mutation. In addition, these cells produce cytokine IL-21, which induces B cell differentiation into memory B cells and antibody-generating plasmablasts. Pathological expansion of Tfh cells in SLE is directed by the interaction of the Tfh cells with the OX40 ligand expressed on myeloid antigen-presenting cells[9].
The expression of the OX40 ligand is induced by TLR7 activation from circulating RNA-containing immune complexes. This pathologic expansion of the TFH cell subset contributes to enhanced antibody production and loss of tolerance in SLE patients[10].
B cells contribute to the pathogenesis of SLE through their response to antigens and autoantibody production. The pathways implicated in the aberrant activation of B cells include the toll-like receptor (TLR) pathway, stimulation via beta cell-activating factor (BAAF), and B-cell receptor (BCR) mediated activation. The stimulation of B cells through the TLR pathway promotes loss of tolerance[11].
BCR- Mediated Activation
Engagement of auto-reactive BCRs by nuclear antigens.
Leads to internalization of antigen and downstream signalling.
Alone, the signal is often insufficient requires co-stimulation
TLR pathway
Endosomal TLR7 (RNA) AND TLR9 (DNA) recognize self-nucleic acids
Immune complexes containing nucleic acids are internalized via Fc receptors.
Simultaneous BCR + TLR signalling powerfully activates auto-reactive B cells.
Transitional B cells are susceptible to TLR9 stimulation and produce autoreactive marginal zone B cells, as seen in SLE patients. An impairment of B cell tolerance can also occur through B cell stimulation from cytokines, particularly BAFF. SLE patients with high levels of BAFF exhibit significantly higher levels of anti-dsDNA, anti-histone, and anticardiolipin antibodies[12].
Transitional B cells constitute a critical peripheral tolerance checkpoint. In systemic lupus erythematous (SLE), aberrant stimulation of transitional B cells through endosomal Toll-like receptor 9 (TLR9) by self DNA containing immune complexes allows autoreactive B cells to escape deletion and preferentially differentiate into marginal zone B cells. In addition, increased levels of the cytokine B-cell activating factor (BAFF) further impair B-cell tolerance by promoting the survival and expansion of autoreactive B-cell clones. Elevated BAFF levels in SLE patients correlate with increased production of pathogenic autoantibodies, including anti-dsDNA, anti-histone, and anticardiolipin antibodies, thereby contributing to disease activity and progression.
Aberrant Apoptotic Cell Clearance
Dysregulation of apoptosis and nuclear debris clearance contributes to an increase in autoantigen exposure. Several pathways evolve to prevent immune activation in response to endogenous cellular debris, but these mechanisms are impaired in SLE[13]. Under physiological conditions, apoptotic cells are rapidly cleared in an immunologically silent manner by phagocytes, with multiple regulatory pathways preventing immune activation against self-derived cellular debris. In SLE, impairment of these clearance mechanisms leads to the persistence of apoptotic material, which is taken up by antigen-presenting cells and recognized by innate immune receptors, resulting in loss of self-tolerance. This promotes activation of autoreactive B and T cells, sustained autoantibody production, and chronic inflammation characteristics of the disease.
The downstream activation of TAM receptors promotes the phagocytosis of apoptotic cells. In addition, it inhibits the signal transducer and activator of transcription 1 (STAT1) and the nuclear factor kappa-light-chain-enhancer of the activated B cell (NF-κB) pathway. In animal studies, TAM knockout has been associated with the presence of anti-dsDNA antibodies, anti-phospholipid antibodies, and SLE-like manifestations, such as arthritis, vasculitis, and the deposition of immunoglobulin G in renal glomeruli[14].
TAM receptor signalling is crucial for the efficient phagocytosis of apoptotic cells (efferocytosis), thereby limiting the persistence of nuclear debris and potential autoantigens. Beyond debris clearance, TAM activation exerts a potent immunoregulatory function by supressing pro-inflammatory signalling pathways, notably STAT1 and NF-Kb, which are central to type I interferon responses and inflammatory gene transcription. Experimental studies in TAM- deficient animals demonstrate that loss of the regulatory pathway resulted in defective clearance of apoptotic material, heightened immune activation, and the development of lupus-like autoimmunity. The presence of anti-dsDNA and antiphospholipid antibodies, along with clinical features such as arthritis, vasculitis, and IgG deposition in renal glomeruli, closely mirrors human SLE, underscoring the critical role of TAM receptors in maintaining self- tolerance and preventing systemic autoimmunity.
C-reactive protein (CRP) can bind to the nuclear antigens of apoptotic bodies and neutralize their immunogenicity potential. Single nucleotide polymorphism of the CRP gene, mainly CRP4, is linked with low serum CRP levels and SLE. In addition, DNase I contributes to the degradation of chromatin released from apoptotic cells, reducing exposure of nuclear antigens to the immune cells. A loss-of-function variant in the DNASE1L3 gene is associated with a familial form of SLE[15].
C- reactive protein plays an important role in maintaining immune tolerance by binding to nuclear antigens exposed on apoptotic bodies, thereby opsonizing them for non-inflammatory clearance and neutralizing their immunogenic potential. Genetic polymorphisms in the CRP gene, particularly the CRP4 variant, are associated with reduced serum CRP levels and increased susceptibility to SLE, highlighting the protective role of CRP in limiting autoimmunity. In parallel, extracellular DNases such as DNase I and DNASE1L3 are essential for degrading chromatin released from apoptotic and necrotic cells, preventing the accumulation of immunostimulatory DNA. Loss of function mutations in DNASE1L3 impair chromatin clearance and are strongly associated with familial and early-onset SLE, leading to enhanced exposure of nuclear antigens, activation of autoreactive immune responses, and sustained autoantibody production.
Complement dysfunction is proposed to accelerate several steps in the pathogenic pathways of SLE, such as impaired clearance of apoptotic debris and IC, increased autoreactive CD+8 T cell activity, and tissue damage by activation of the inflammatory cascade in organs with IC deposition[16]. C1q typically assists in the removal of apoptotic material and immune complexes and inhibits the CD8+ T cell response to self-antigens by modulating their mitochondrial metabolism. Patients with C1q homozygous deficiency develop autoantibodies and a lupus-like syndrome, evidently due to the inability to eliminate apoptotic cells[17].
Complement dysfunction, particularly involving early components such as C1q, accelerates multiple pathogenic steps in SLE. Under normal conditions, C1q binds to apoptotic cells and immune complexes, promoting their efficient clearance in an immunologically silent manner and preventing the accumulation of nuclear auto-antigens. In addition to its role in debris clearance, C1q exerts important immunoregulatory effects by supressing autoreactive CD+T –cell responses, partly through modulation of mitochondrial metabolism and limiting pro-inflammatory activation. In patients with homozygous C1q deficiency, failure to eliminate apoptotic material and immune complexes leads to persistent autoantigen exposures, loss of self-tolerance, autoantibody formation, and the development of a lupus-like syndrome. Furthermore, defective complement regulation enhances immune-complex-mediated inflammation, resulting in tissue damage in organs such as the kidneys, skin, and blood vessels.
Particulate Exposure
Experimental studies suggest that crystalline silica induces cellular apoptosis and the release of intracellular antigens. Other disease mechanisms include increased activity of pro-inflammatory cytokines, oxidative stress, and diminished regulatory T-cell activity. In murine models, silica exposure is linked with higher serum autoantibodies and immune complexes[18].
Crystalline silica is recognised as an environmental factor that can initiate or exacerbate systemic autoimmunity. It induces apoptosis in various cell types, leading to the release of intracellular antigens that can act as autoantigens, thereby promoting loss of tolerance. In addition, silica exposure triggers pro-inflammatory cytokine production, generates oxidative stress, and impairs regulatory T-cell function, all of which amplify autoreactive immune responses. Experimental murine models demonstrate that silica exposure leads to elevated serum levels of autoantibodies and circulating immune complexes, mirroring the humoral autoimmunity seen in SLE. These findings underscore how environmental agents can interact with genetic susceptibility to drive disease onset or progression.
Exposure to toxic components from cigarette smoke (e.g., nicotine, polycyclic aromatic hydrocarbons, carbon monoxide, and free radicals) can induce oxidative stress and directly damage endogenous proteins and DNA, leading to genetic mutations that potentially induce autoimmunity and augment the production of pro-inflammatory cytokines[19]. A meta-analysis of studies on smoking and SLE risk revealed that smokers had an increased risk of developing SLE (OR 1.5; 95% CI 1.09, 2.08) compared to non-smokers[20].
Cigarette smoke contains multiple toxic components- such as nicotine, polyclinic aromatic hydrocarbons, carbon monoxide, and free radicals- that induce oxidative stress, directly damage DNA and proteins, and promote genetic and epigenetic alterations. These changes can break immune tolerance, trigger autoimmunity, and increase the production of pro-inflammatory cytokines, creating a milieu conductive to systemic autoimmunity. Epidemiological data support this mechanistic link: a meta-analysis shows that smokers have a significantly increased risk of developing SLE (OR 1.5; 95 % Cl 1.09-2.08) compared to non-smokers. This demonstrates that environmental exposures, like cigarette smoke, act synergistically with genetic predisposition to trigger to exacerbate SLE.
Antinuclear antibody (ANA), hematological and immunological disorders, arthritis, and cutaneous manifestations were among the most presented symptoms of PL syndrome. Therefore, a significant proportion of preclinical lupus (approximately 10% to 20%) often transitions to SLE. Most PL patients are treated with steroids and other immunosuppressive therapies such as azathioprine and methotrexate. The most prevalent clinical presentations are summarized below
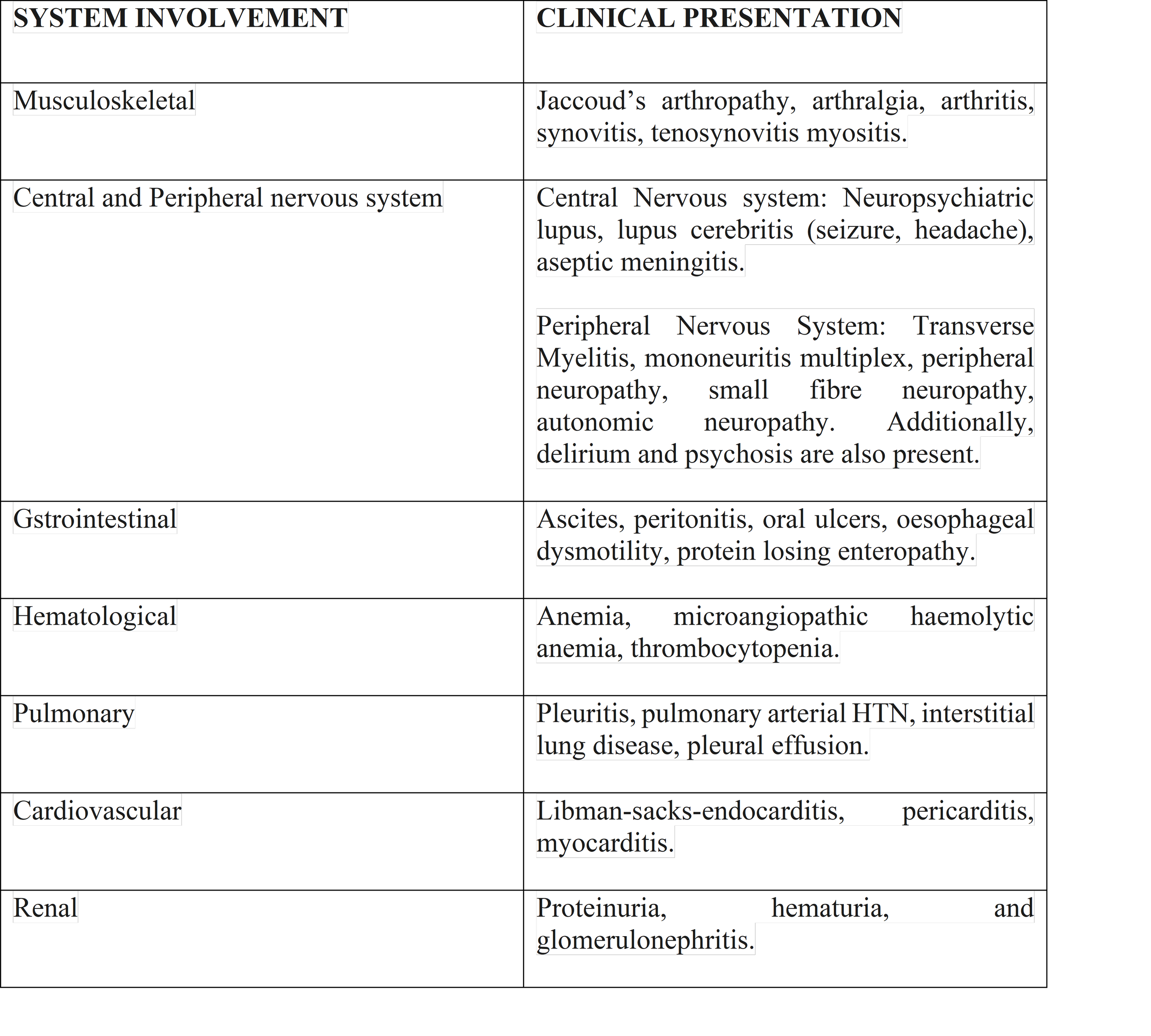
Cardiovascular System
All three layers of the heart, namely the pericardium, myocardium, and endocardium, and often, coronary circulation, may be affected in SLE. The frequently seen manifestations include cardiomyopathy, valvular diseases, rhythm discrepancies, and heart failure. The most prevalent cardiac manifestation is pericarditis secondary to exudative pericardial effusions[1].
SLE can affect all three layers of the heart- pericardium, myocardium, and endocardium- ad well as the coronary circulation, reflecting its systemic autoimmune nature. Cardiac manifestations are diverse: pericarditis is the most common, often presenting with exudative pericardial effusions, myocarditis can lead to cardiomyopathy and heart failure; valvular involvmemtn may cause thickening or libman-sacks endocarditis; and cionduction abnormalities can produce arrhythmias. These manifestations result from a combination of immune complex deposition, complement activation, and chronic inflammation, and they contribute significantly to morbidity in SLE. Early recognition is essential, as some complications, such as pericardial tamponade or severe cardiomyopathy, can be life-threatening.
Gastrointestinal System
A vast array of gastrointestinal (GI) symptoms are also observed in SLE, including flatulence, diarrhea, abdominal cramps, hematemesis, gastric atony, duodenal and jejunal ileus, chronic ulcerative colitis, oral ulcers, esophageal dysmotility issues, protein-losing enteropathy, and lupus enteritis. Moreover, mesenteric vessel thrombosis, Budd-Chiari syndrome, and hepatic veno-occlusive disease also occur secondary to SLE and anti-phospholipid antibody syndrome[2].
Functional symptoms such as flatulence, diarrhoea, abdominal cramps, gastric intestinal vasculitis and myopathy, while mucosal immune injury explains oral ulcers, hematemesis, and chronic colitis. More specific entities like protein-losing enteropathy and lupus enteritis- typically involving the jejunum and ileum- are closely linked to active disease and are usually steroid- responsive if recognised early. In parallel, the presence of antiphospholipd antibodies predisposes to mesenteric vessel thrombosis and hepatic vascular disorders such as Budd-Chiari syndrome and veno-occulsive disease, undergoing that GI manifestations in SLE may represent either inflammatory activity or life-threatening thrombotic complications and therefore demand prompt evaluation.
Hematological Syndrome
Around 18% to 80% of patients with SLE suffer from anemia. Anemia of chronic disease is the most prevalent type encountered in SLE. Microangiopathic hemolytic anemia, iron deficiency anemia, coomb's positive autoimmune hemolytic anemia, red blood cell aplasia, anemia secondary to chronic renal disease, and pancytopenia are also seen in SLE. Autoimmune cytopenia is not infrequent in SLE owing to the presence of antigens in the blood vessel compartment, resulting in more production of antibodies[3].
The above mentioned statement appropriately reflects that anaemia and other cytopenias are common hematologic manifestations of SLE, predominantly due to anaemia of chronic disease but also encompassing immune-mediated hemolyis, marrow suppression, renal involvement, and antibody-driven autoimmune cytopenias resulting from deregulated immune responses against blood cell antigens.
Musculoskeletal System
Musculoskeletal manifestations such as arthralgia and arthritis are present in 80% to 90% of patients with SLE. Though any joint can be affected most commonly, there is symmetrical involvement of small joints such as hands, wrists, and knees. The condition is aptly named lupus arthritis[4].
It is also known as Jaccoud's arthropathy. SLE arthritis might have a similar presentation to rheumatoid arthritis, including ulnar deviation and subluxation of the metacarpophalangeal joints, and the term "ruphus" has been coined to represent this condition. Rarely, cases of avascular necrosis of the hip joint with bilateral involvement have also been reported[5].
Lupus arthritis is classically deforming but reducible, as seen in Jaccoud’s arthropathy, distinguishing it from rheumatoid arthritis despite overlapping features such as ulnar deviation and MCP subluxation; however, the coexistence of true erosive changes in some patients has led to the term “rhupus” to denote an RA-SLE overlap. Additionally, avascular necrosis of the hip, often bilateral, though uncommon, is a clinically significant complication, frequently related to chronic corticosteroid use and cumulative disease activity.
Nervous System
The central and peripheral nervous system involvement and psychiatric symptoms are often seen in SLE. Often headache is the most frequently encountered symptom. Additionally, there is an increased risk for ischemic stroke in SLE patients compared to the general population. Cognitive dysfunction is another significant concern in SLE patients, as different studies showed a cognitive decline in these patients. Seizures, aseptic meningitis, demyelinating syndrome, and movement disorder are other CNS manifestations. Complications associated with the parasympathetic nervous system include autonomic neuropathies, mononeuritis multiplex, and central and peripheral neuropathies. Psychiatric symptoms include anxiety, depression, and psychosis[6].
Pulmonary System
One of the most frequent seen pulmonary symptoms includes pleuritis, pleural effusion, acute reversible hypoxemia, pulmonary embolism, obstructive lung disease, and upper airway disease. Pulmonary arterial hypertension is another grave complication of SLE. Other pulmonary conditions associated with SLE are lupus pneumonitis, interstitial lung disease, and usual interstitial pneumonia and diffuse alveolar haemorrhage, and pulmonary embolism[7].
Renal System
One of SLE’s most prevalent and recognised clinical presentations is lupus nephritis. It is one of the earliest manifestations of SLE and occurs in around 50% of patients. Interstitial nephritis and thrombotic angiopathy are among the other renal manifestations which can be attributed to a surge of inflammatory cytokine profiles, for example, interleukins (IL-1, IL-6, IL-17, IL-18), tumour necrotic factor, Th1 and Th2 cytokines[8]. However, for completeness and academic rigor, it is worth emphasizing that immune complex deposition with subsequent complement activation remains the central pathogenic mechanism in lupus nephritis, while cytokine dysregulation acts as a key amplifier of renal inflammation and disease progression rather than the primary initiating factor.
Initially, proteinuria usually raises the suspicion of renal involvement. A wide range of manifestations (including mild presentation of sub-nephrotic proteinuria) may lead to diffuse involvement of renal structures, resulting in progressive of renal involvement are lupus nephrits, including hematuria, raised creatinine, lower limb edema, anascara, and new onset of hypertension.
Lupus nephritis (LN) is classified into six categories based on renal biopsy results. It includes glomerular immune complexes deposition, infiltration of renal parenchyma by cells and macrophages, and activation of toll-like receptors leading to elevated levels of antibodies and interferons. Different stages of renal manifestation of SLE and their prognosis are listed below.
Diagnosis
SLE presents with a wide array of clinical manifestations and an expansive profile of autoantibodies. This clinical and serological heterogeneity makes it a great challenge to reach an accurate diagnosis. Therefore, physician acumen plays a pivotal role in diagnosing SLE since various clinical features, serological findings, imaging, and histopathology must be considered simultaneously.
Classification Criteria
Several classification criteria for SLE have been formulated with the primary goal of grouping individuals for clinical studies. Furthermore, these can provide a backbone for the diagnostic approach in an individual patient[9].
Each criterion is built on the previous sets by refining, adding, or new information. The major limitation of the 1997 ACR as diagnostic criteria was a low sensitivity of 83%. According to this classification, one in six patients of SLE would not be correctly classified, with sensitivity dropping to 66% early in the disease, because criteria items may need time to accumulate during disease, which was a further limitation to using 1997 ACR as a diagnostic criterion. To rectify this, the 2012 SLICC was introduced with improved sensitivity of 97% and an increase in sensitivity to 84% early in the disease. However, the specifity decreased to 84%, whereas ACR criteria specificity was 93%[10] .
Management
Systemic lupus erythematosus is a disease of heterogenic manifestation involving multiple organs; therefore, the disase severity and organ involvement vary from patient to patient, thus posting a significant challenge in disease management and require an interdisciplinary approach. The treatment aims to prevent the flare-ups of the disease, promote remission and maintenance, and prevent relapse at a minimum cost of side effects of the drugs used[11].
Treatment decisions in SLE are guided by the level of disease activity, which is assessed using standardized scoring systems. Since the publication of the EULAR guidelines in 2008, significant advances have improved disease management. Commonly used disease activity indices include SLEDAI-2K, SLAQ, PGA, BILAG-2004, and LFA-REAL, while irreversible organ damage is evaluated using damage indices such as the SLICC/ACR Damage Index and the Brief Index of Lupus Damage. These tools are essential for guiding therapeutic choices and monitoring response, as SLEDAI scores classify disease activity (0 = remission; 1–5 = mild; 6–10 = moderate), with a change of ≥3 points indicating either a disease flare or meaningful improvement with treatment.
Goal of Treatment
The goal of treatment is to get optimum control of symptoms and remission of the disease, improve long-term outcomes for the patient, prevent end organ damage, and better quality of life for the patient. The definition of an acceptable remission state in SLE includes a SLEDAI score of 3 or less than three antimalarial, PGA of 1 or less than 1 with less than or equal to 7.5 mg of predinisone. Therefore, the first line of drugs for the SLE maintenance phase is antimalarial, the most common of which is hydroxyquinone. In acute phases, intravenous prednisolone is used, which might be later tapered off gradually and replaced by an immunosuppressant or antimalarial, depending on the disease severity.
Glucocorticoids are central to the management of SLE flares, with the goal of inducing remission followed by dose tapering to a maintenance dose of ≤7.5 mg/day to minimize adverse effects, often in combination with hydroxychloroquine or immunosuppressants. High-dose intravenous methylprednisolone is reserved for acute, organ-threatening disease. Early introduction of immunosuppressive therapy helps reduce disease flares and long-term glucocorticoid exposure, particularly when antimalarials alone provide insufficient control. Immunosuppressants such as methotrexate and azathioprine are used in patients with inadequate response or frequent relapses, while mycophenolate mofetil and cyclophosphamide are typically reserved for severe or organ-threatening disease, with drug selection influenced by disease manifestations, age, and pregnancy considerations.
Biologic therapies, including belimumab and rituximab, target B-cell pathways and are considered in patients with high disease activity or extra-renal manifestations who fail conventional therapy, particularly when glucocorticoids cannot be safely tapered. Emerging agents such as litifilimab have shown promise in early trials but require further validation. NSAIDs are used for serositis and musculoskeletal symptoms, while low-dose aspirin is indicated for thrombosis prevention in patients with antiphospholipid antibodies. Additional non-pharmacological options, such as IVIG and plasmapheresis, are reserved for severe, refractory, or life-threatening manifestations, though their cost-effectiveness and long-term benefits remain less well established compared with immunosuppressive and biologic therapies.
Conclusion
The management and long-term complications of lupus markedly improved in the last two decades, but still, there are a lot of unanswered questions regarding the disease. Current research is on its way, and further randomized connt5rol trials are needed in order to excellent compliance and commitment. Poor drug compliance, lack of monitoring, and reassessing the disease activity usually lead to poor outcomes, frequent relapses, and resistance cases. Patients should be counselled regarding the disease pathology, signs and symptoms, the need for regular monitoring, medication compliance, and preventive measure such as lifestyle changes, dietary modification, and regular exercise to control weight and lipid levels and prevent cardiovascular complications.
REFERENCES
Justiz Vaillant AA, Goyal A, Varacallo M. Treasure Island: StatPearls Publishing; 2022. Systemic Lupus Erythematosus
Autoantibodies associated with connective tissue diseases: what meaning for clinicians? Didier K, Bolko L, Giusti D, Toquet S, Robbins A, Antonicelli F, Servettaz A. Front Immunol. 2018;9:541. doi: 10.3389/fimmu.2018.00541.
The worldwide incidence and prevalence of systemic lupus erythematosus: a systematic review of epidemiological studies. Rees F, Doherty M, Grainge MJ, Lanyon P, Zhang W. https://pubmed.ncbi.nlm.nih.gov/28968809/ Rheumatology (Oxford) 2017;56:1945–1961. doi: 10.1093/rheumatology/kex260.
Abnormal B cell development in systemic lupus erythematosus: what the genetics tell us. Karrar S, Cunninghame Graham DS. https://pubmed.ncbi.nlm.nih.gov/29207444/ Arthritis Rheumatol. 2018;70:496–507. doi: 10.1002/art.40396.
Deng Y, Tsao BP. Dubois' Lupus Erythematosus and Related Syndromes (Ninth Edition) London: Elsevier; 2019. Genetics of human SLE; pp. 54–68.
Genetic predisposition to lupus across ancestries has >300 separable genetic contributions: what we know today. Laurynenka V, Kottyan LC, Weirauch MT, Kaufman KM, Harley JB. Lupus Sci Med. 2021
The pathology of T cells in systemic lupus erythematosus. Mak A, Kow NY. https://pubmed.ncbi.nlm.nih.gov/24864268/ J Immunol Res. 2014;2014:419029. doi: 10.1155/2014/419029.
T cells in systemic lupus erythematosus. Suárez-Fueyo A, Bradley SJ, Tsokos GC. Curr Opin Immunol. 2016;43:32–38. doi: 10.1016/j.coi.2016.09.001.
Clinical relevance of T follicular helper cells in systemic lupus erythematosus. Nakayamada S, Tanaka Y. Expert Rev Clin Immunol. 2021;17:1143–1150. doi: 10.1080/1744666X.2021.1976146.
ew insights into the immunopathogenesis of systemic lupus erythematosus. Tsokos GC, Lo MS, Costa Reis P, Sullivan KE. http://pubmed.ncbi.nlm.nih.gov/27872476/ Nat Rev Rheumatol. 2016;12:716–730. doi: 10.1038/nrrheum.2016.186.
Abnormal B cell development in systemic lupus erythematosus: what the genetics tell us. Karrar S, Cunninghame Graham DS. https://pubmed.ncbi.nlm.nih.gov/29207444/ Arthritis Rheumatol. 2018;70:496–507. doi: 10.1002/art.40396
New insights into the immunopathogenesis of systemic lupus erythematosus. Tsokos GC, Lo MS, Costa Reis P, Sullivan KE. http://pubmed.ncbi.nlm.nih.gov/27872476/ Nat Rev Rheumatol. 2016;12:716–730. doi: 10.1038/nrrheum.2016.186.
Disturbances of apoptotic cell clearance in systemic lupus erythematosus. Shao WH, Cohen PL. Arthritis Res Ther. 2011;13:202. doi: 10.1186/ar3206.
Incomplete clearance of apoptotic cells in systemic lupus erythematosus: pathogenic role and potential biomarker. Jung JY, Suh CH. https://onlinelibrary.wiley.com/doi/full/10.1111/1756-185X.12568. Int J Rheum Dis. 2015;18:294–303. doi: 10.1111/1756-185X.12568.
Loss-of-function variant in DNASE1L3 causes a familial form of systemic lupus erythematosus. Al-Mayouf SM, Sunker A, Abdwani R, et al. Nat Genet. 2011;43:1186–1188. doi: 10.1038/ng.975.
Mechanisms of disease: the complement system and the pathogenesis of systemic lupus erythematosus. Cook HT, Botto M. https://pubmed.ncbi.nlm.nih.gov/16932712/ Nat Clin Pract Rheumatol. 2006;2:330–337. doi: 10.1038/ncprheum0191.
The complement system in systemic lupus erythematosus: an update. Leffler J, Bengtsson AA, Blom AM. http://pubmed.ncbi.nlm.nih.gov/24845390/ Ann Rheum Dis. 2014;73:1601–1606. doi: 10.1136/annrheumdis-2014-205287.
Silica accelerated systemic autoimmune disease in lupus-prone New Zealand mixed mice. Brown JM, Archer AJ, Pfau JC, Holian A. https://pubmed.ncbi.nlm.nih.gov/12605693/ Clin Exp Immunol. 2003;131:415–421. doi: 10.1046/j.1365-2249.2003.02094.x.
Environmental and occupational exposures in the development of systemic lupus erythematosus in adults: a narrative review. Monteiro BG, Pizarro CB. Rheumatology. 2022:61.
Cigarette smoking and the risk of systemic lupus erythematosus: a meta-analysis. Costenbader KH, Kim DJ, Peerzada J, Lockman S, Nobles-Knight D, Petri M, Karlson EW. https://pubmed.ncbi.nlm.nih.gov/15022327/ Arthritis Rheum. 2004;50:849–857. doi: 10.1002/art.20049.
A meta-analysis of cardiovascular events in systemic lupus erythematosus. Gu MM, Wang XP, Cheng QY, Zhao YL, Zhang TP, Li BZ, Ye DQ. https://www.tandfonline.com/doi/abs/10.1080/08820139.2019.1567534. Immunol Invest. 2019;48:505–520. doi: 10.1080/08820139.2019.1567534.
Gastrointestinal manifestations in systemic lupus erythematosus. Fawzy M, Edrees A, Okasha H, El Ashmaui A, Ragab G. https://journals.sagepub.com/doi/abs/10.1177/0961203316642308. Lupus. 2016;25:1456–1462. doi: 10.1177/0961203316642308.
Haematological manifestations of systemic lupus erythematosus. Keeling DM, Isenberg DA. https://pubmed.ncbi.nlm.nih.gov/8130682/ Blood Rev. 1993;7:199–207. doi: 10.1016/0268-960x(93)90006-p.
Lupus arthritis. Grossman JM. https://pubmed.ncbi.nlm.nih.gov/19591780/ Best Pract Res Clin Rheumatol. 2009;23:495–506. doi: 10.1016/j.berh.2009.04.003.
Musculoskeletal manifestations of systemic lupus erythmatosus. Mahmoud K, Zayat A, Vital EM. https://pubmed.ncbi.nlm.nih.gov/28661935/ Curr Opin Rheumatol. 2017;29:486–492. doi: 10.1097/BOR.0000000000000421.
Neuropsychiatric lupus: new mechanistic insights and future treatment directions. Schwartz N, Stock AD, Putterman C. https://www.nature.com/articles/s41584-018-0156-8#citeas. Nat Rev Rheumatol. 2019;15:137–152. doi: 10.1038/s41584-018-0156-8.
Pulmonary manifestations in late versus early systemic lupus erythematosus: a systematic review and meta-analysis. Medlin JL, Hansen KE, McCoy SS, Bartels CM.
Cytokine expression in lupus kidneys. Aringer M, Smolen JS. https://pubmed.ncbi.nlm.nih.gov/15732282/ . Lupus. 2005;14:13–18. doi: 10.1191/0961203305lu2053oa.
2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Aringer M, Costenbader K, Daikh D, et al. Arthritis Rheumatol. 2019;71:1400–1412. doi: 10.1002/art.40930.
Evaluating the performance of ACR, SLICC and EULAR/ACR classification criteria in childhood onset systemic lupus erythematosus. Abdwani R, Al Masroori E, Abdullah E, Al Abrawi S, Al-Zakwani I. https://pubmed.ncbi.nlm.nih.gov/34503539/ Pediatr Rheumatol Online J. 2021;19:141. doi: 10.1186/s12969-021-00619-w.
2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Fanouriakis A, Kostopoulou M, Alunno A, et al. https://pubmed.ncbi.nlm.nih.gov/30926722/ Ann Rheum Dis. 2019;78:736–745. doi: 10.1136/annrheumdis-2019-215089.